
Red Alert 2
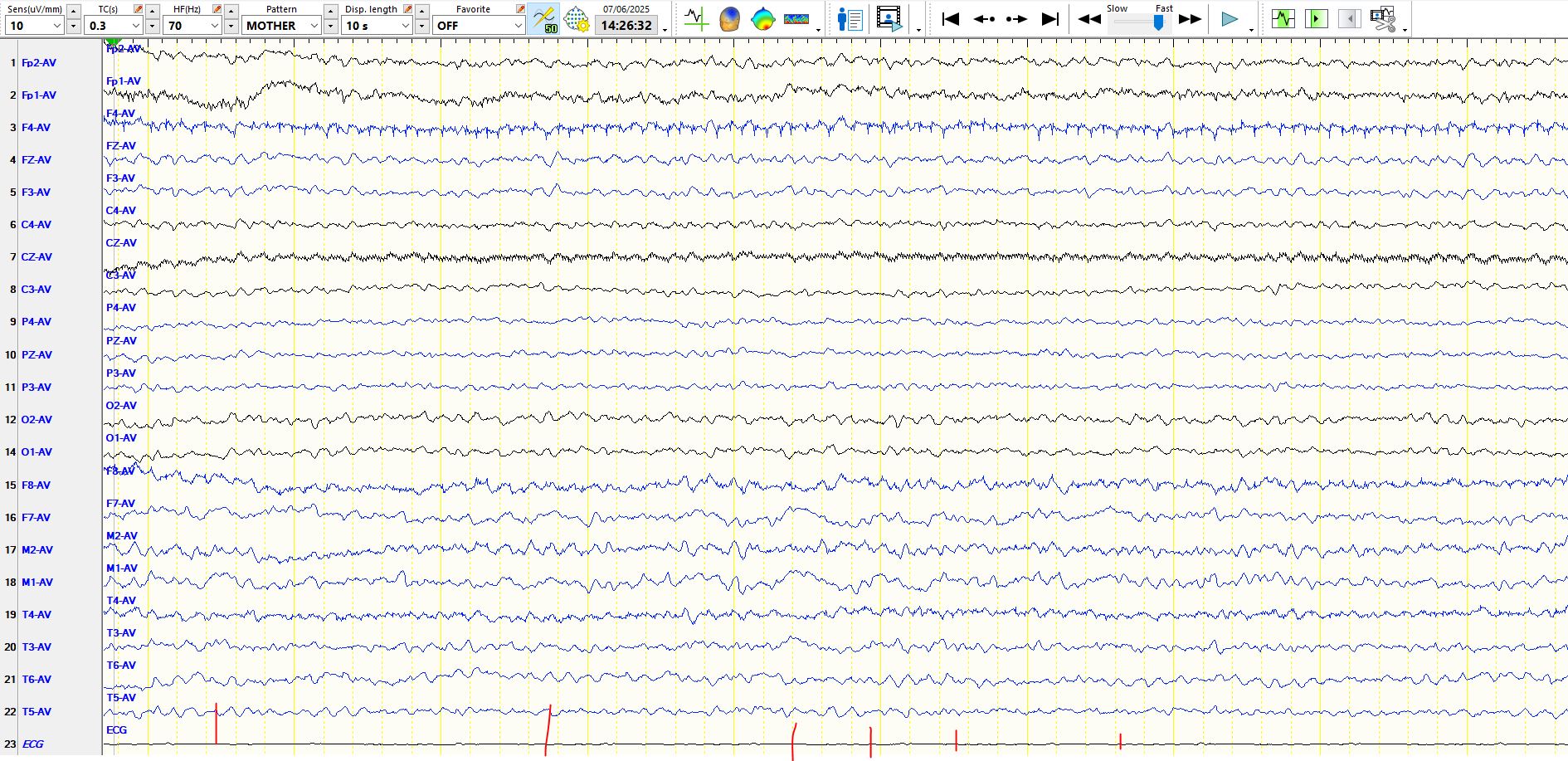
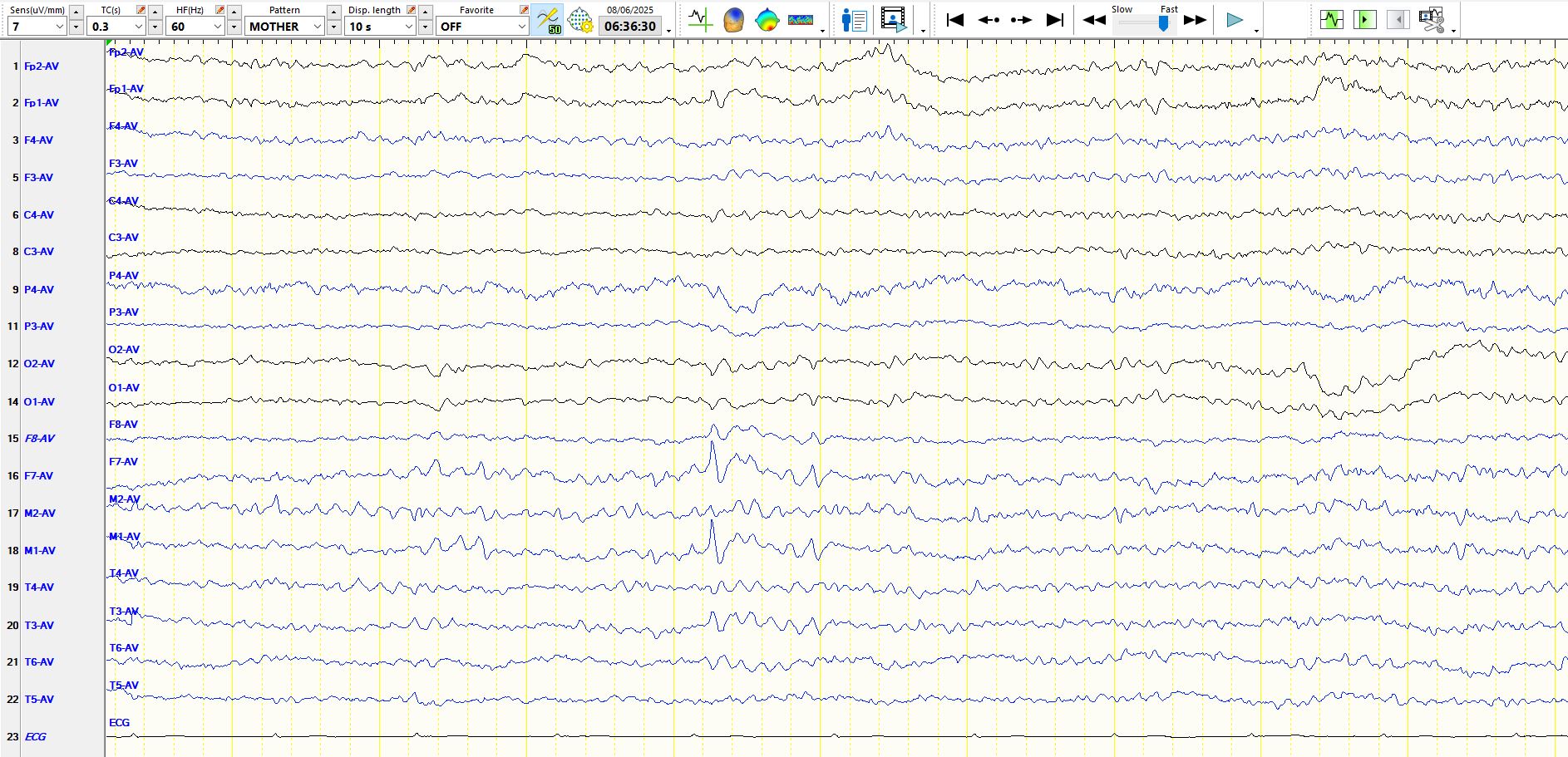
Jun 09, 2025Here is another example of a "wicked spike":
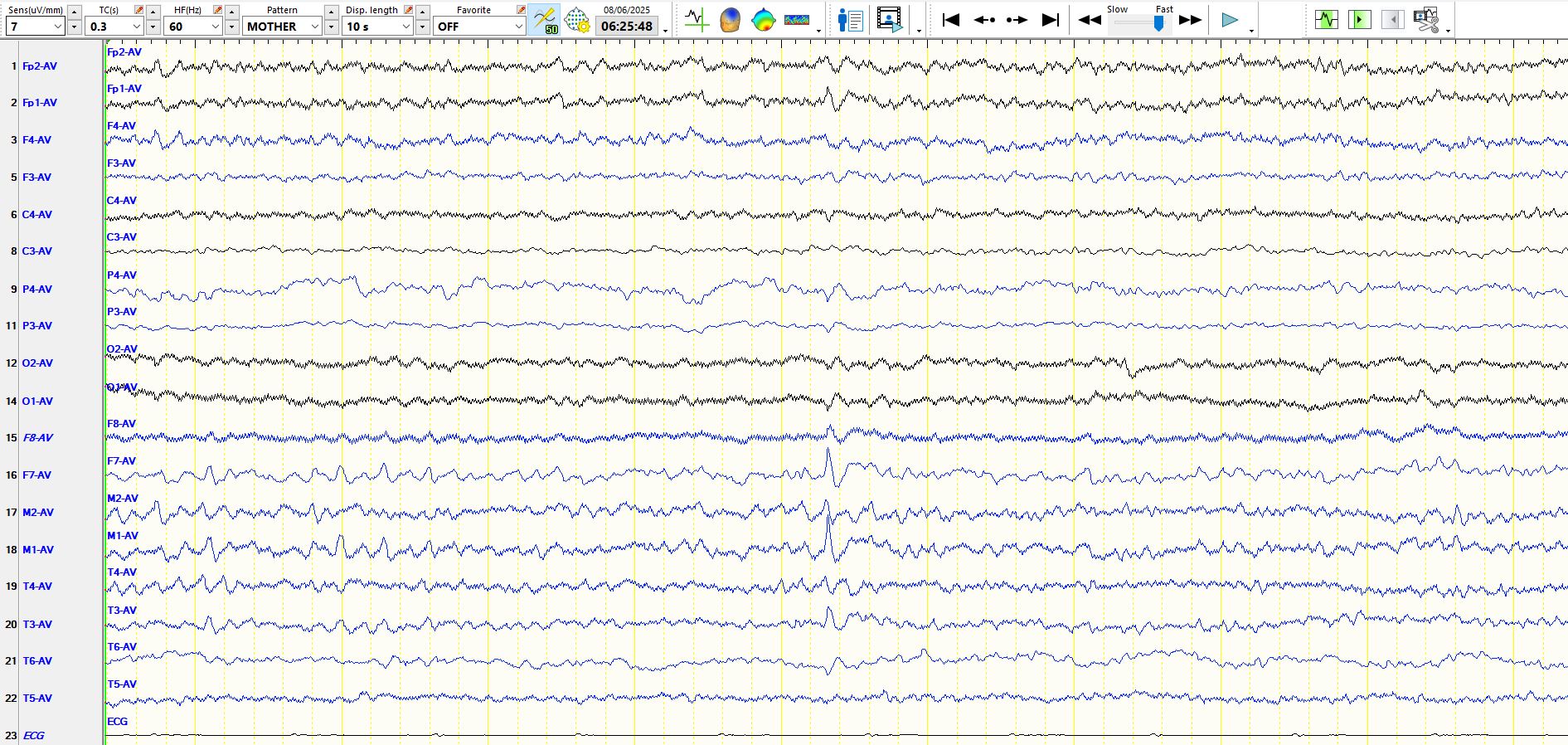
Try and store this image and those below in your memory and try to ensure that:
1. You will have a high index of suspicion for these waves when you see sharply-contoured waves over the temporal regions
2. You set the bar high when calling something a spike or sharp wave (inter-ictal epileptiform discharges) and, in the event of even minor uncertainty, you default to doing no more than reporting the wave