
The best bipolar montage? Mu rhythm?
Dec 13, 2025As mentioned in previous posts, I prefer the coronal bipolar montage to the anterior-posterior bipolar montage for several reasons. The following page illustrates one of the reasons:
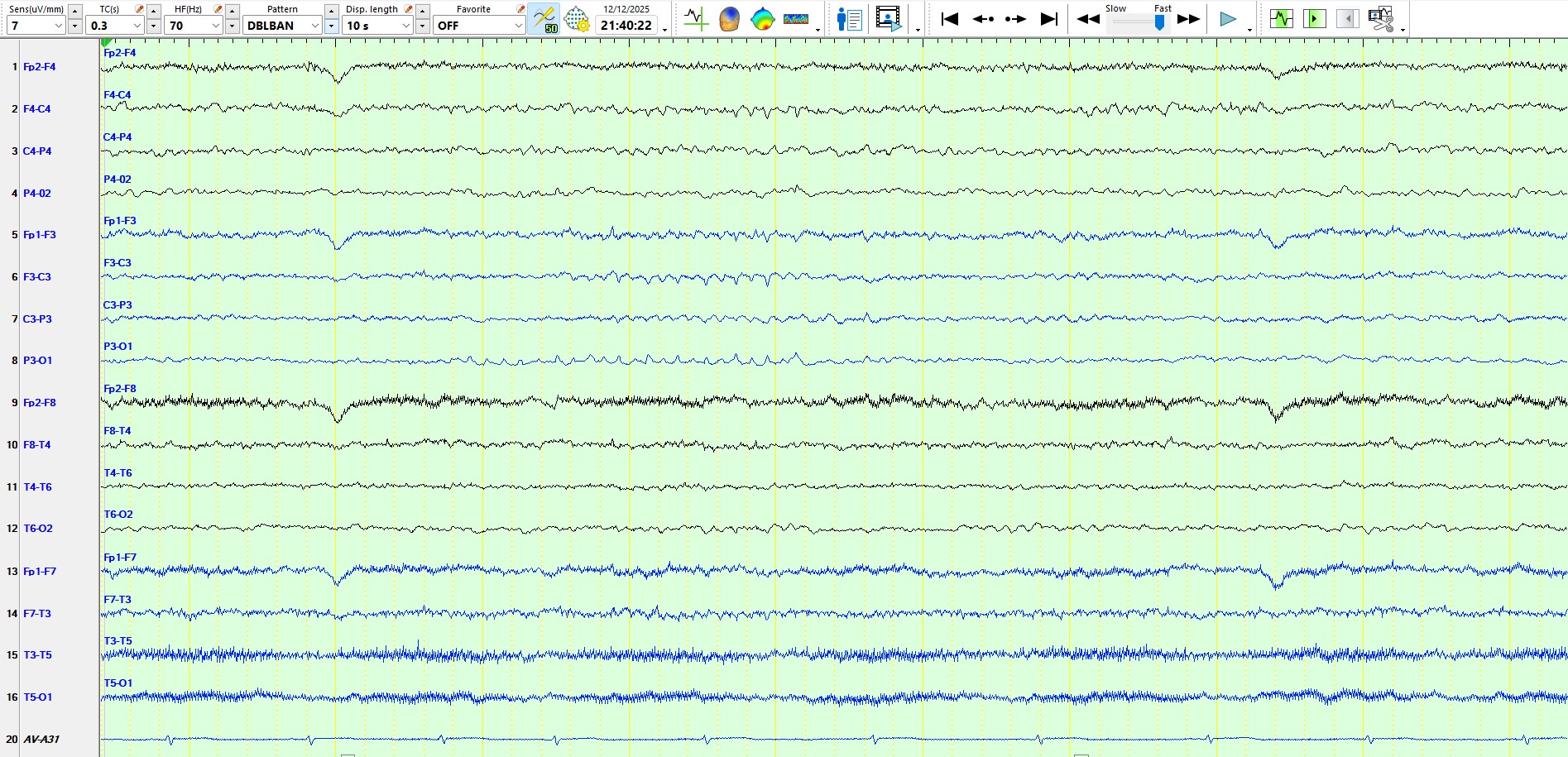
The following pages show the same 10-second