
Triphasic waves vs spikes
Jul 16, 2025If you want to start an argument, wading into the territory of triphasic waves is sure to have the desired effect! Some authors suggest that spikes and triphasic waves rarely coexist, but I doubt that this would withstand objective analysis. There are plenty of people who write scientific papers who do not spend their days working in the trenches, in this case seeing lots of patients with epilepsy and reading lots of EEGs.
Are Triphasic Waves Different From Generalized Spike-Wave Discharges? - PubMed
"The occurrence of both patterns in the same patient is extremely rare with only a single prior case report."
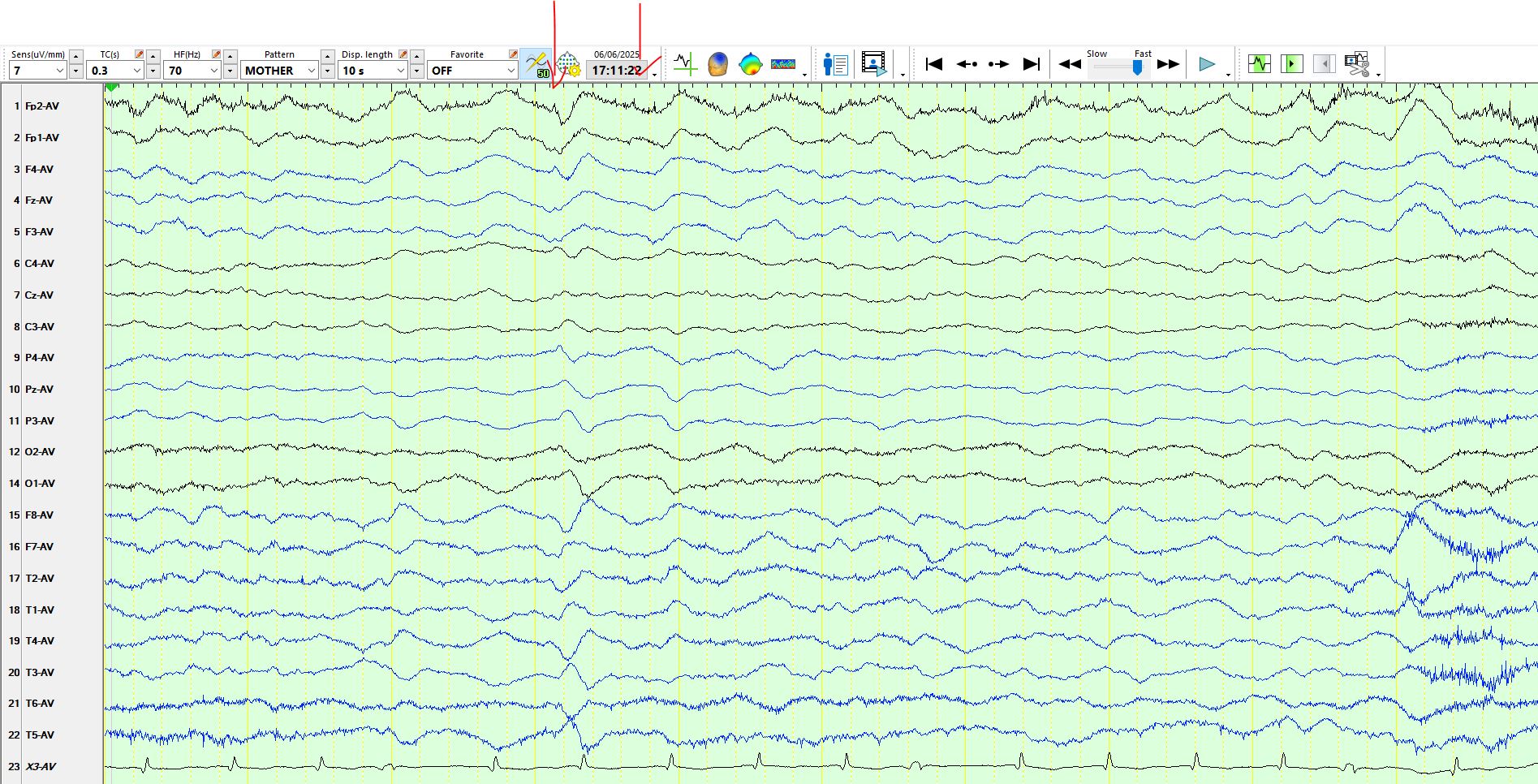
Have a look at the following pages and come to your own conclusions. Several of the waves on the following page might represent either of the above possibilities, but the first wave certainly is a spike, given its very sharp morphology.