in the body of your EEG report with words like "nature unclear" or, if you are certain about the nature of the waves, calling them by their name ( "wicket spikes" or "wicket waves" or "small sharp spikes" or "14- and 6-Hz positive bursts" et cetera). I often read the EEG and say to myself "Am I sure that this wave means that this patient really has epilepsy?". Remember, we as human beings have an appalling tendency to overconfidence. There is reproducible scientific literature which demonstrates that people think that they are better than 80-90% drivers, irrespective of age-group (this is statistically impossible). Furthermore, intuitive interpretation of EEG is prone to errors that relate to the way the brain is made. The book by Daniel Kahneman, Nobel prize winner, about the "thinking fast and thinking slow" systems in the brain is highly applicable to EEG interpretation.
Judgment under Uncertainty: Heuristics and Biases - PubMed
Are we all less risky and more skillful than our fellow drivers? - ScienceDirect
The trouble with overconfidence - PubMed
3. You try to read the EEG without bias. I do this by avoiding looking at referral letters and then reporting the EEG, before integrating the history into the "clinical interpretation" (see below about the quality of the history). Of course, you will sometimes know the patient and be confident about the diagnosis of epileptic seizures one way or another; if this is the case, read the EEG as though your diagnosis may be incorrect, especially if it is epilepsy, report your findings in the body of the EEG and then do the clinical interpretation. An EEG loses its predictive value when read in a biased manner and you may as well not do the EEG. You should view the history and the EEG as independent data points in the process of