epoch on three different montages:
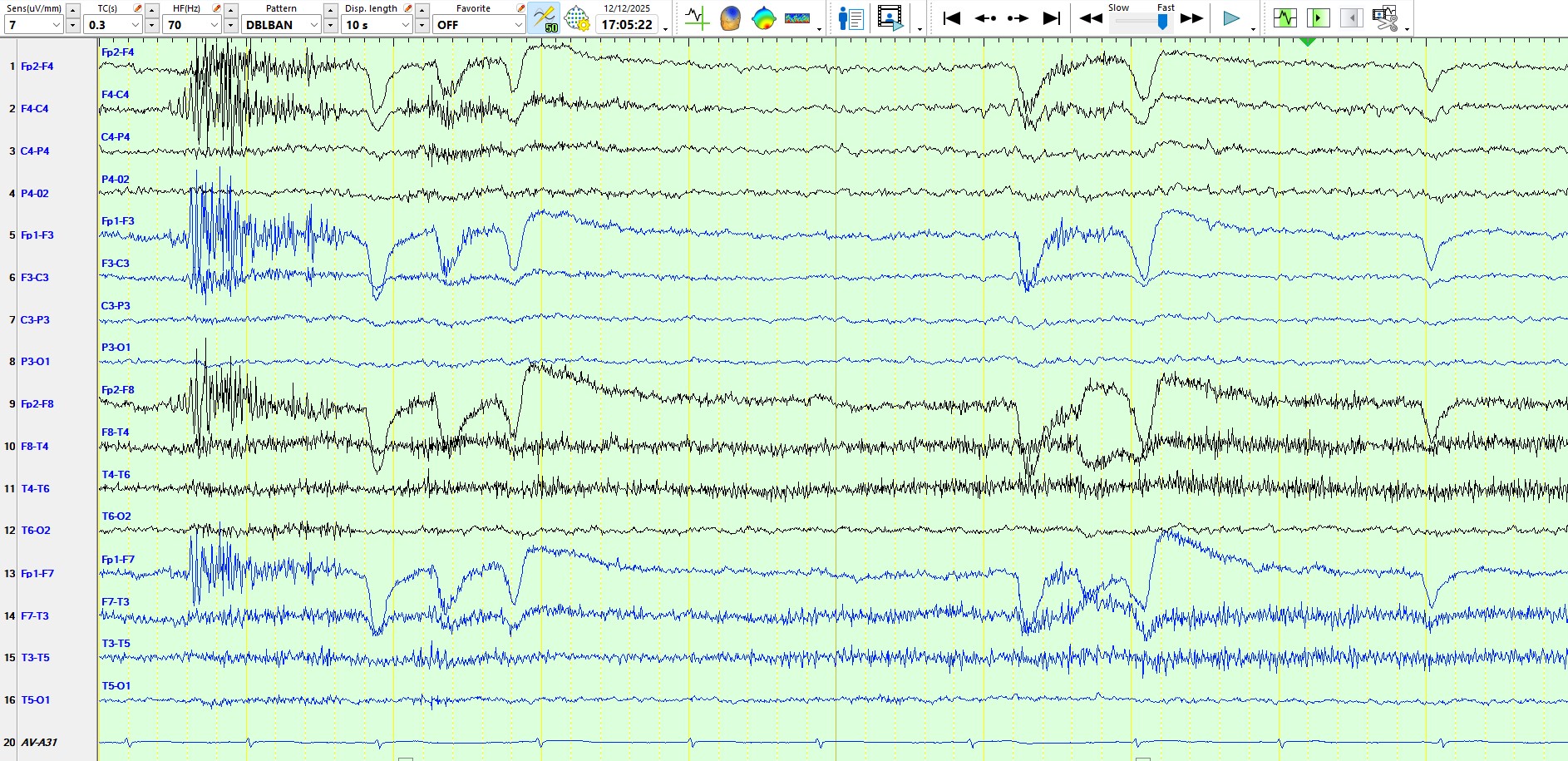
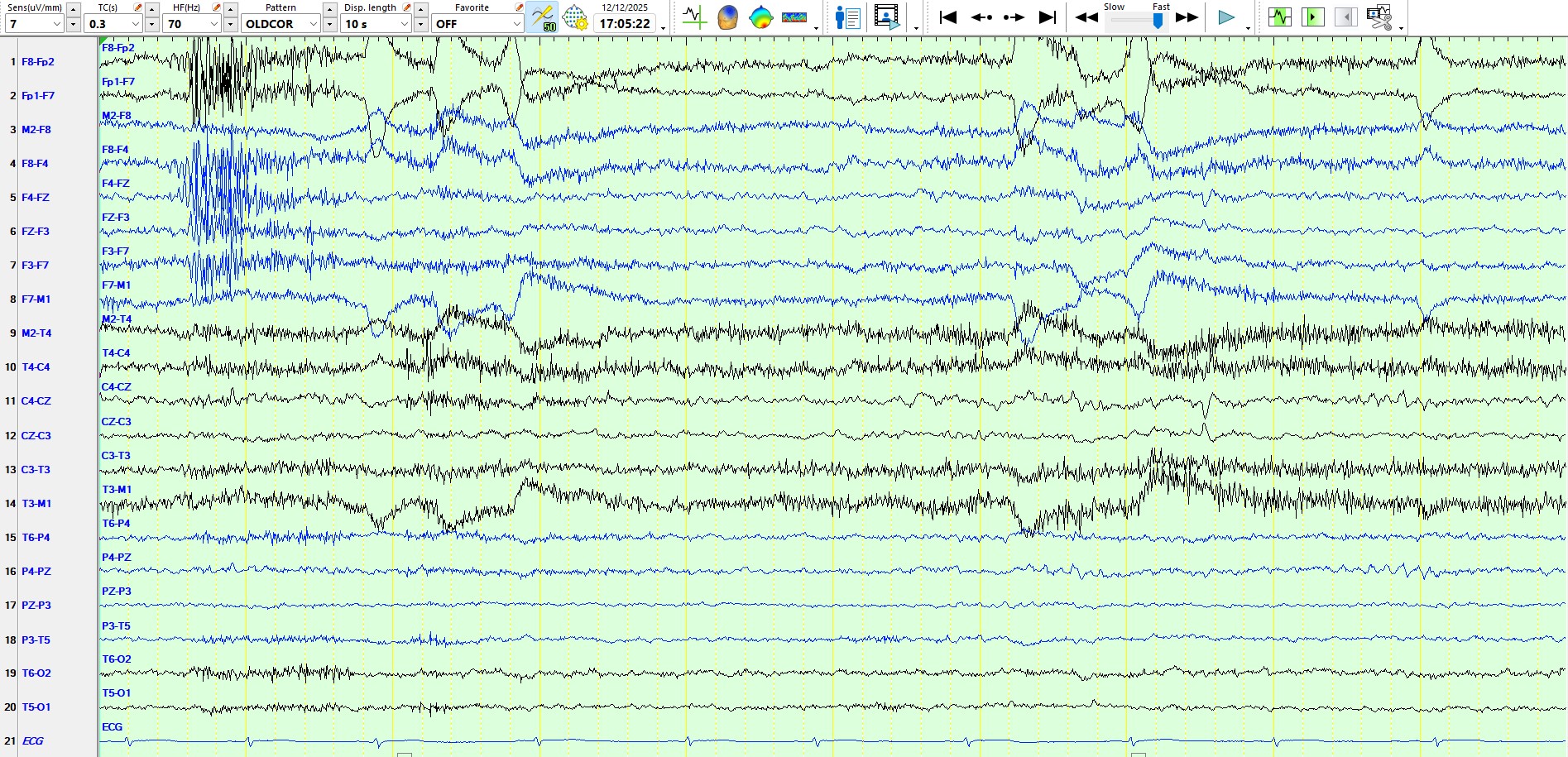
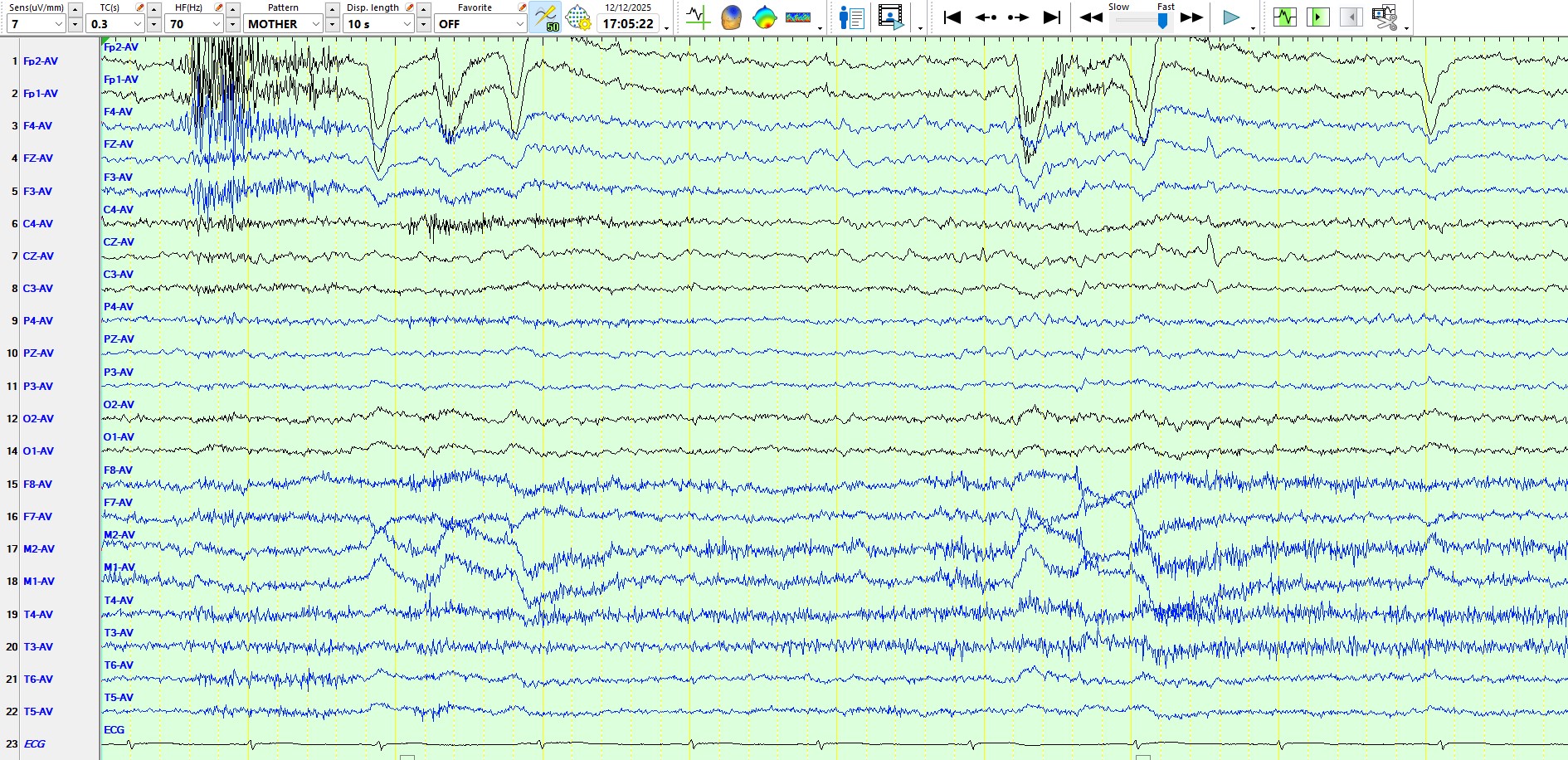
