Small sharp spikes, further comment and case
Aug 13, 2025Roland made the point at the bottom of this post Small sharp spikes; wading into the controversy. that small sharp spikes are often missed on bipolar montages and are particularly noticeable on referential montages. This is an important issue, both in respect of distinguishing them from inter-ictal epileptiform discharges and in respect of the pitfalls of referential montages. So, if they are low in amplitude, barely visible or not visible on bipolar montages, please avoid calling them inter-ictal epileptiform discharges. They may be very conspicuous on referential montages and, if this is your preferred montage when reading EEGs, you best raise your threshold when considering calling apiculate waves "spikes" and double check the waveform on bipolar montages. Know your foe. If you read EEGs on bipolar montage as your default, you likely won't be troubled by them.
Here is an example. 30+ years old. His/her father had epilepsy. The patient was investigated for drug-resistant seizures. The EEG recording was normal For 4 consecutive days, with discontinuation of antiseizure medication. Innumerable seizures were recorded, with unambiguous evidence for the diagnosis of functional seizures. The patient was counselled and discharged, with referral for psychological therapy. No further seizures occurred until 4 months ago. There have been 4 probable tonic-clonic seizures over the past 4 months, some of which were preceded by myoclonic movements by minutes to 3 hours. A tray was dropped. Hospitalization was preceded by the occurrence of more to agree about seizures. 5 days later the patient became psychotic. The patient was brought to hospital and a routine EEG was normal. The psychosis resolved after 5 days, during which time intramuscular therapy only was possible. A clinical diagnosis of probable juvenile myoclonic epilepsy was made. A 24-hour video-EEG recording was possible following the resolution of the psychosis. The EEG was normal during wakefulness. The pages presented here are from sleep.
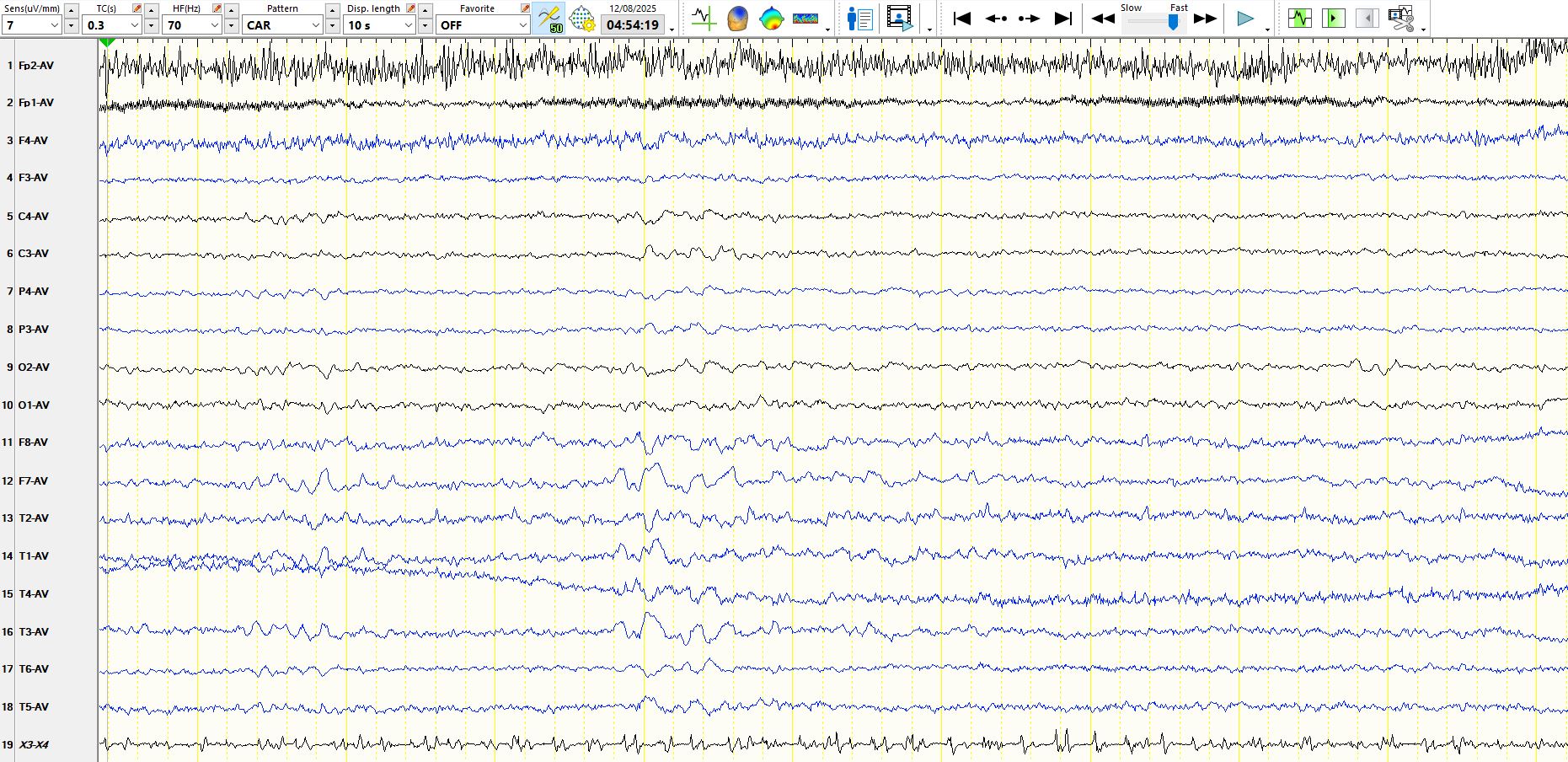
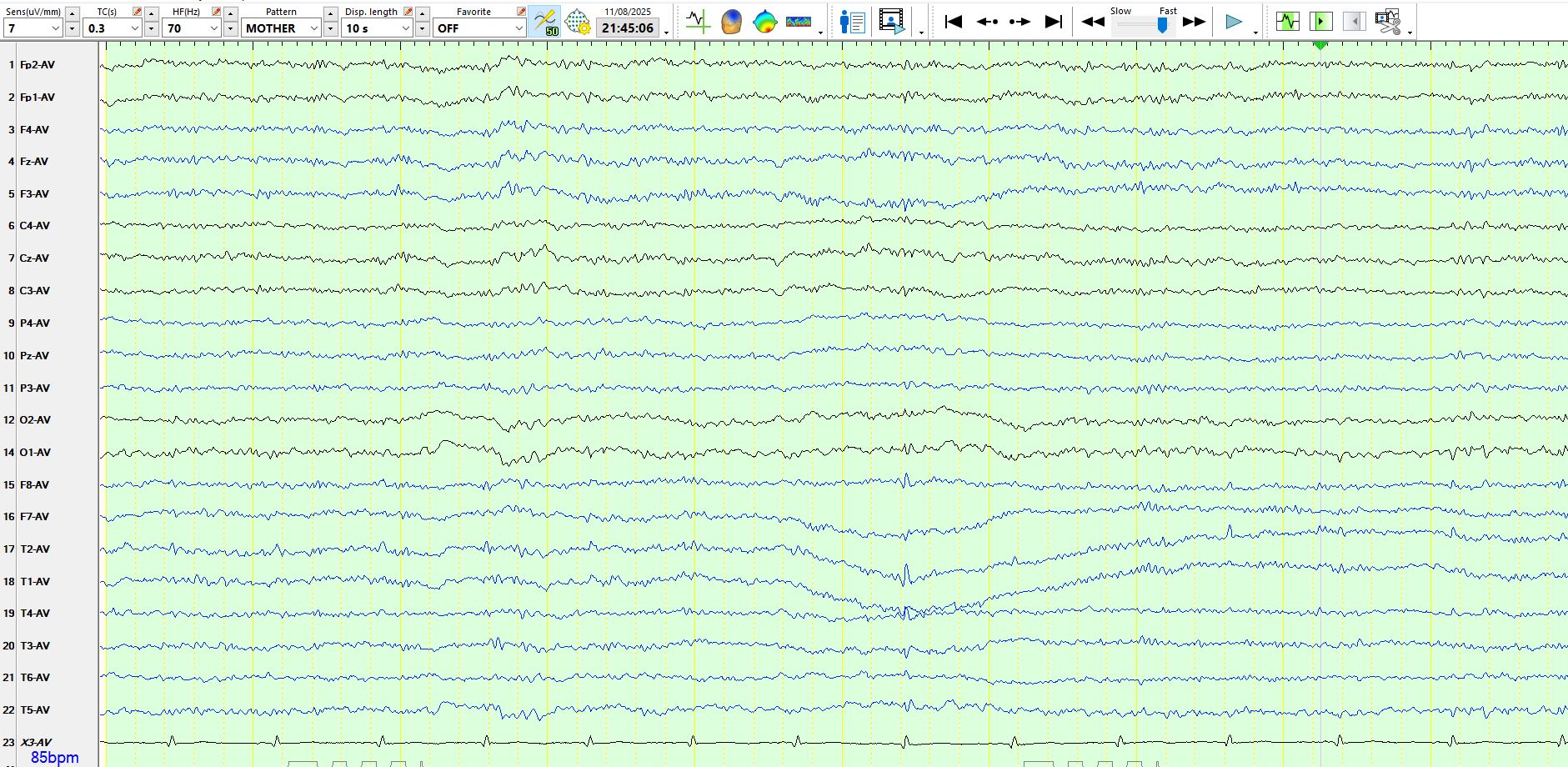
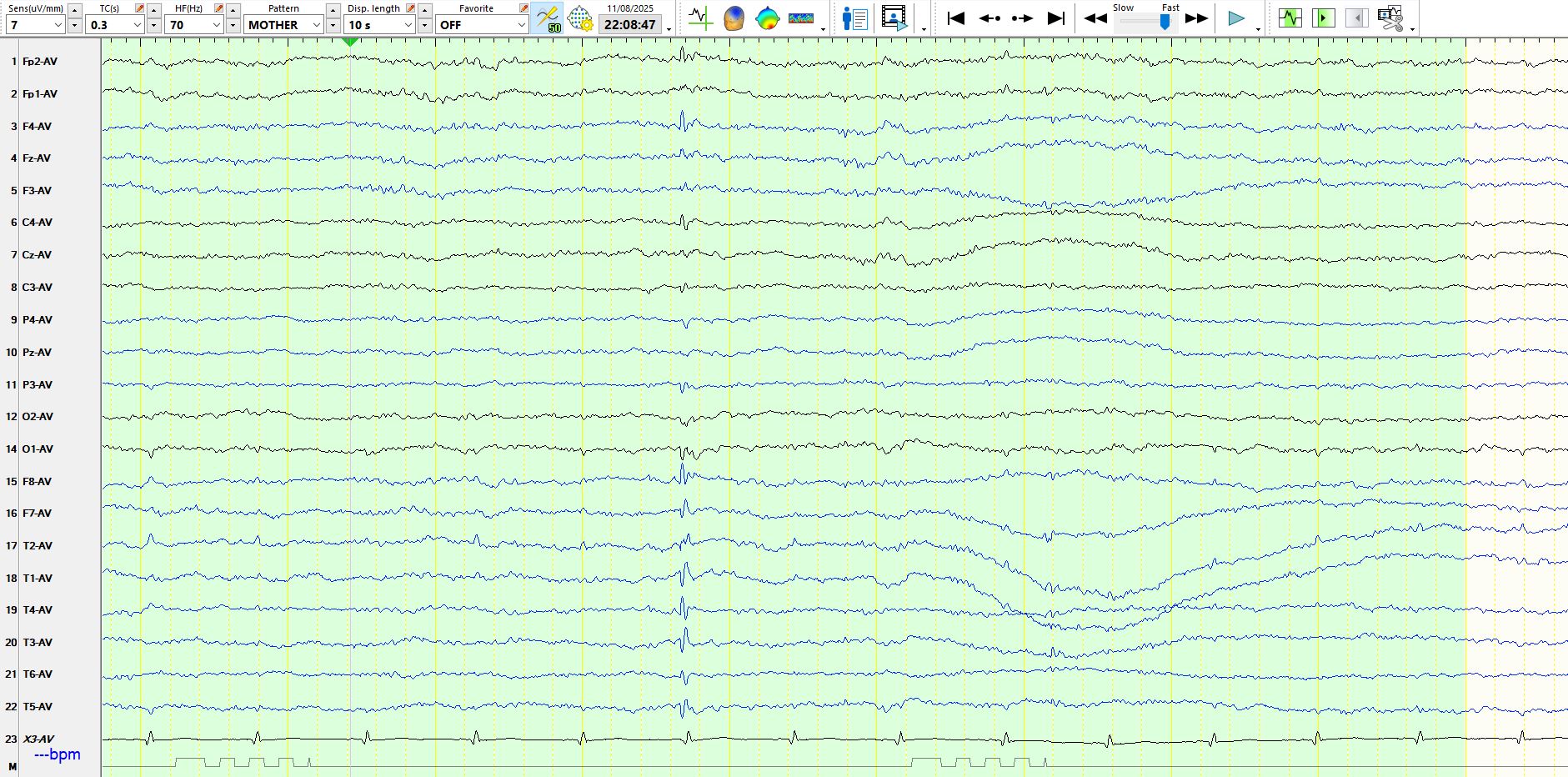
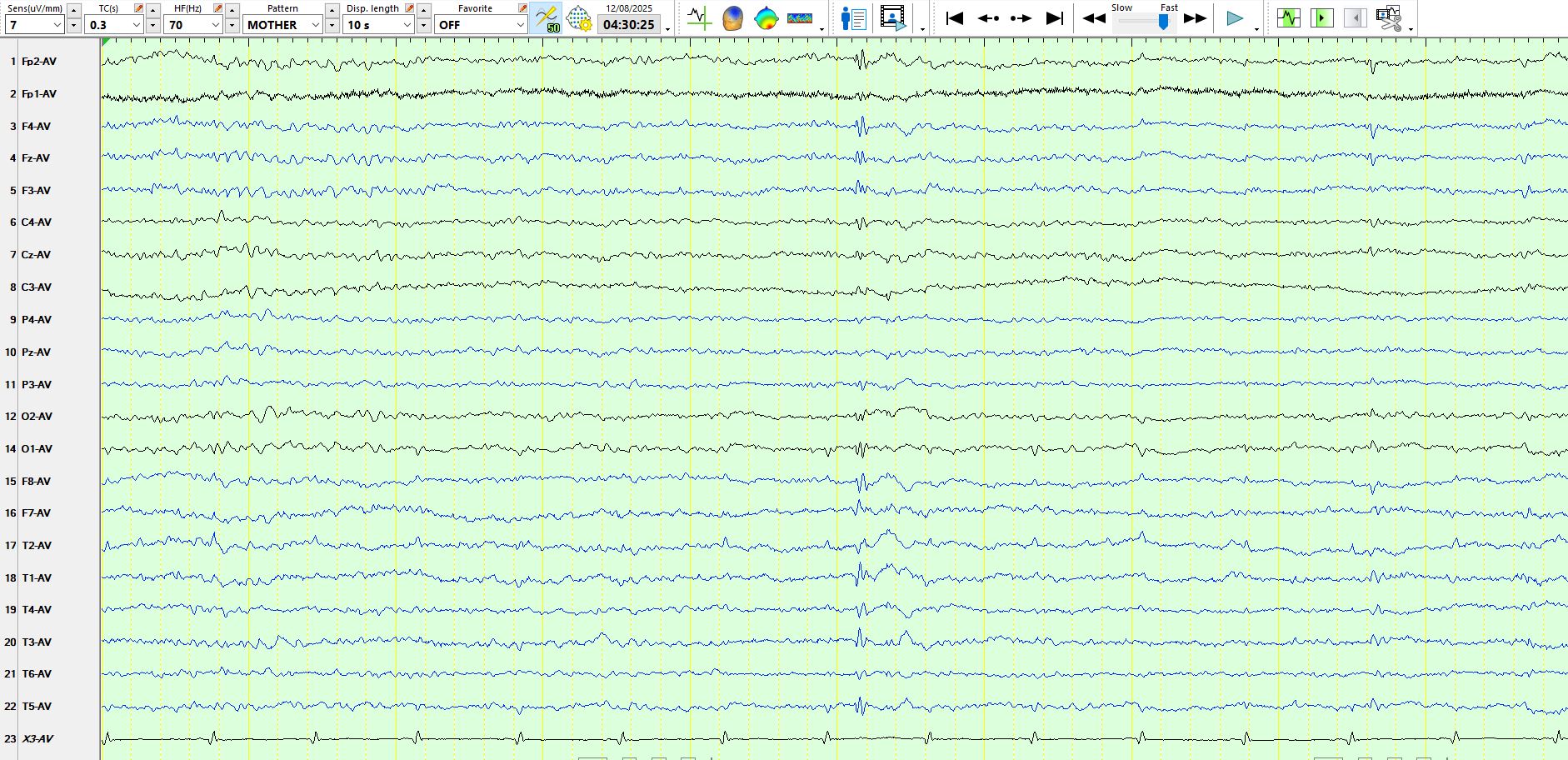
The following few pages demonstrate typical small sharp spikes in sleep on a referential montage; they have the characteristic morphology, distribution and amplitude of SSS and there is lack of a succeeding slow-wave.