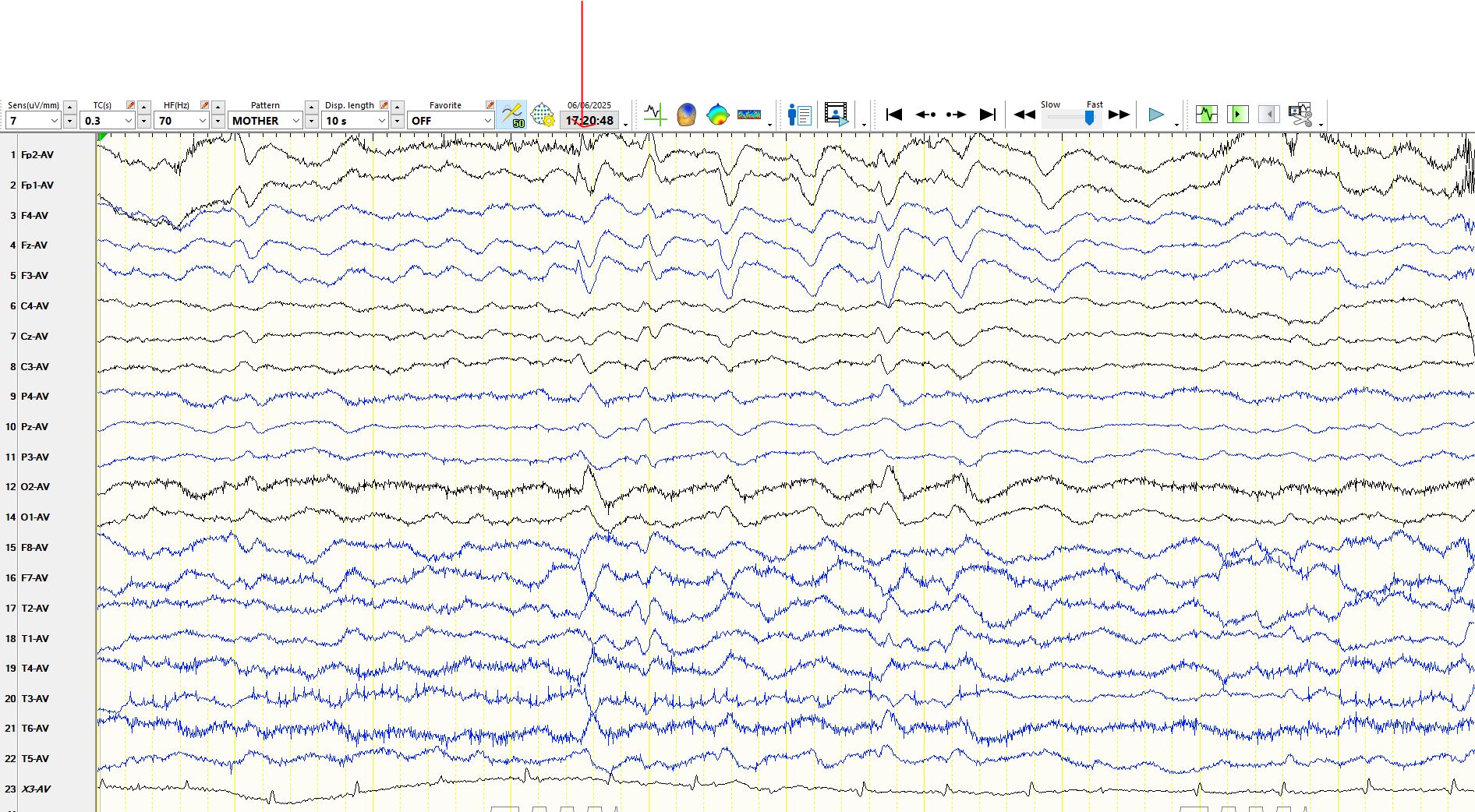
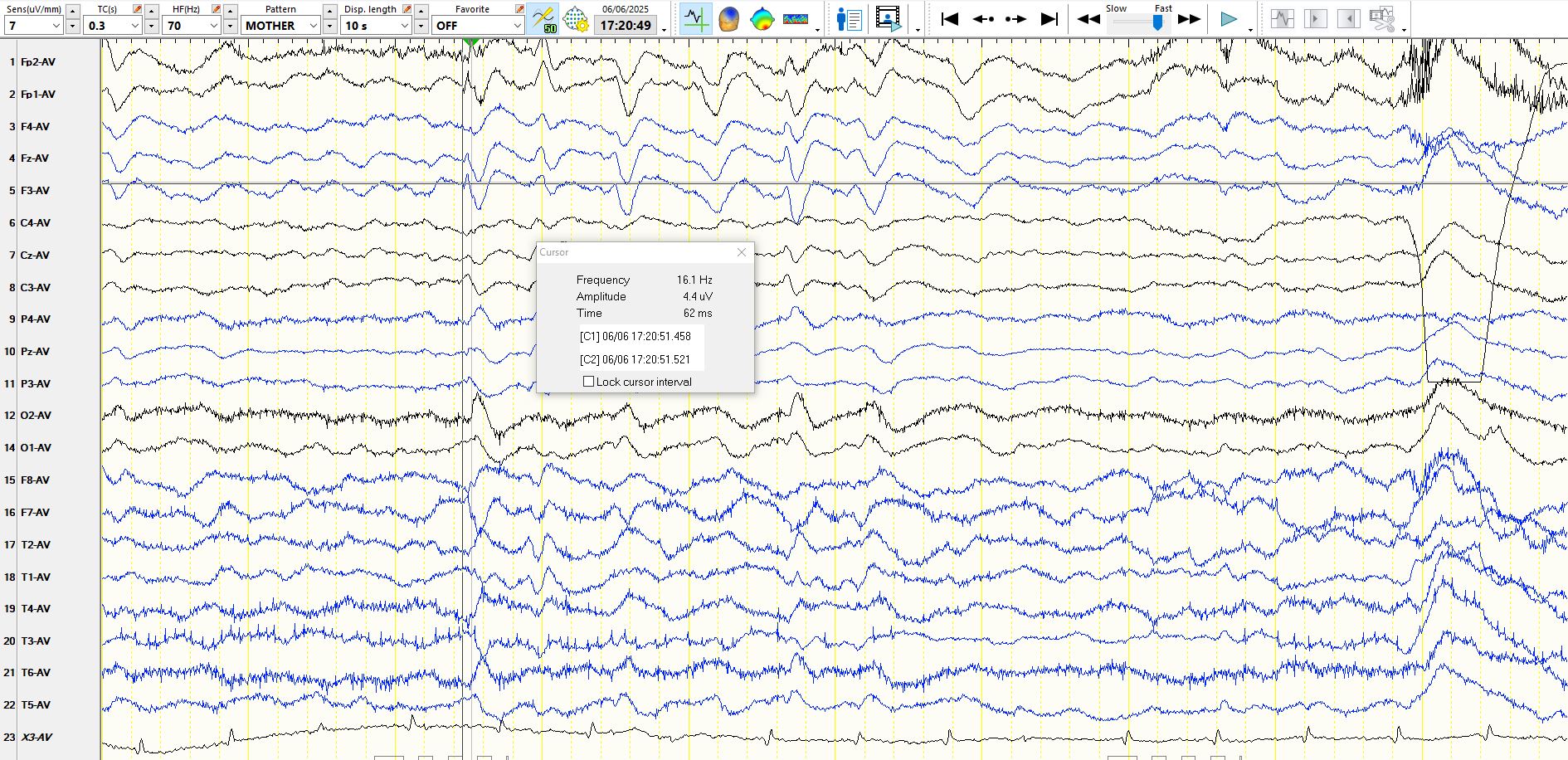
Sometimes it is worth measuring the duration