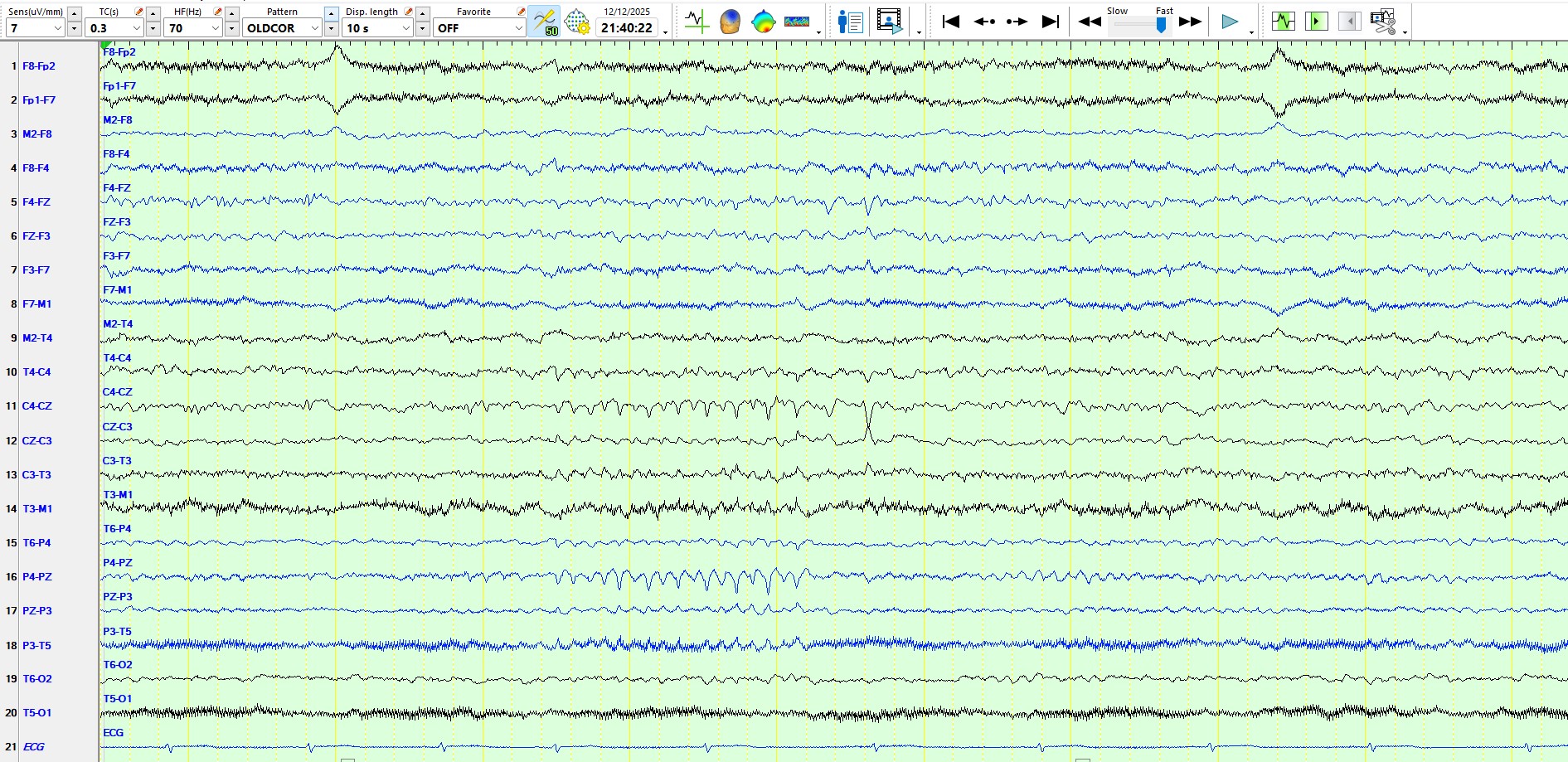
This patient has spikes at CZ-FZ that cannot be seen on the bipolar anterior-posterior montage, simply because this montage excludes cortex adjacent to the midline. In this case, the central sagittal spikes can be clearly seen on the bipolar coronal and the referential montages.
