
What is wrong with the "double banana" montage?
Jul 07, 2025Have a look at the following page of the EEG and count the number of spikes.
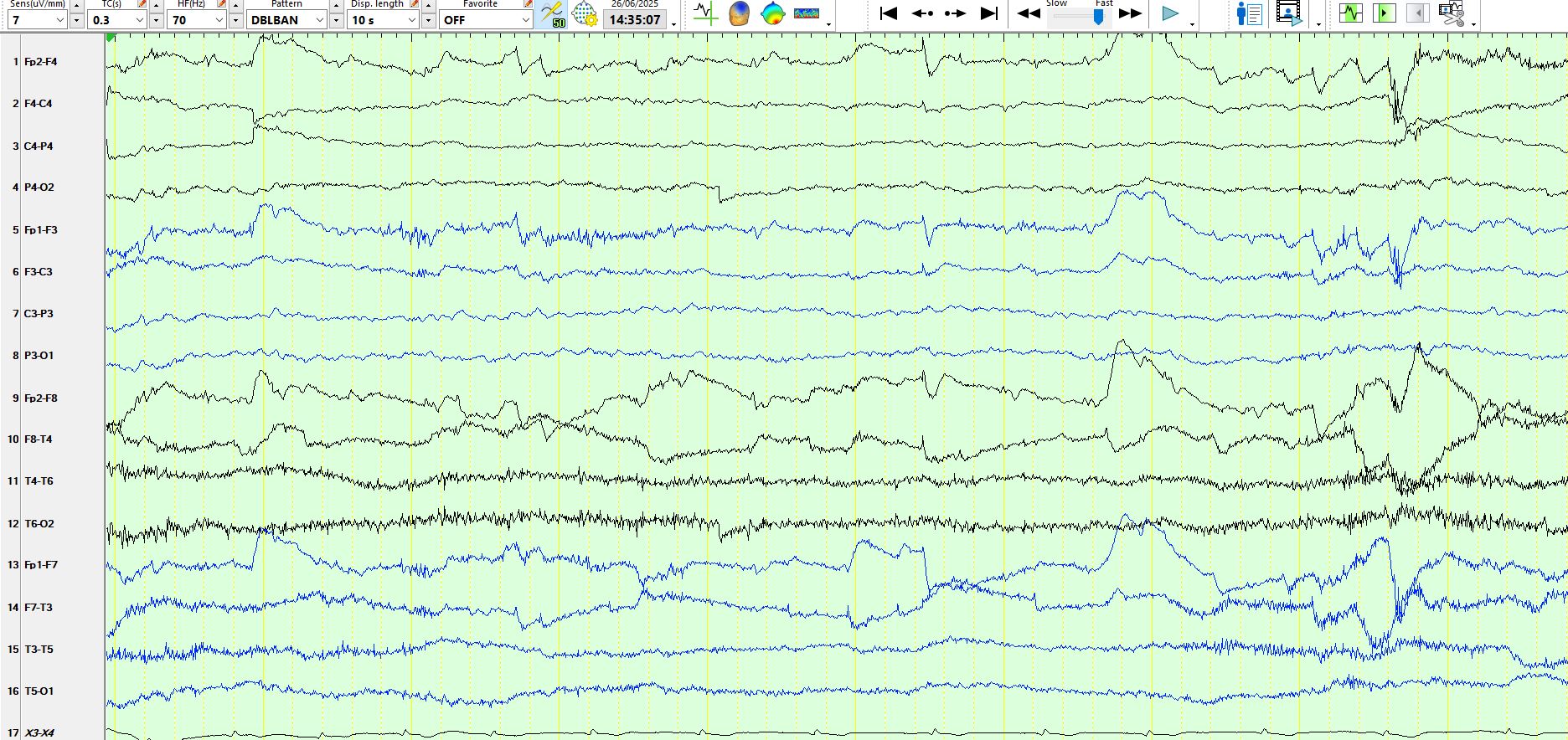
In the days predating digital EEG, the bulk of the routine EEG recording was performed in the above manner. Depending on the EEG laboratory's protocols, there likely would have been a coronal and a referential montage, but these would have been performed for no more than a few minutes of the 20-minute recording. The routine EEG has a poor sensitivity for detecting inter-ictal epileptiform discharges and, if there were spikes that were missed by the above montage specifically, the likelihood of detecting these on another montage would be determined by the probability that such a spike from someone with epilepsy would appear during those few minutes that the coronal and referential montages were performed.