of waves, as illustrated here:
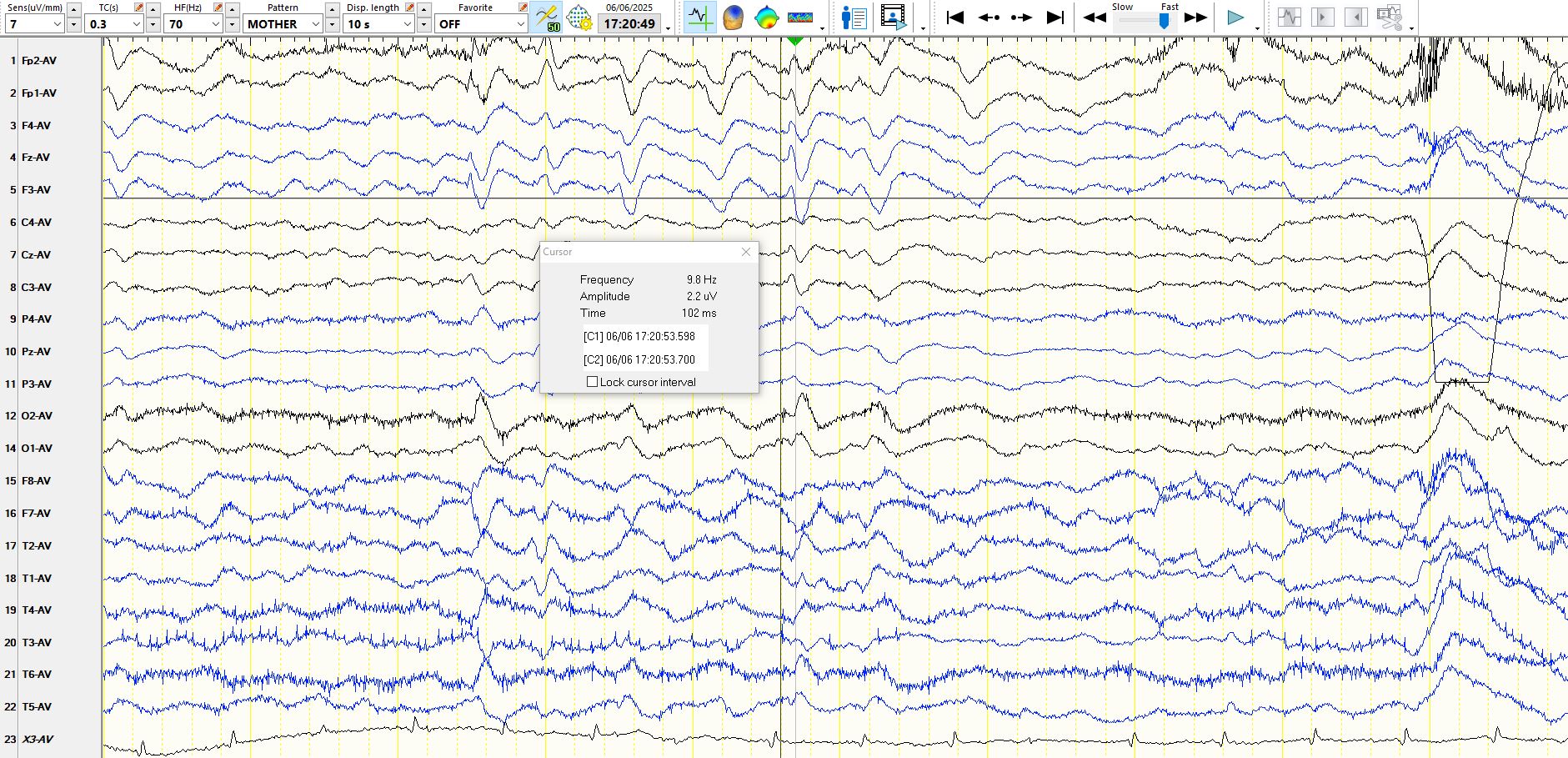
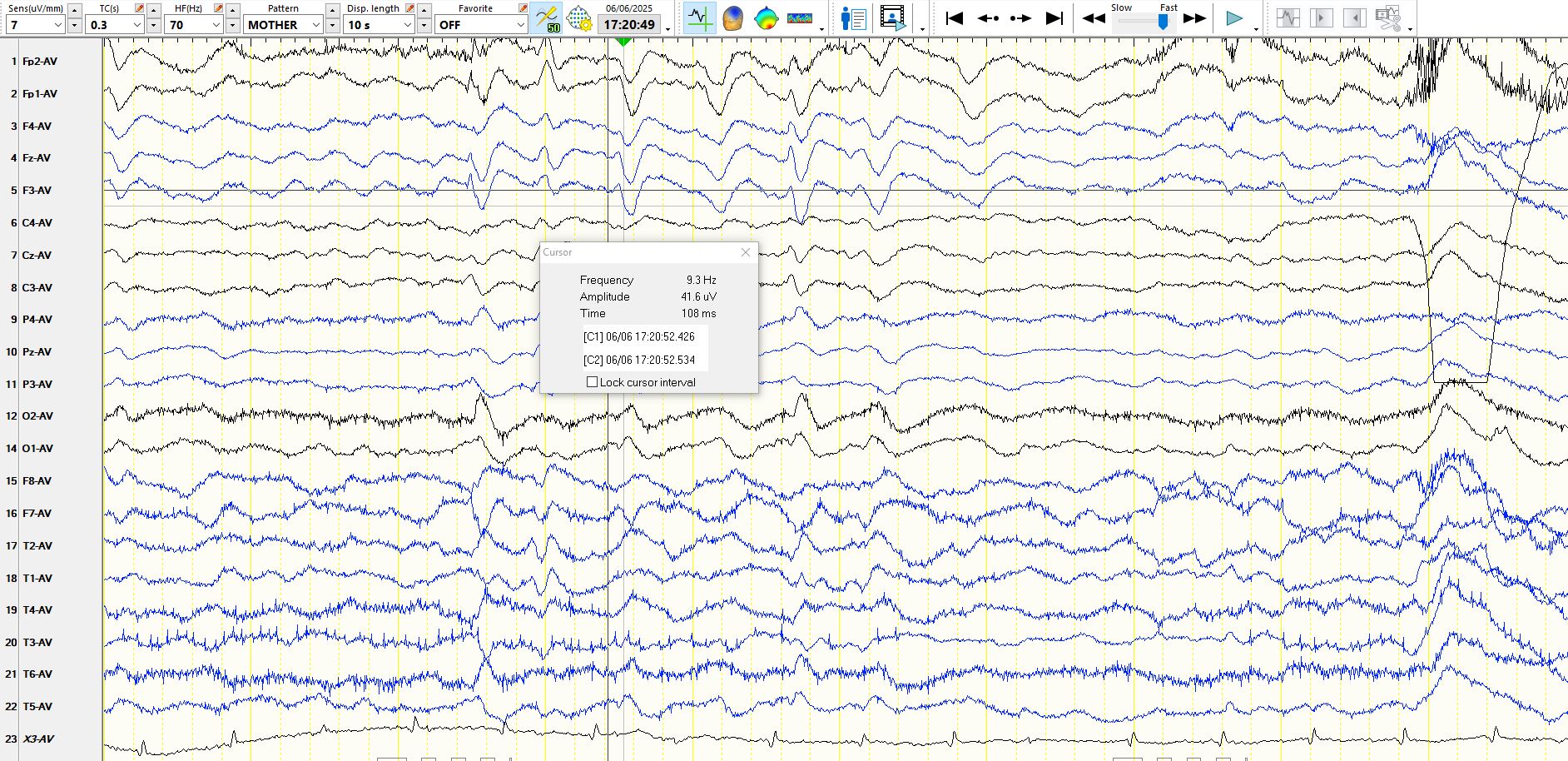