The following represents a different page:
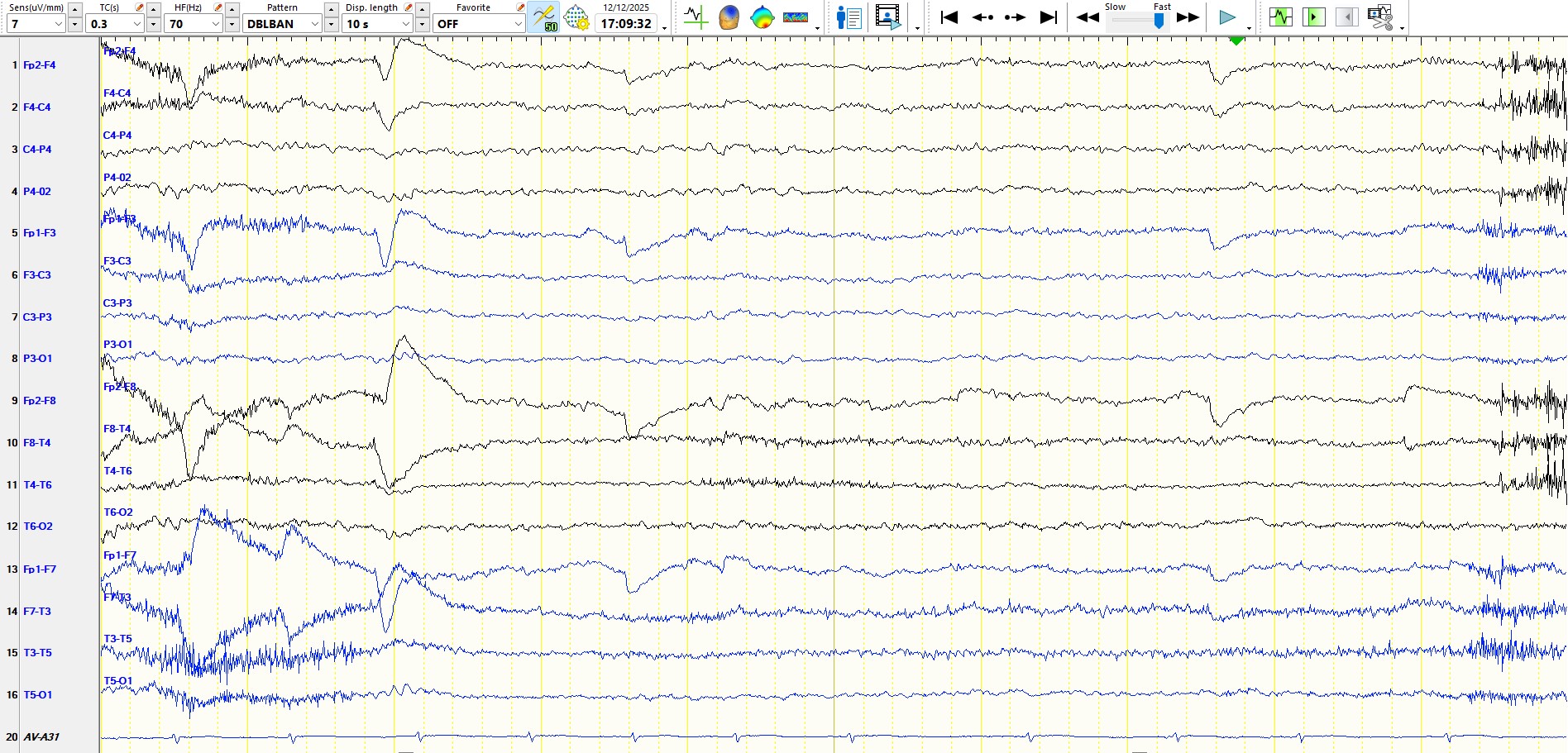

The bipolar anterior-posterior montage again misses spikes. Would a neuroradiologist accept an MRI scan that excludes axial sequences of the top of the brain? Should one exclude this part of the brain from the default montage when reviewing an EEG?
Is the following an example of alpha rhythm or mu rhythm?