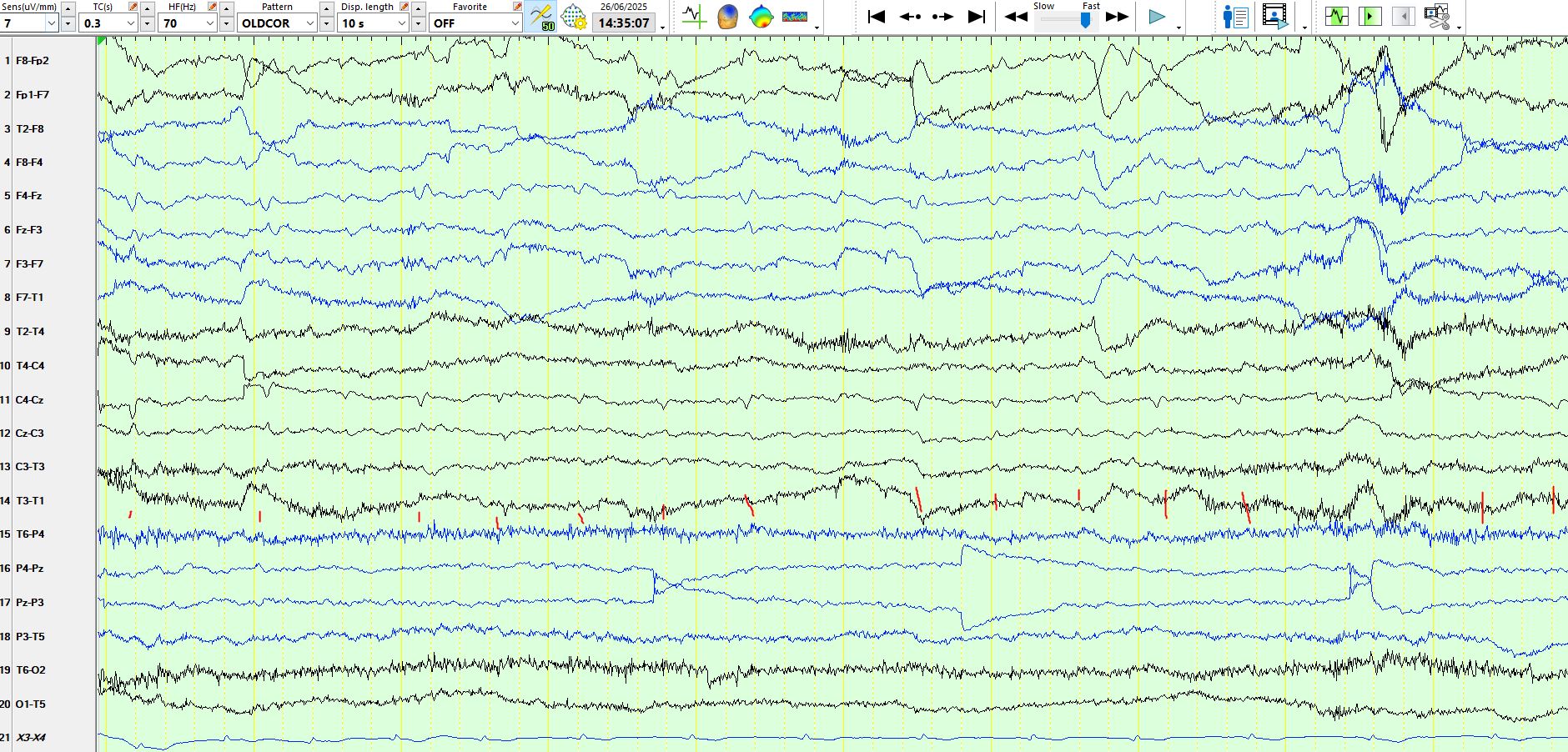
Here is the above page represented on the coronal and referential montages. You likely will be astonished by the number of spikes that have been missed by the double banana montage. Lesson learnt?