trying to predict the absence or presence of epilepsy. They lose their independence when the information about the other data point is known at the time of interpreting one of these.
Note: In trying to determine whether the patient has or does not have epilepsy, the predictive properties of the history and the EEG are determined by the quality of the interpretation of each of these. When each is done well and if done independently, these probabilities multiply. If not one quickly goes down the slippery slope of diminishing accuracy of the diagnosis. Remember that in predicting a diagnosis of any sort, it is a case of "rubbish in and rubbish out".
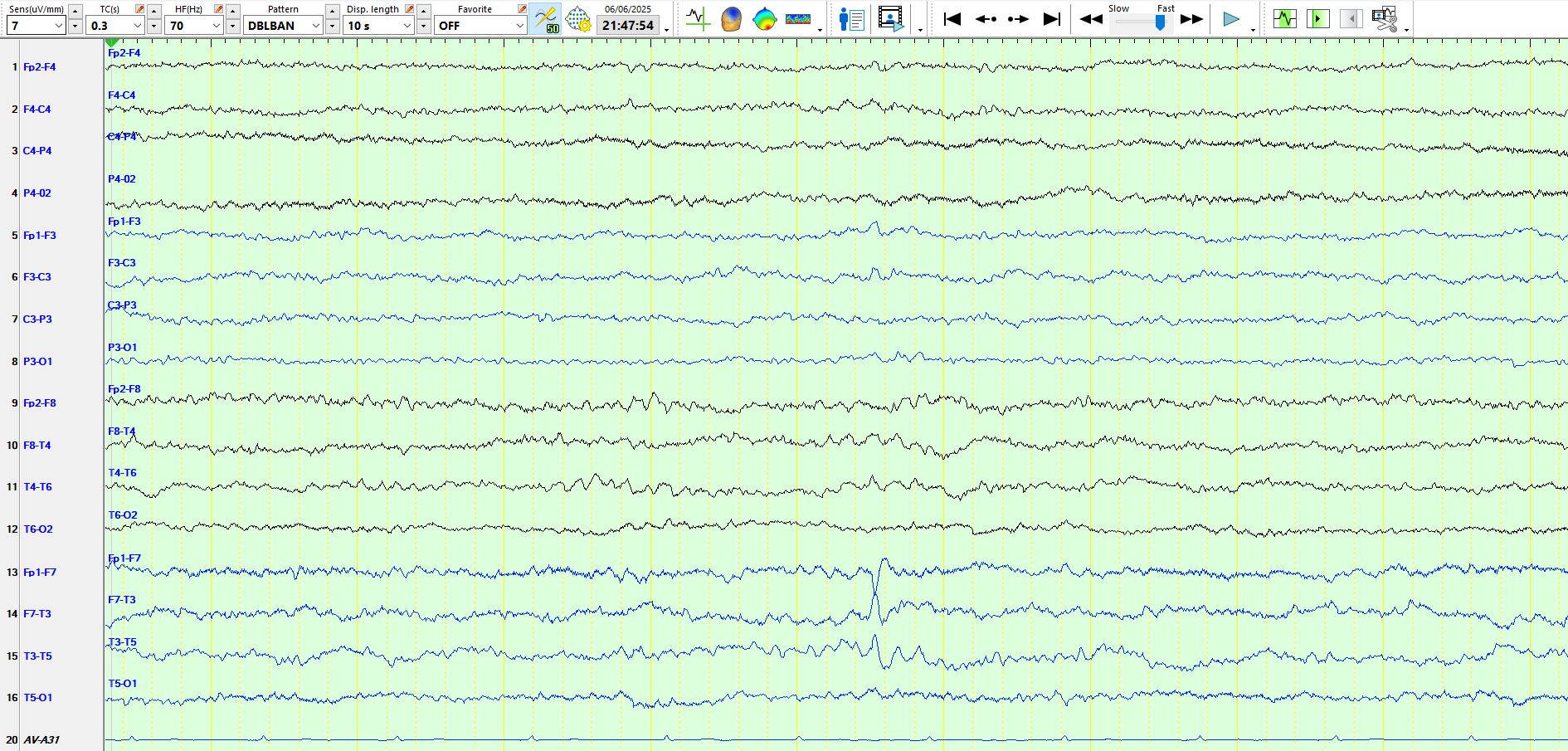
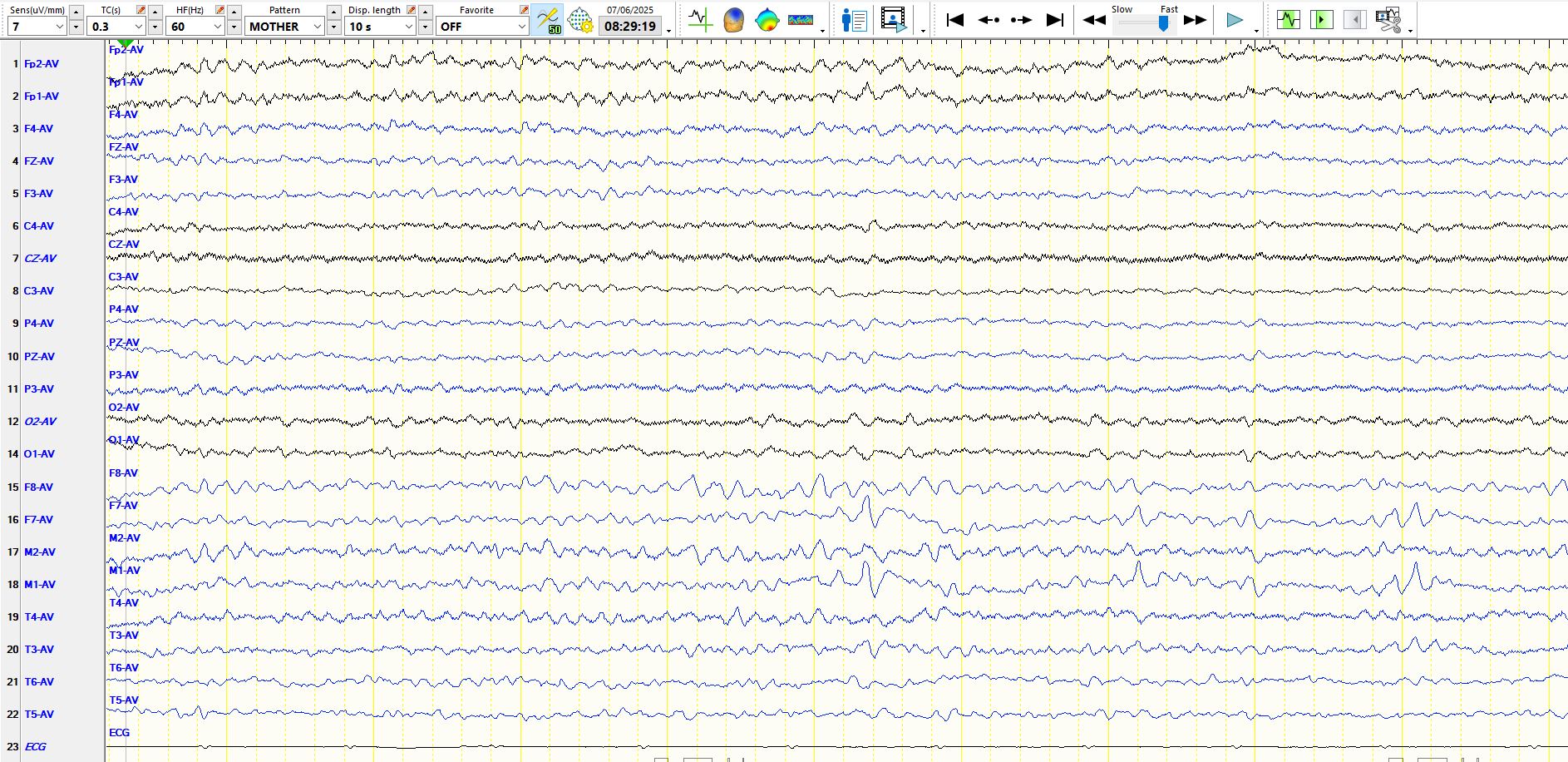
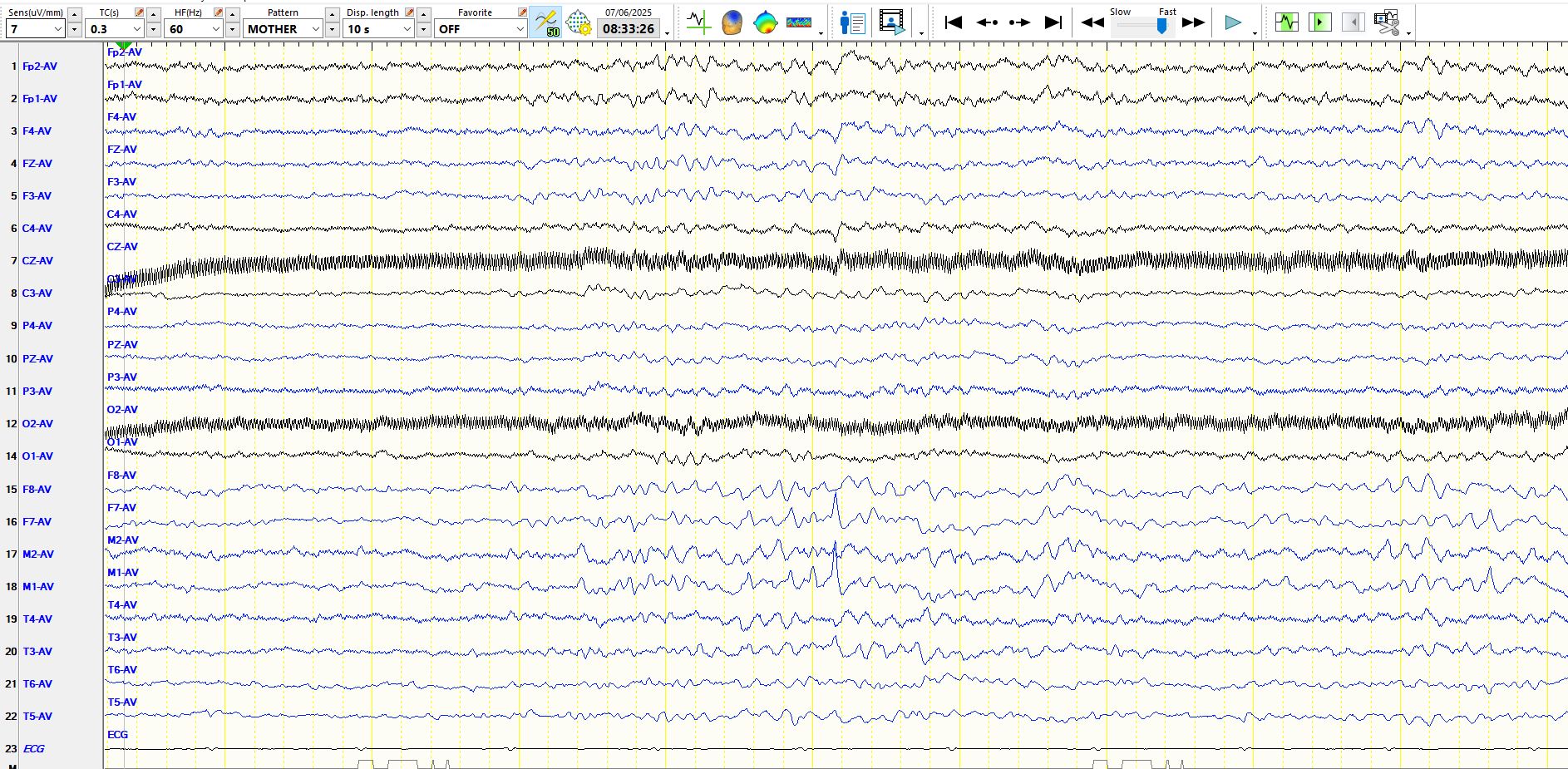
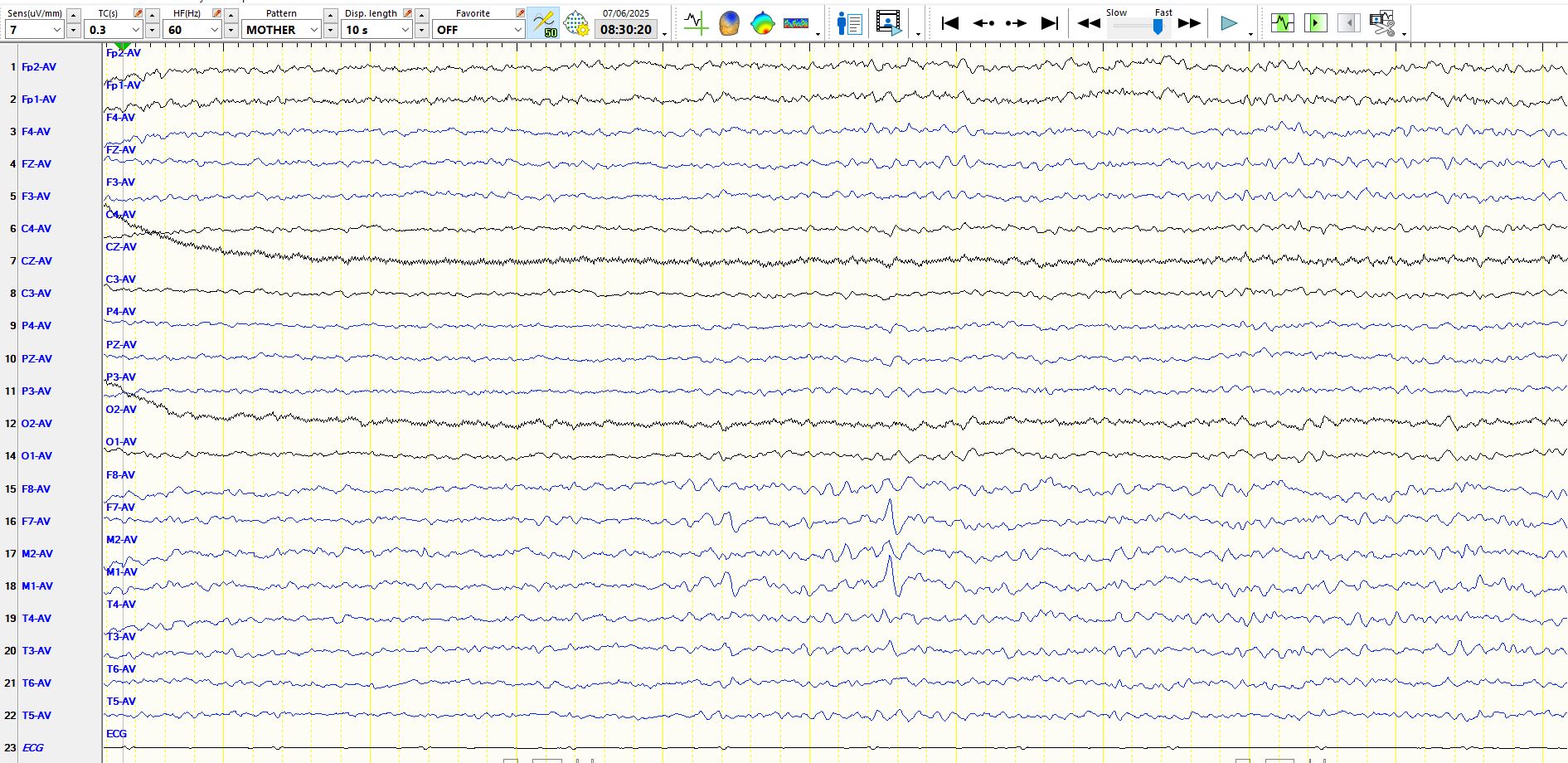
Below is another "wicked wave"; the same epoch is represented on 3 montages below.
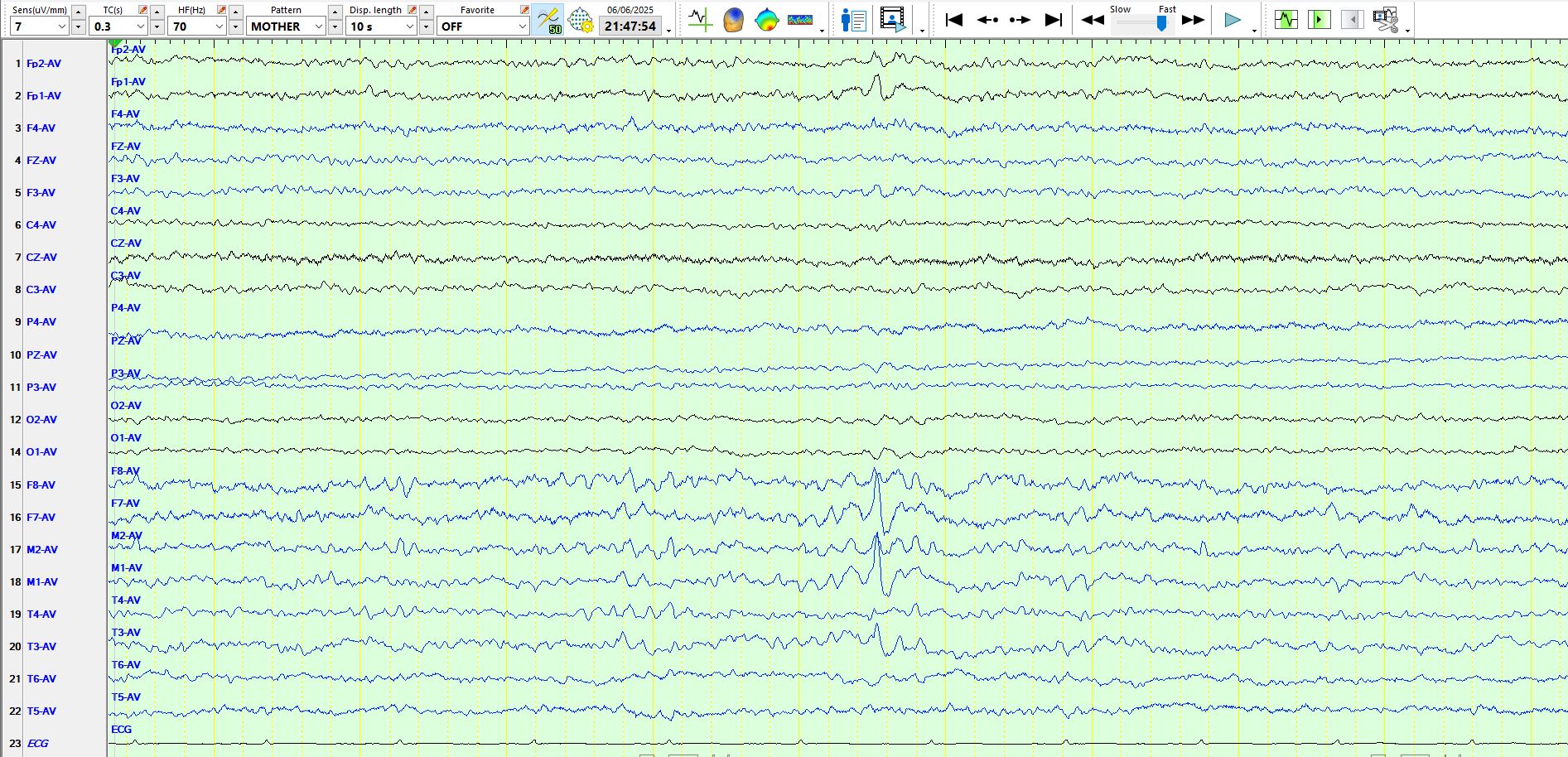
Bipolar AP:
Coronal:
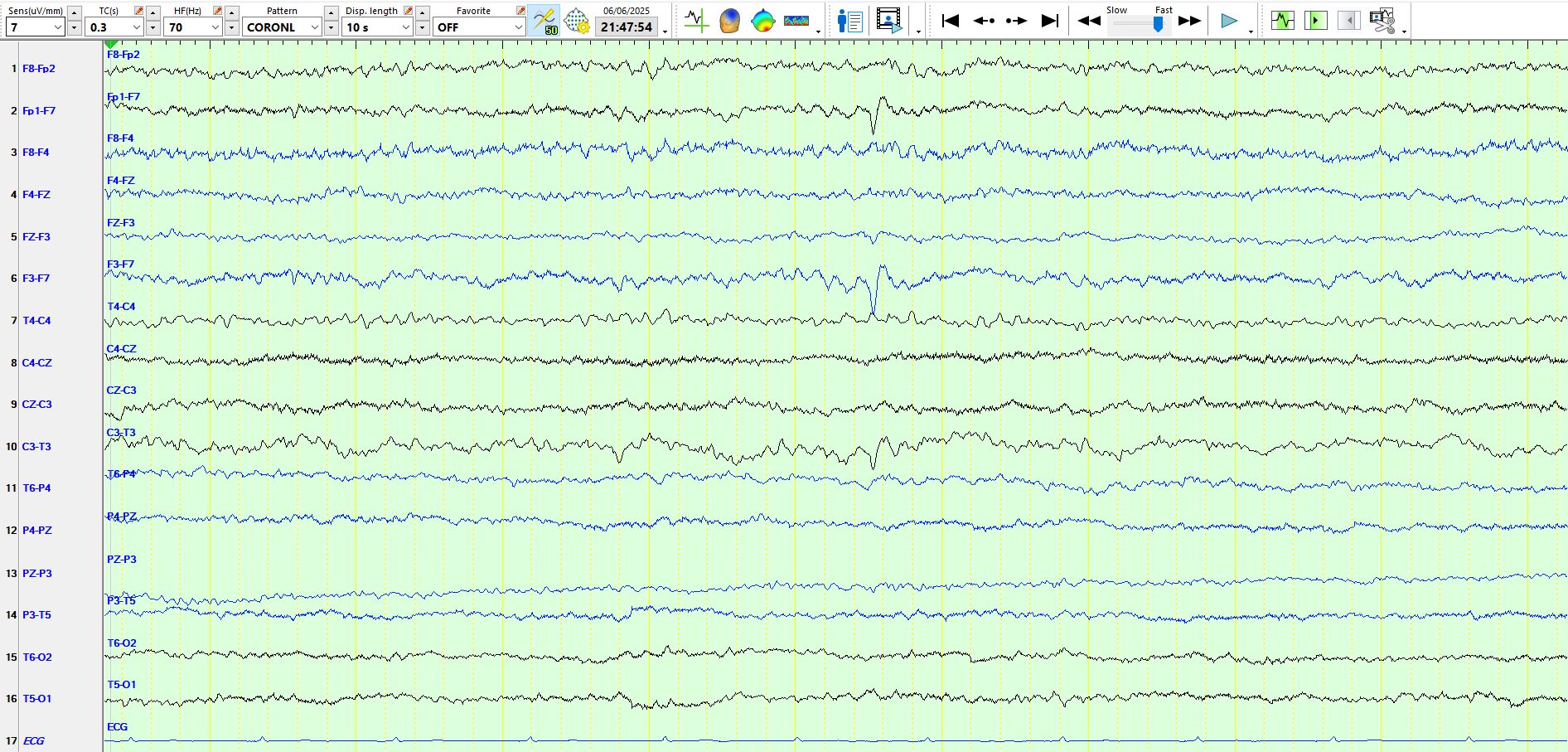
Be assured, the above patient has delta waves (six on this page) at M1-F7-T3:
Below are examples from Reiher's classic article of wicket spikes. Notice the slow wave in the first example