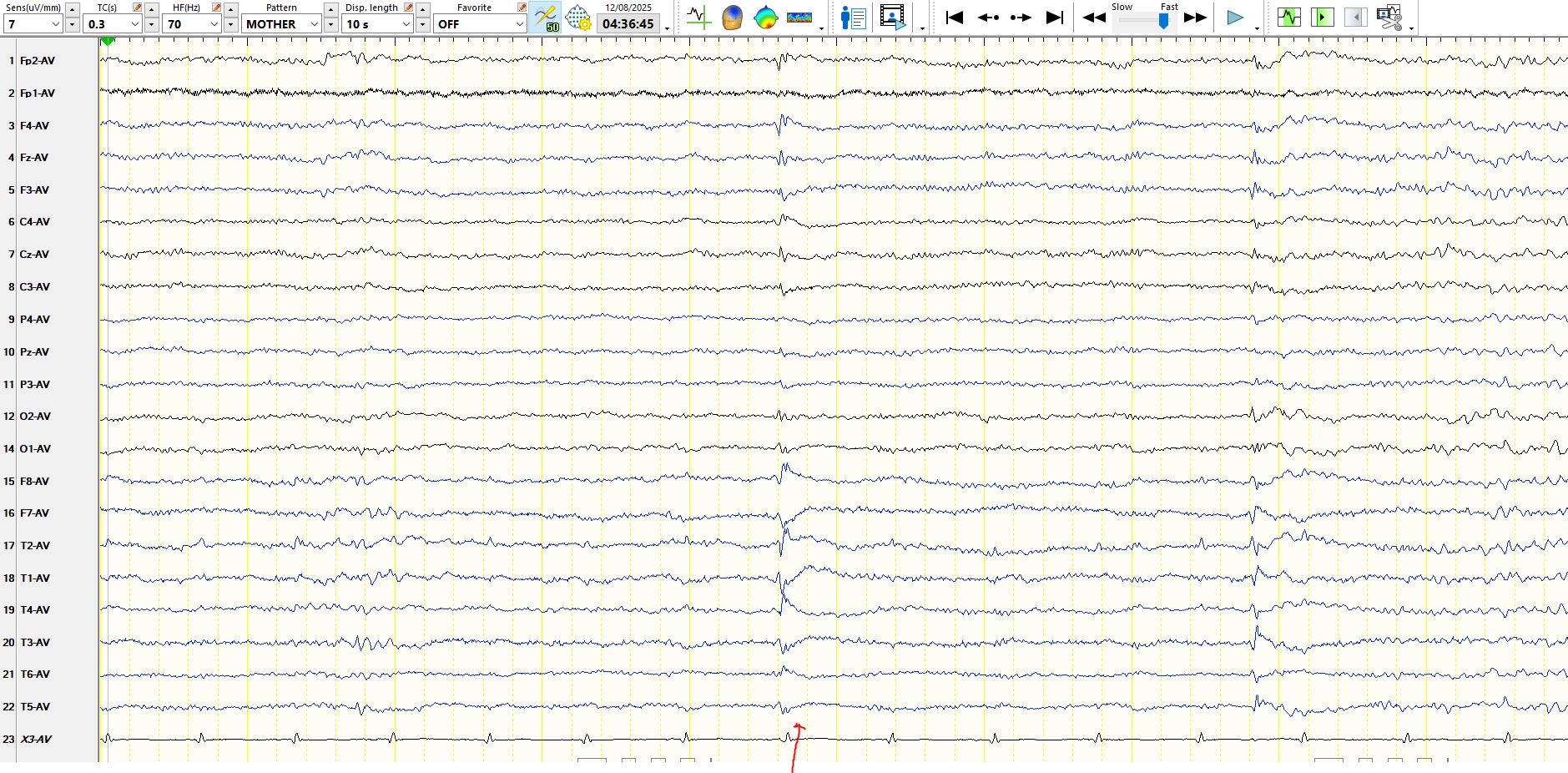
In the above image, the discharge corresponding to the 8th ECG beat likely does not represent a wave that is entirely attributable to the ECG. There are waves of variable amplitude in F7, M1, M2, 01 , that are due to ECG artefact (See above the 11th and 13th ECG beats), while some derivations, such as T3 and T4, have no such ECG artefacts. The wave corresponding to the 8th ECG beat is low in amplitude and biphasic and has a large field, likely representing a small sharp spike, probably with a small contribution from the ECG in some of the derivations. The above wave is so low in amplitude that you need not worry about it on the referential montage, especially given its shape and the lack of a succeeding slow-wave.