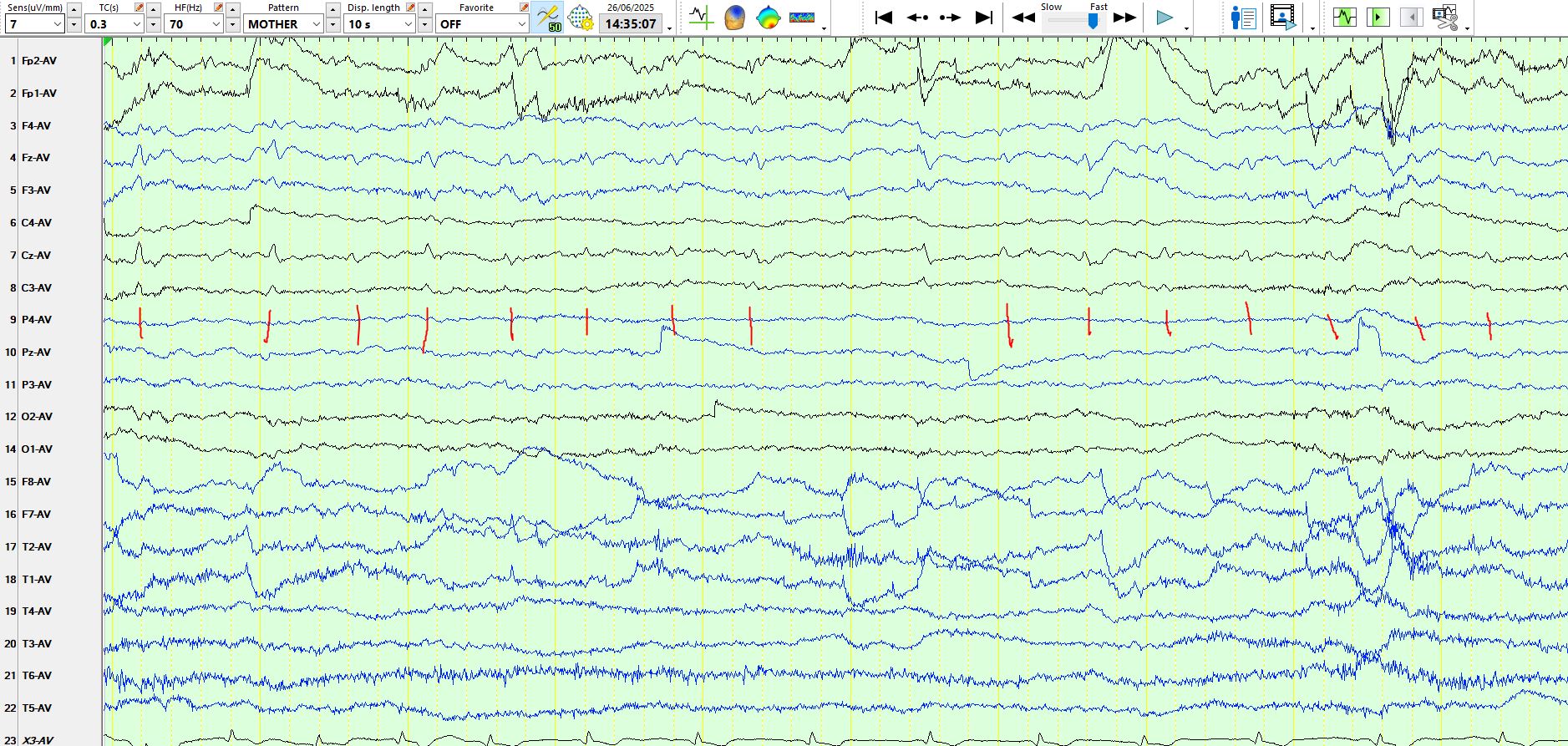
I wrestled with just such a case when starting our epilepsy monitoring unit in 1999 and remembered the words of one of my mentors, Warren Blume, who had taught, "construct your own montages". Now you might say that with digital EEG the problem is solved, because you can look at the recording on multiple different montages. Well, you certainly can, but then you would end up reading the same EEG 3 times on different montages, which, in my view, was an inefficient use of time. This led me to construct what I called the "Mother Montage", named in this way as I wanted a montage that was "the mother of all montages" (pardon the expression). The idea was to have all of the scalp electrodes represented on a single referential montage, so as not to run afoul of the above problem. That is the easy bit. The next difficulty relates to the reference used in this montage. There is no right or wrong answer to this; I opted to use the common average, deciding that I would choose which electrodes were allocated to the common average. Unfortunately, the common average requires a fair bit of experience and the ability to be mindful of the significant disadvantages of the common average reference used in the "Mother Montage". This relates specifically to discharges that are of high amplitude or discharges which have a relatively large field; these will contaminate the reference and potentially lead to "false localisation" and the representation of physiological waveforms in such a manner that they resemble spikes or sharp waves. The simpler solution is to use one of the more conventional references, such as CZ or A1/A2 or other electrodes. If these become contaminated, it is fairly easy to change the reference electrode retrospectively and remove reference artefact. More of this to follow in subsequent posts.
As is the case in life, one must not seek a perfect solution. It is better to know the limitations of the montage(s) that you are using and also one's own limitations. For what it's worth, the coronal montage is a better solution than using the "double banana" as a default montage, imho. Perhaps most importantly, have a default montage that you use as your benchmark for checking on "what is normal", especially in tricky or doubtful situations. This is the advantage of reading most of the recording using one montage only; it is the quickest way to assimilate normative data. Your brain, must use this data so that you consciously and eventually intuitively recognize when something differs from "norma'.