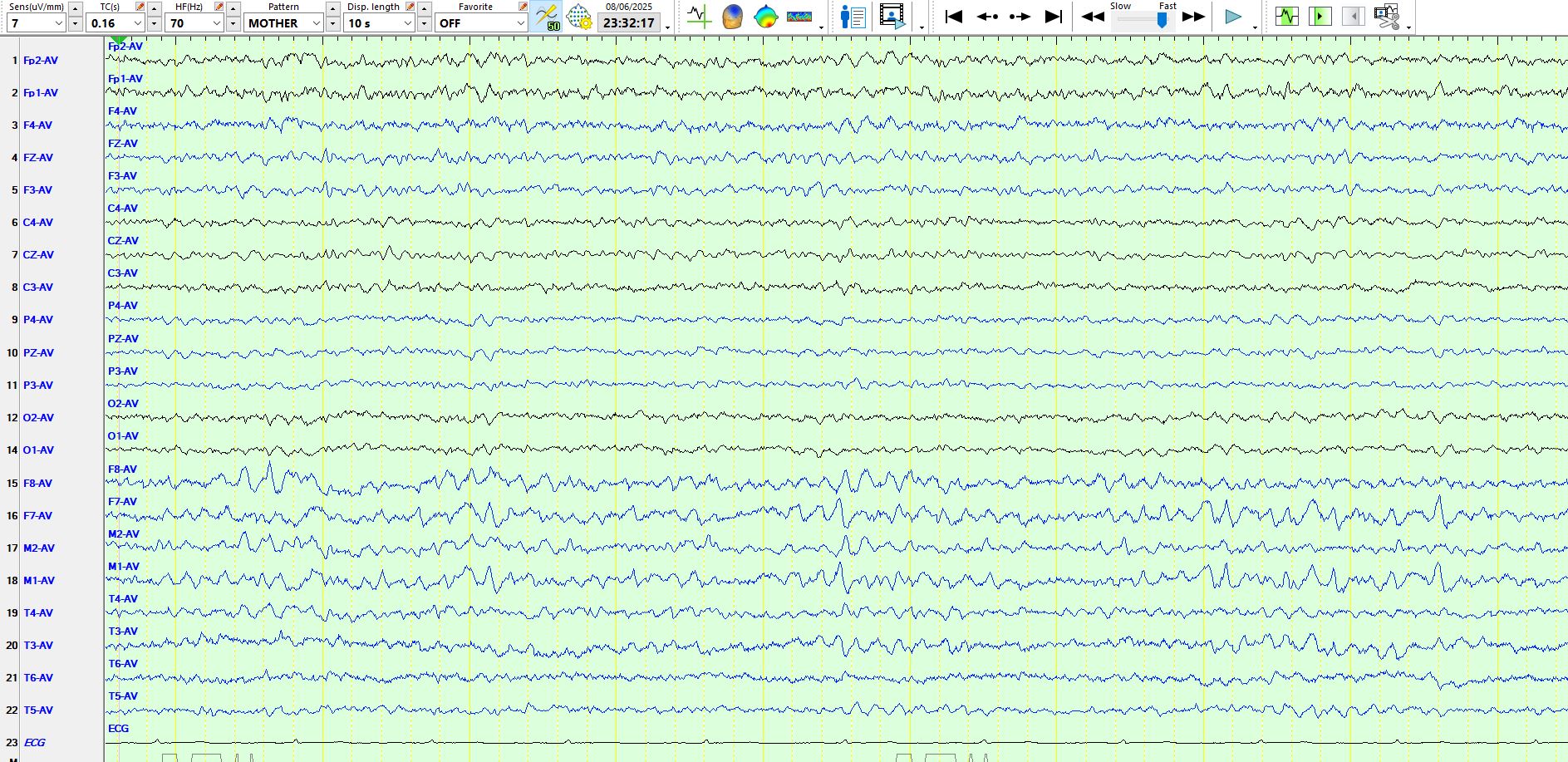
The following example demonstrates a waveform that is abruptly much higher in amplitude than previous waves and there are some slow waves in same region:

Wicket spikes as part of a train and a separate example of an isolated wicket spike ("know thy enemy"):

An isolated wicket spike ("know thy enemy")

some more examples
Below is an example of (red arrows) and delta waves (red lines)

And here (below), another example of "pseudo spike-and-wave" (this is not an electrographic term, but you may find it useful to remember the phenomenon). To reiterate, in this patient these waveforms appeared on the left, but such persistent asymmetries of temporal alpha, wicket waves and wicked spikes are common (the human face is asymmetric). Revisiting the laterality of wicket spikes with continuous EEG - PubMed
"Know thy enemy"!
Then go back and look at these examples: 61, amnestic events
And read these:
Errors in EEG interpretation and misdiagnosis of epilepsy. Which EEG patterns are overread? - PubMed
Revisiting the laterality of wicket spikes with continuous EEG - PubMed
Clinical and EEG features of patients with EEG wicket rhythms misdiagnosed with epilepsy - PubMed