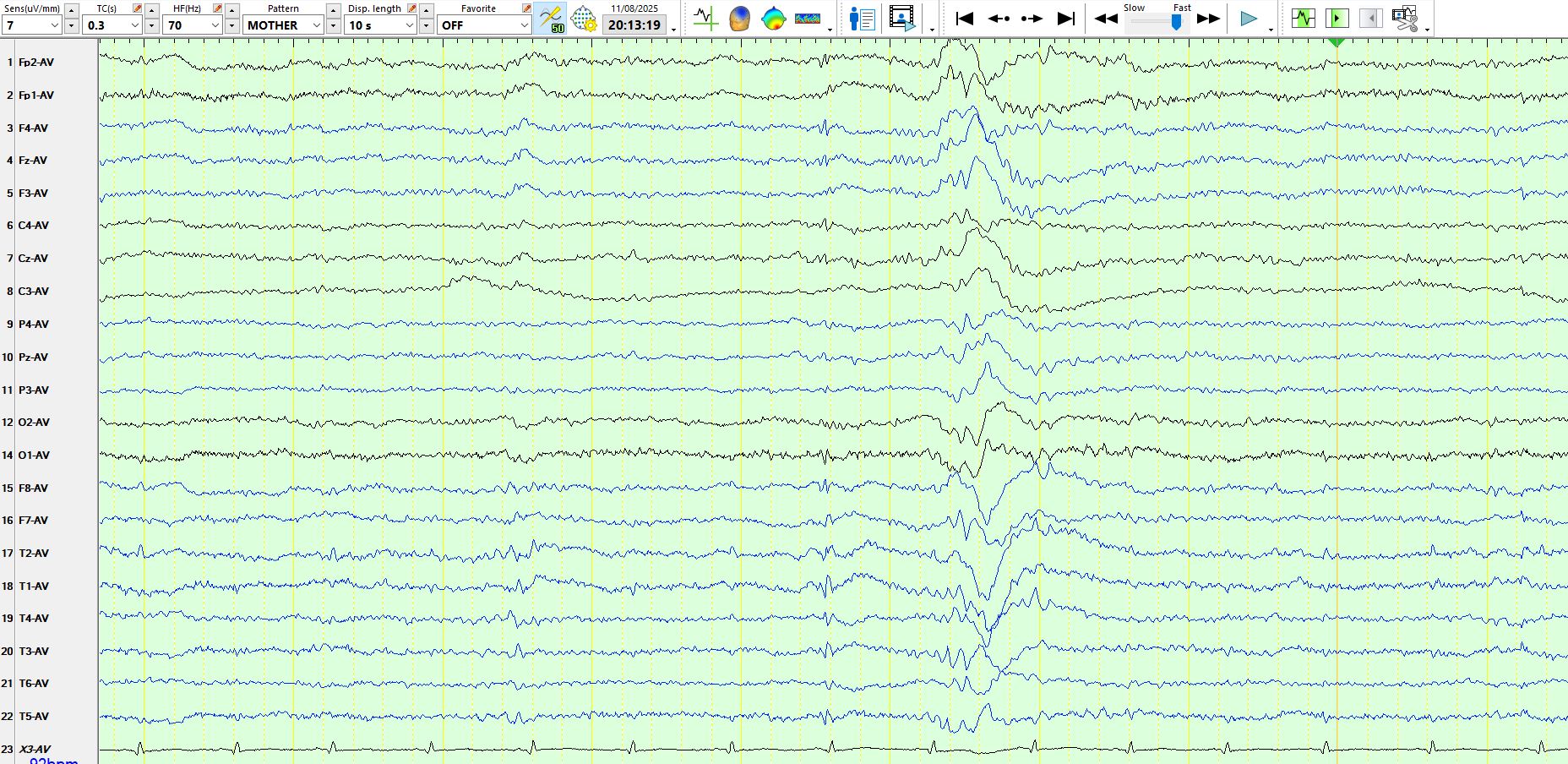
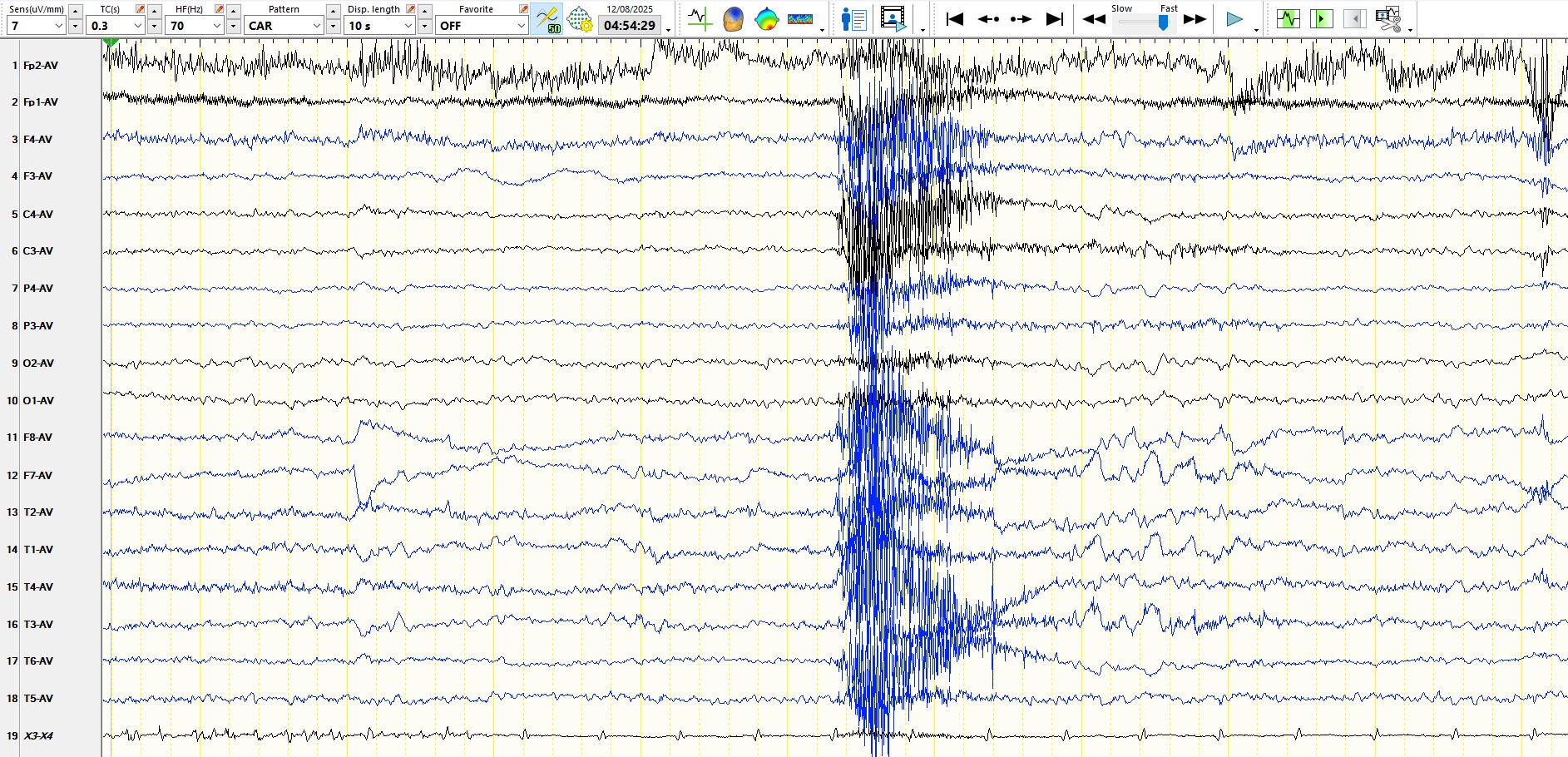
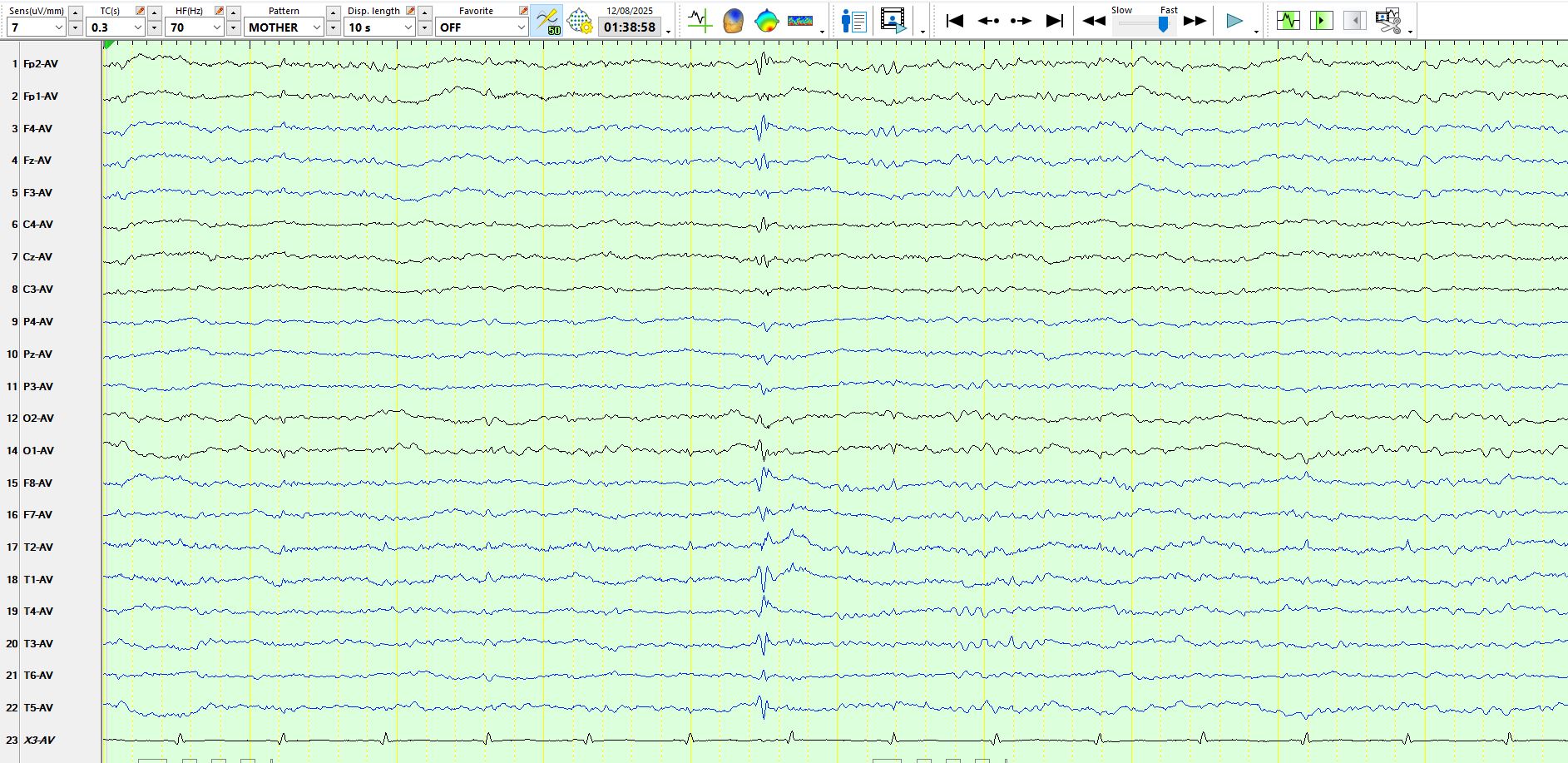
The above wave is a good deal higher in amplitude than those on the preceding pages and there is a slow wave at M1-F7, yet the sharp component retains the morphology and distribution of a small sharp spike. The point of showing this is to demonstrate how easily you might start interpreting a small sharp spike as a spike-and-wave, especially if you have a bias, based upon the history that you have obtained and your clinical diagnosis. You may easily have confirmation bias.