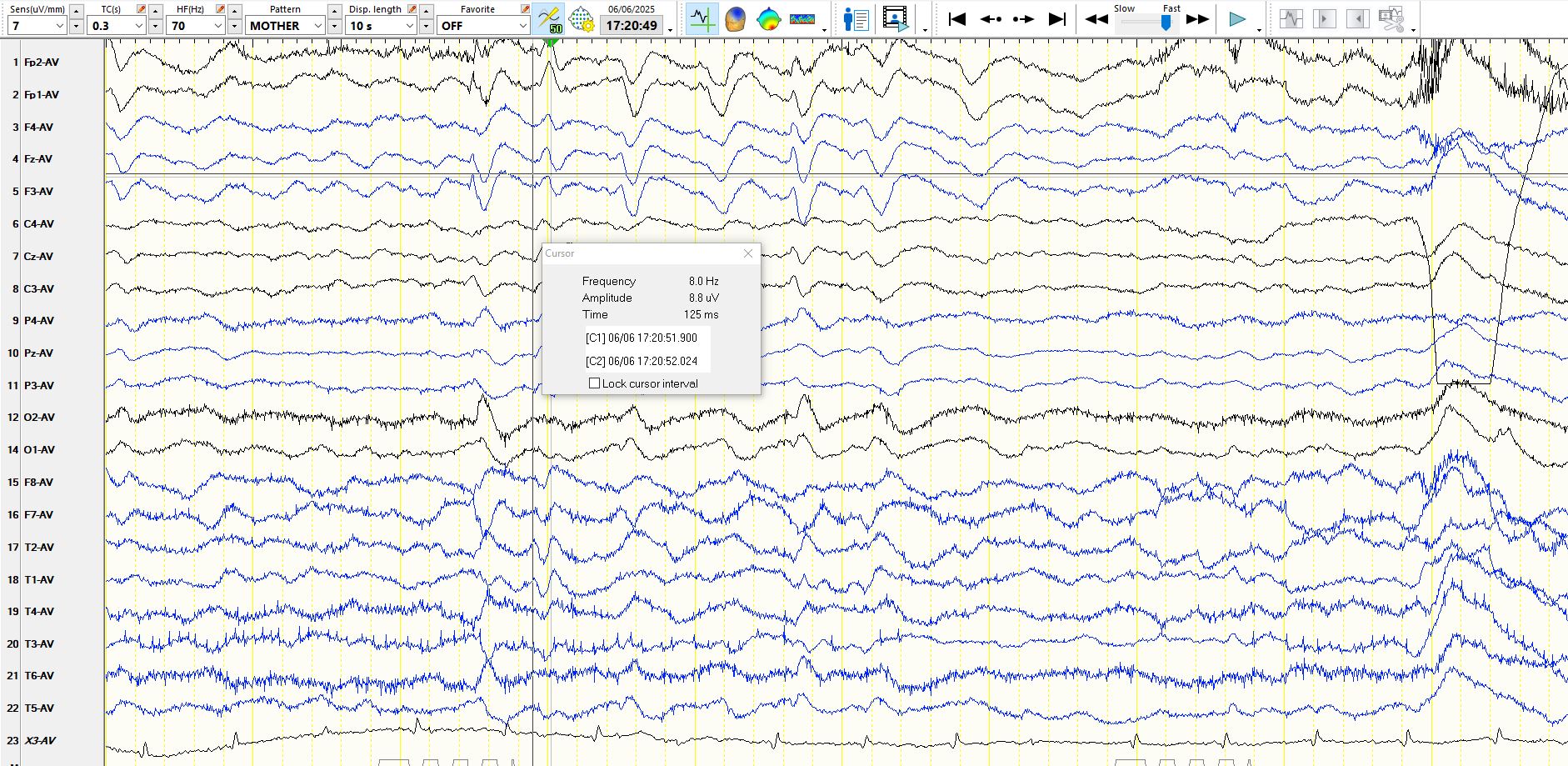
Measurement confirms the hypothesis that the first wave represents a spike, since this wave is approximately 60 msec in duration. By contrast, triphasic waves last 300-600 ms and the first component is typically about 100-200 ms.
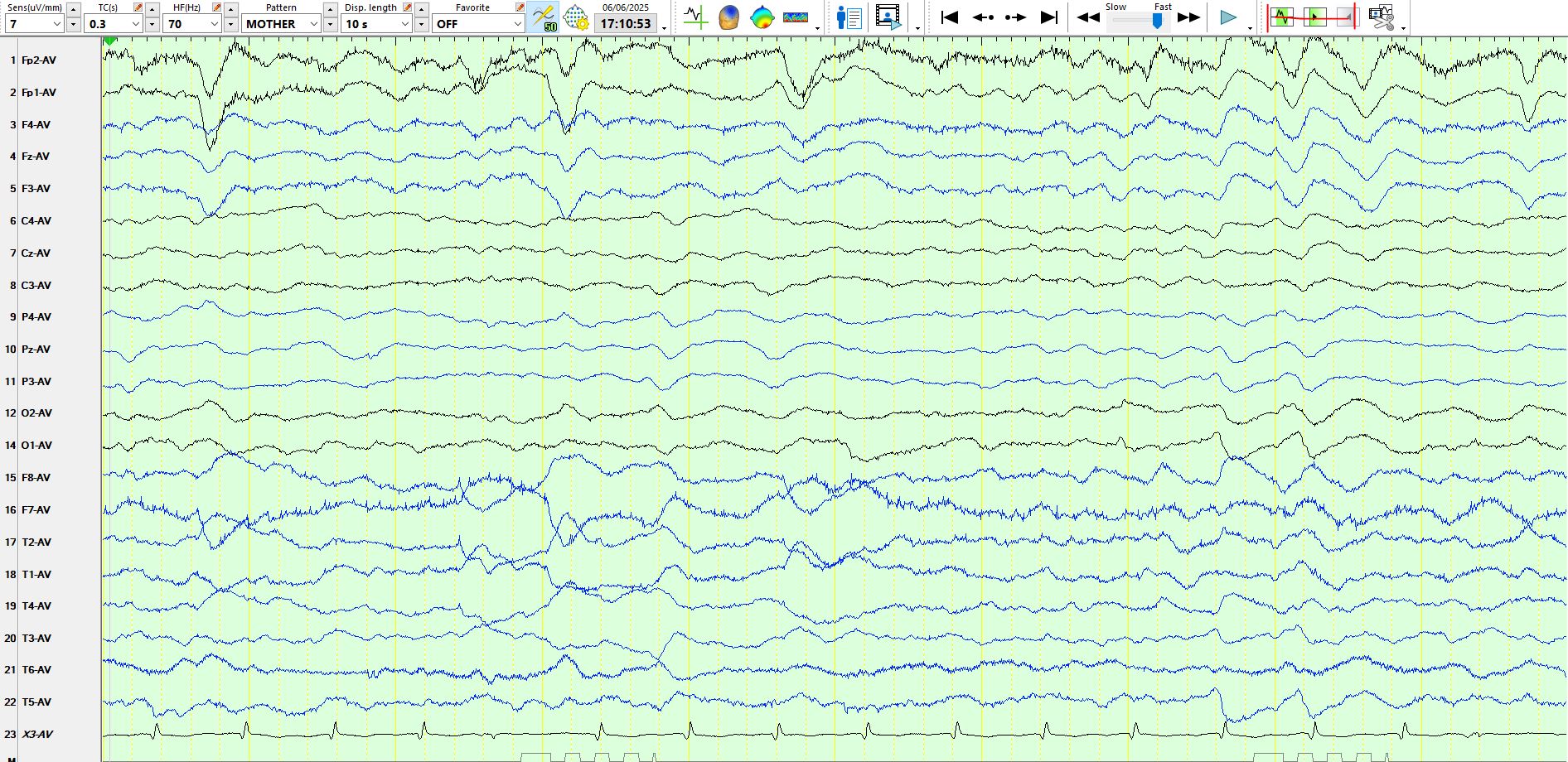
The following waves from the same short EEG represent triphasic waves, I would argue, as these meet the criteria for such waves and I would certainly not call these spikes or slow spike and wave. heHave a look at the following few pages:
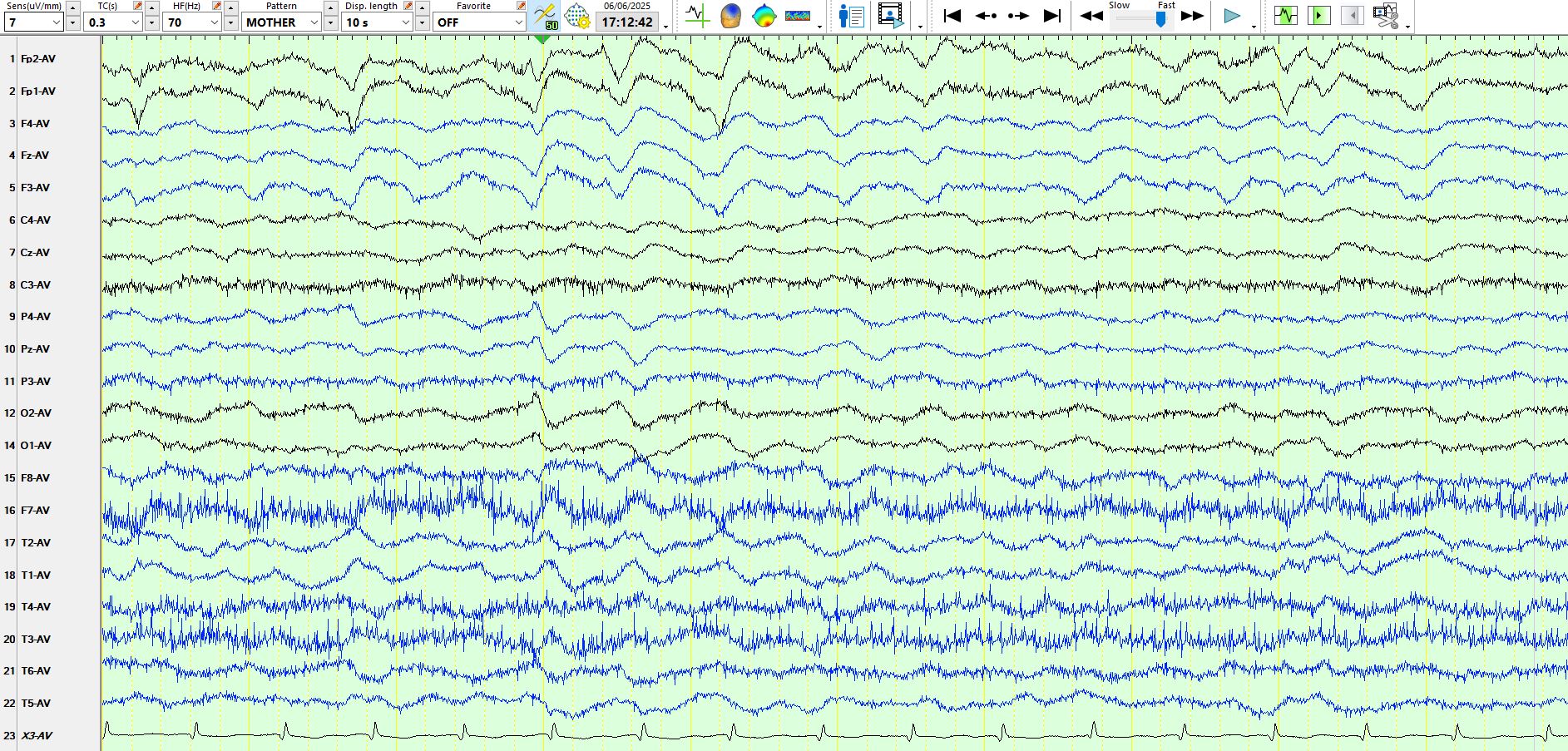
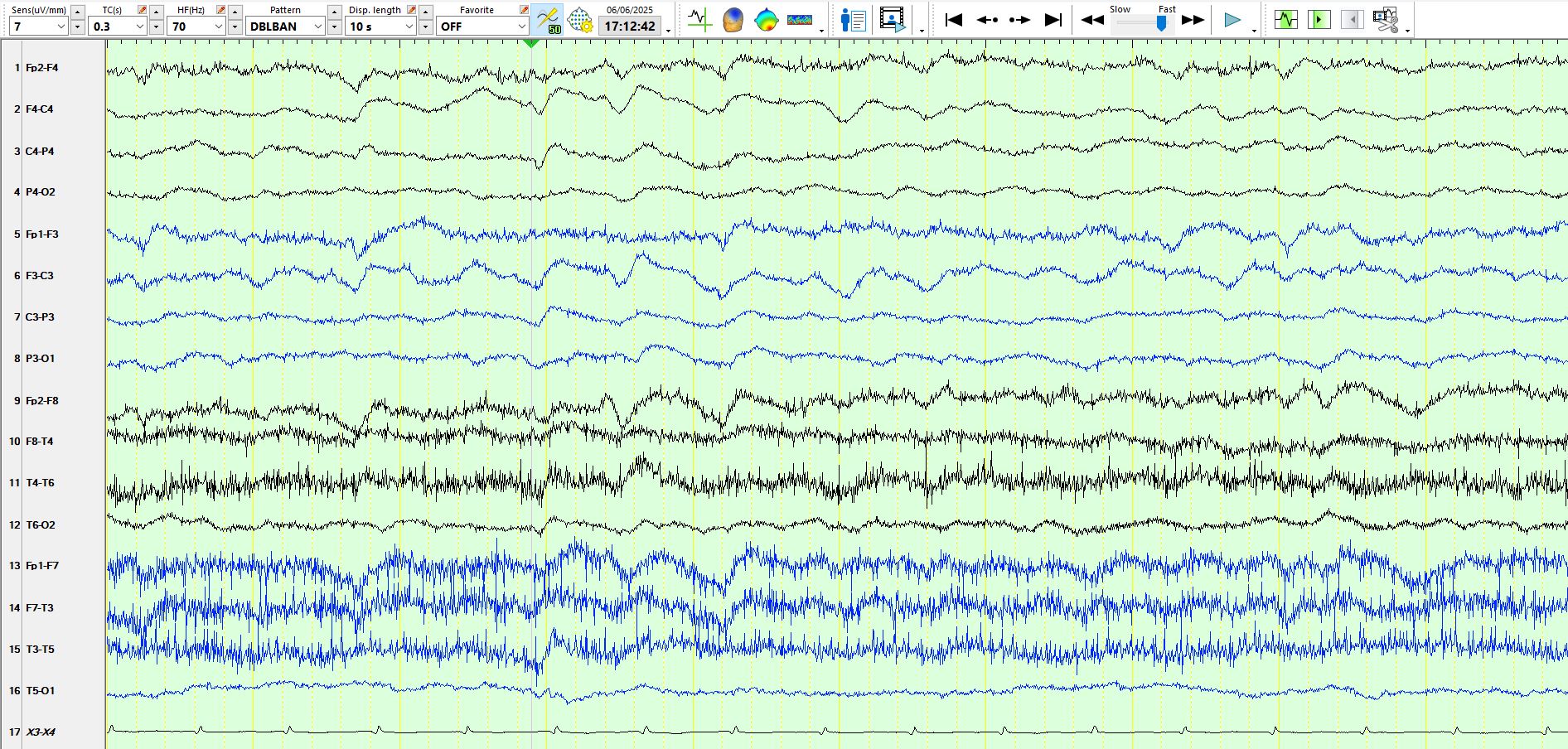
Here is the above page represented on a bipolar montage:
There is another wave on the EEG which corroborates the conclusion that the first wave in the first image above represents a spike at F3-FZ-FP1 (left superior frontal). Notice the short duration of the following wave and notice the shape of the aftercoming slow wave.

Triphasic waves have different causes. Of the three components, the second (electropositive) wave of a triphasic wave is generally the highest in amplitude. A key feature is that successive components of a triphasic wave increase in duration. A posterior-anterior delay, especially well seen on referential montages, is more common than an anterior-posterior delay, in