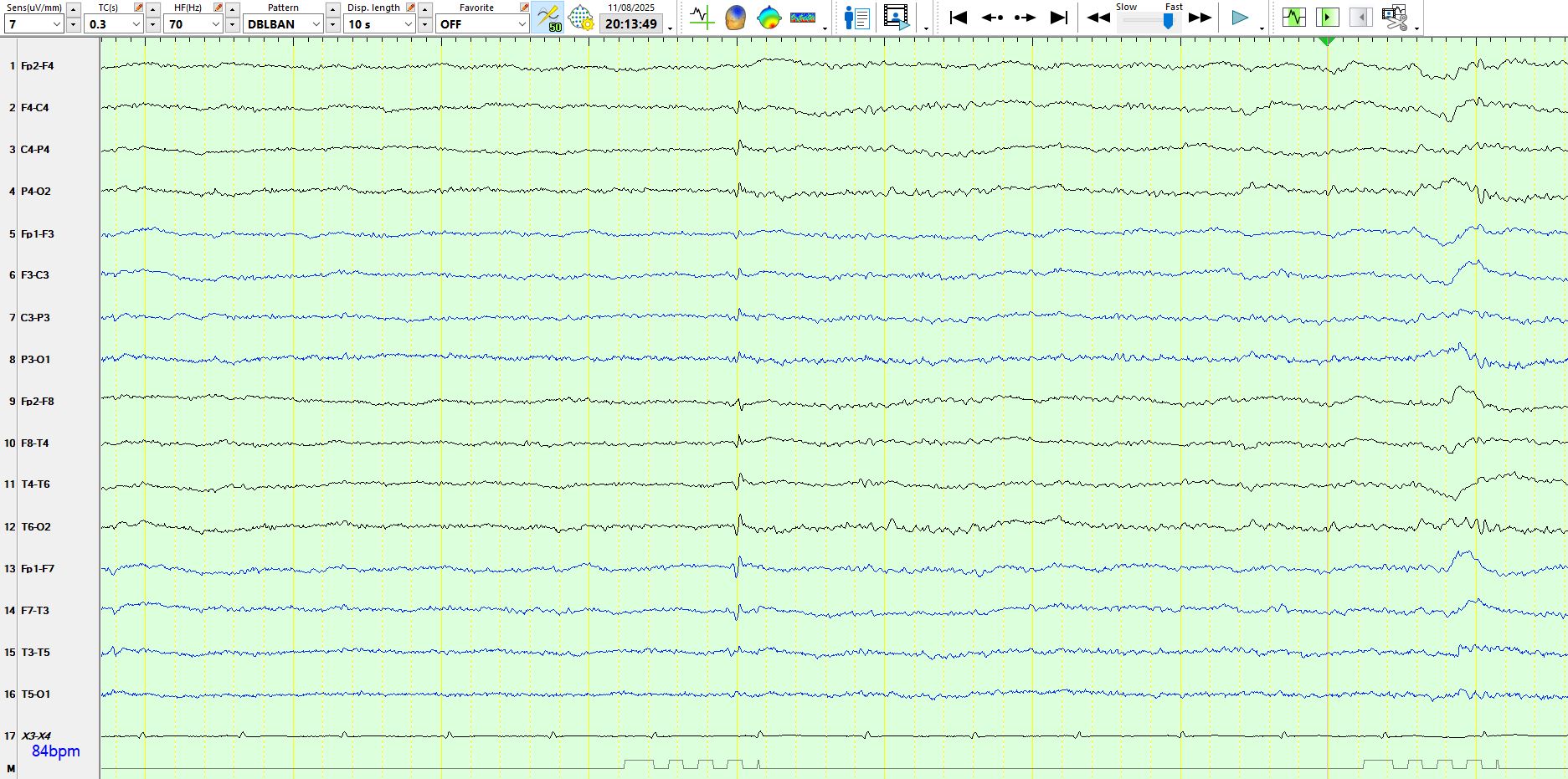
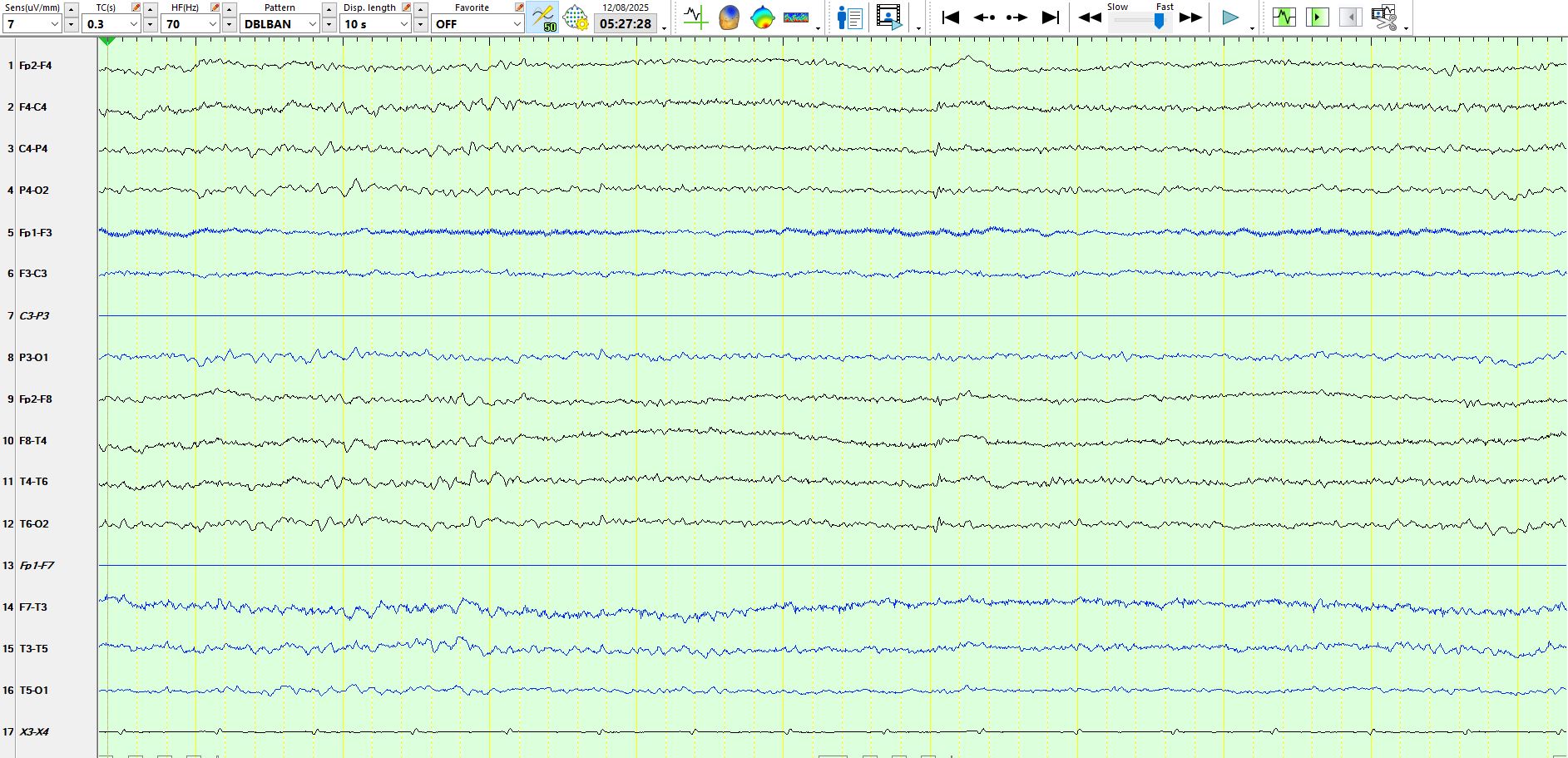
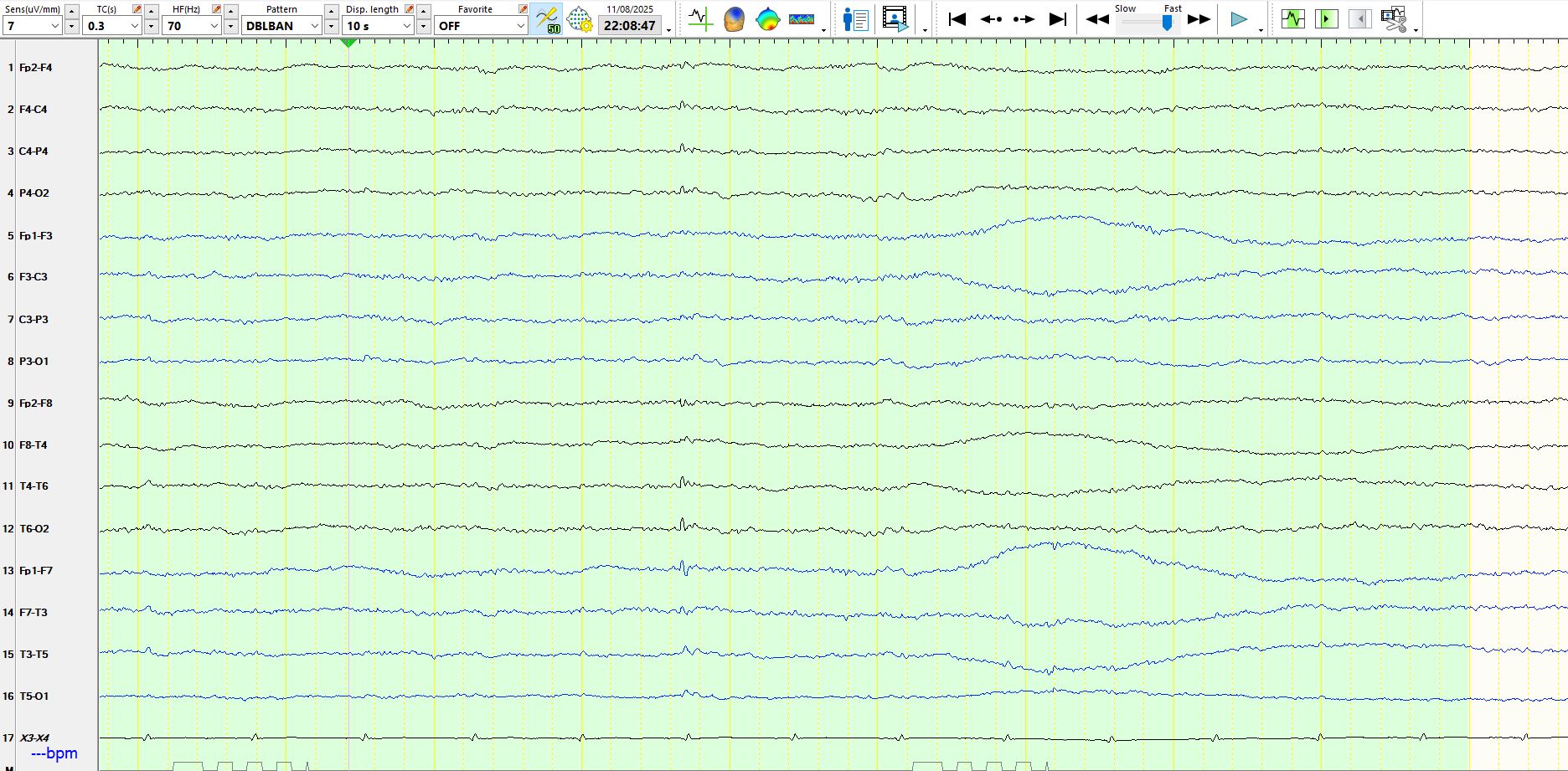
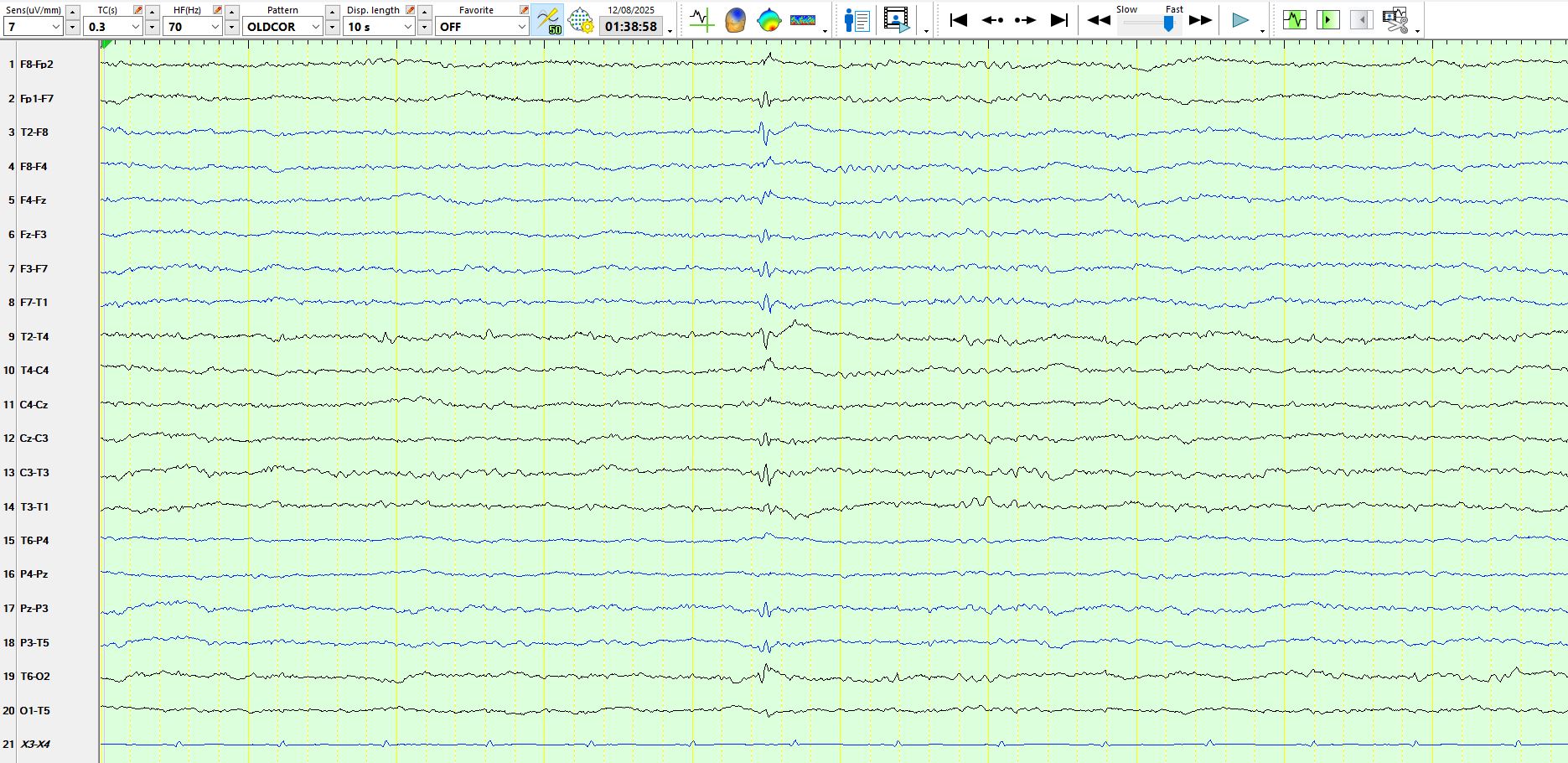
The above page represents the previous page on a bipolar montage and in this instance the small sharp spike is easily seen on the bipolar AP montage. The point is that amplitudes of small sharp spikes vary.
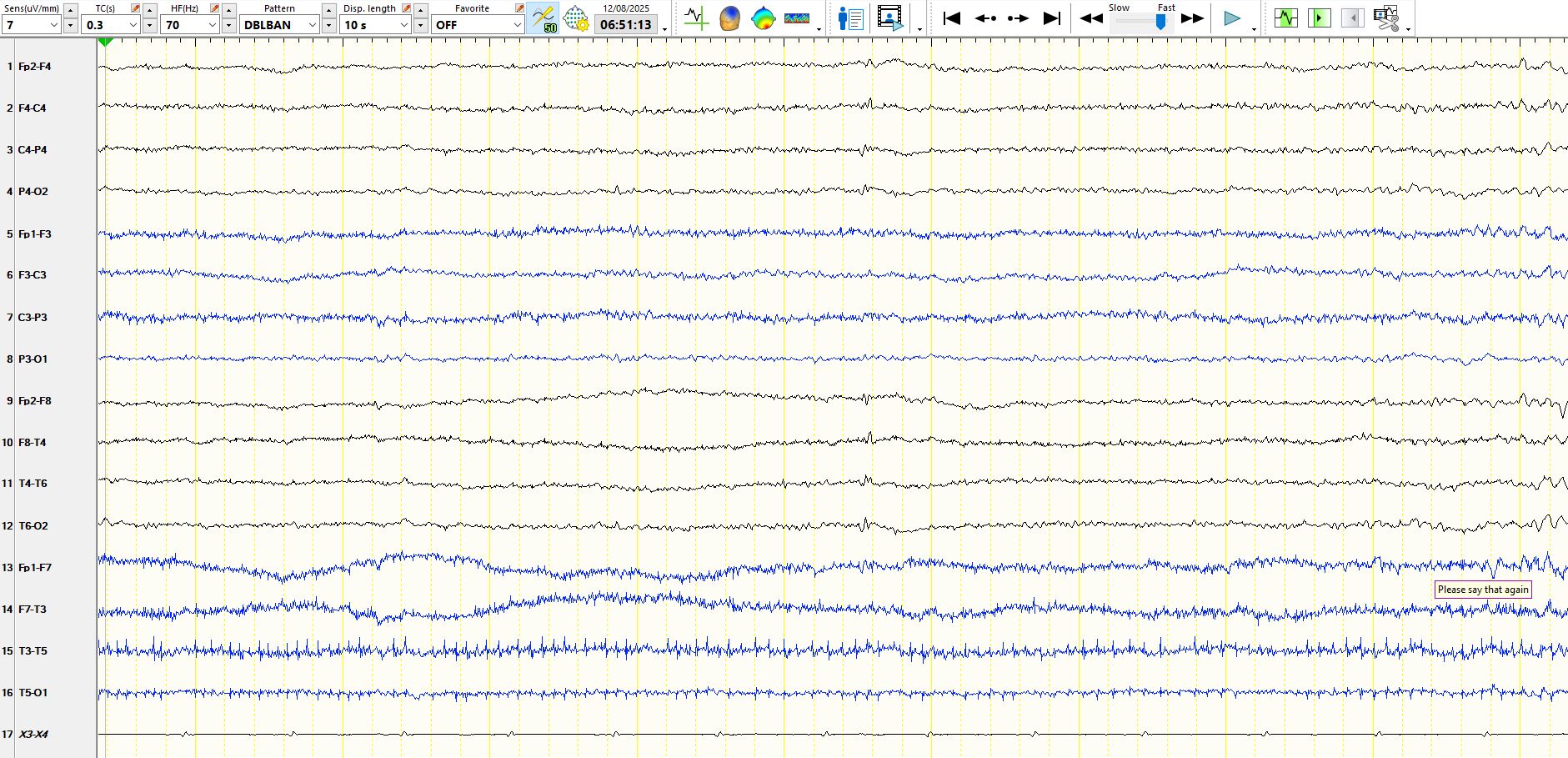
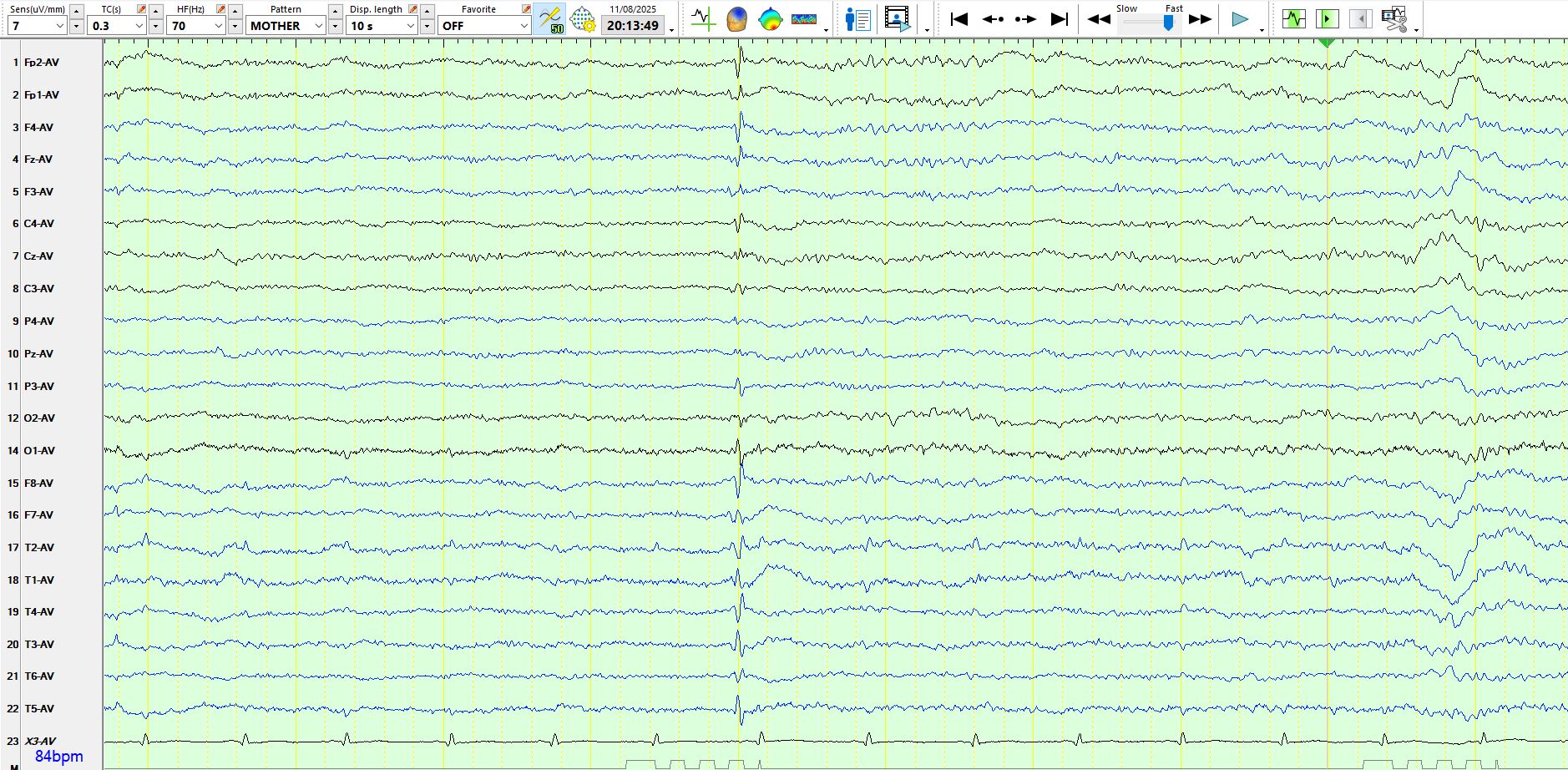
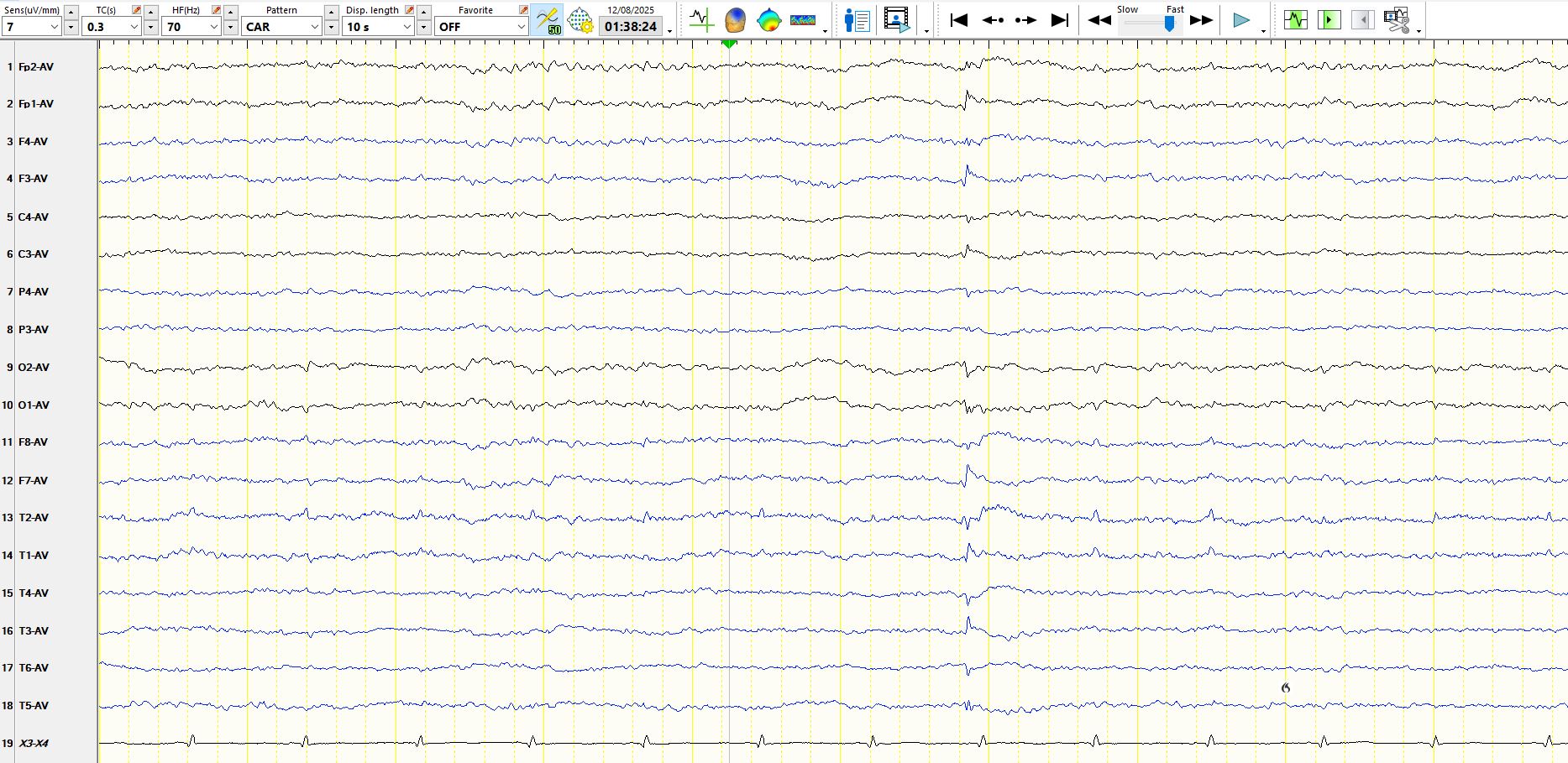
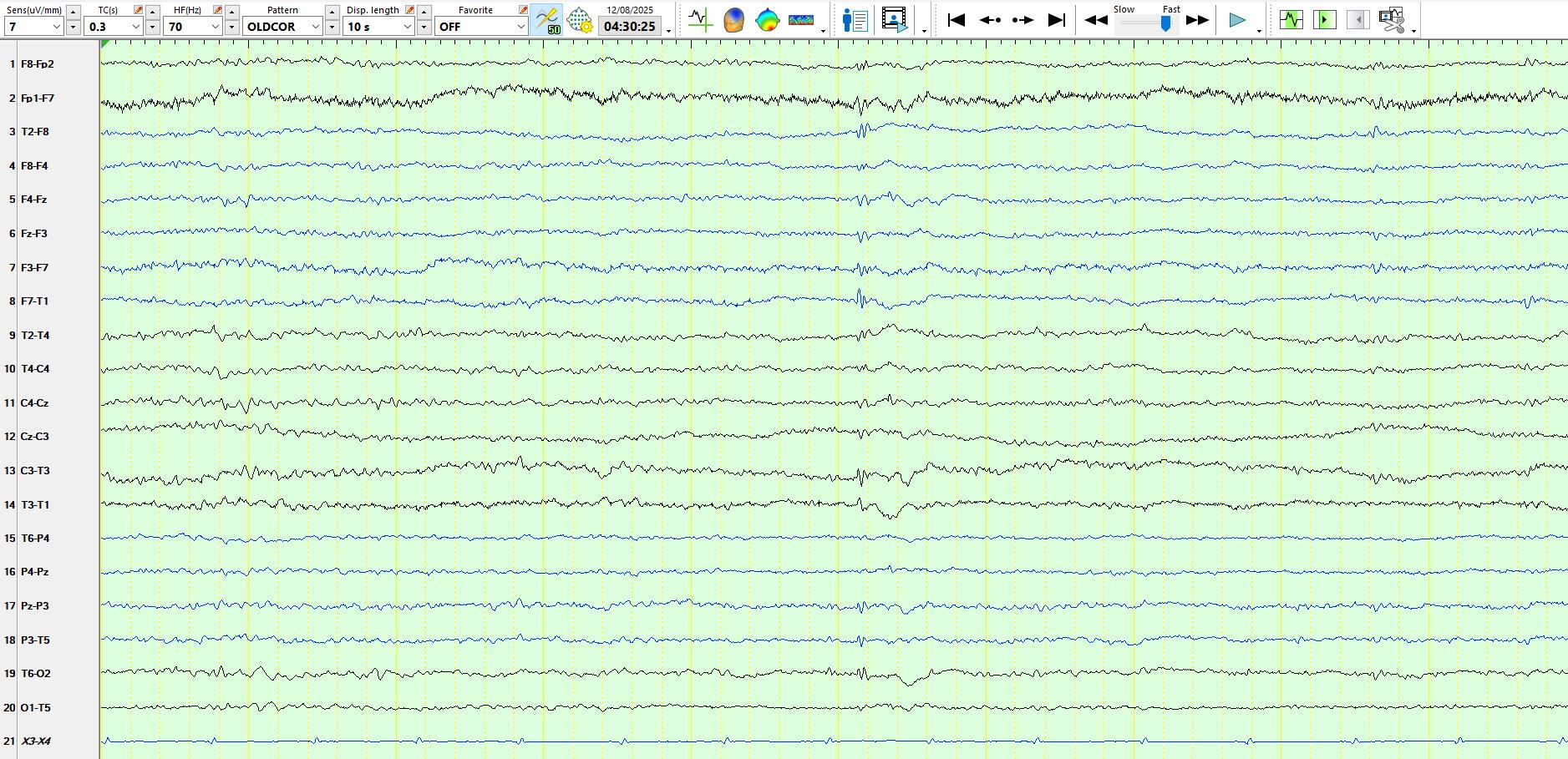
The patient had lots of typical small sharp spikes; The page above and below display the same wave on the common average montage (above) and the bipolar montage (below). On the bipolar montage it is far less conspicuous than on the referential montage.
Above there is yet another small sharp spike with a biphasic morphology, but the succeeding slow-wave caught my eye. Sometimes there is a slow wave associated with small sharp spikes.
The wave above and below have similar features, but are triphasic. However, they are otherwise characteristic of small sharp spikes.
Above and below are waves with multiple phases that raise some concerns; however, in this instance they are low in amplitude and there is not a well-developed slow-wave after these. I was certainly concerned about them, but noted them in my report, but did not interpret them as inter-ictal epileptiform discharges. They have several of the features of small sharp spikes and, as always, it is far better to err on the side of under interpretation of waves that might concern you.
In the page above there is another notable slow-wave.