contradistinction to their maximal expression over the anterior head regions. The above EEG therefore demonstrates evidence of a generalised encephalopathy and inter-ictal epileptiform discharges over the left superior frontal region. These are congruent with the clinical findings. The above EEG was performed on a patient who was confused, but awake and talking, albeit with frequent paraphasic errors, following a seizure. His urea and creatinine and LFts are normal.
Triphasic waves: clinical correlates and morphology - PubMed
Have there been some scientifically sound studies of triphasic waves? The following one does not consider spike-and-wave vs TWs, but instead considers periodic discharges in general
As is clear from the study, interrater agreement among experts blinded to the clinical data of EEG's demonstrating periodic discharges was no more than "fair" (kappa = 0.33) for TWs.
The above findings stand in contrast to the following study:
Generalized Periodic Discharges With and Without Triphasic Morphology - PubMed
In this study agreement for the presence of triphasic waves was moderate (kappa = 0.6he7).
Here is some sensible, recent commentary on triphasic waves
EEG Triphasic Waves - StatPearls - NCBI Bookshelf
Atypical or Typical Triphasic Waves-Is There a Difference? A Review - PubMed
PS: I have seen a few patients with Angelman syndrome who have near-continuous triphasic waves; the first one that I ever saw caused me to consider the possibility that the patient was in nonconvulsive status epilepticus! Needless to say, I treated the patient aggressively with oral antiseizure medications, with no benefit and therefore reverted to continuing the patient's usual antiseizure medication.
Over the years I have noticed triphasic waves during the postictal period of a few patients in the epilepsy monitoring unit. This is not oft documented and no doubt you might argue that I'm incorrect in my interpretation of these waves. This is the problem with the anecdote. There is one article describing the same, but I could find no others in a search in the National Library of Medicine.