The following is the same page as above, represented on the coronal montage:
The following is the same page as above, represented on the referential montage:
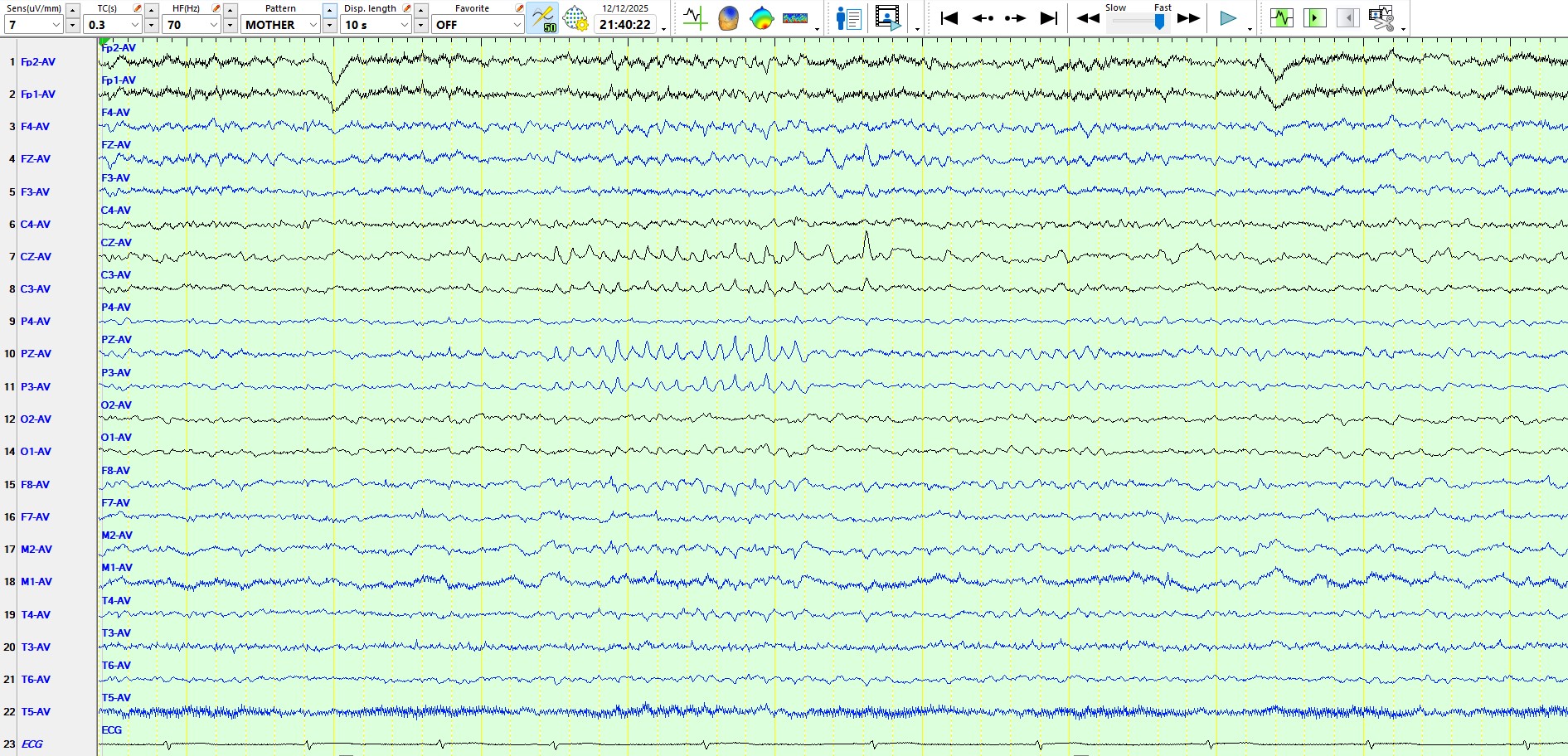
The answer? Neither of the above possibilities. This is a train of spikes, arguably representing a brief electrographic seizure, admittedly less than 10 seconds. There is evidence for the latter statement; the following is the onset of a clinical seizure, commencing with motor symptomatology in the LEFT foot:
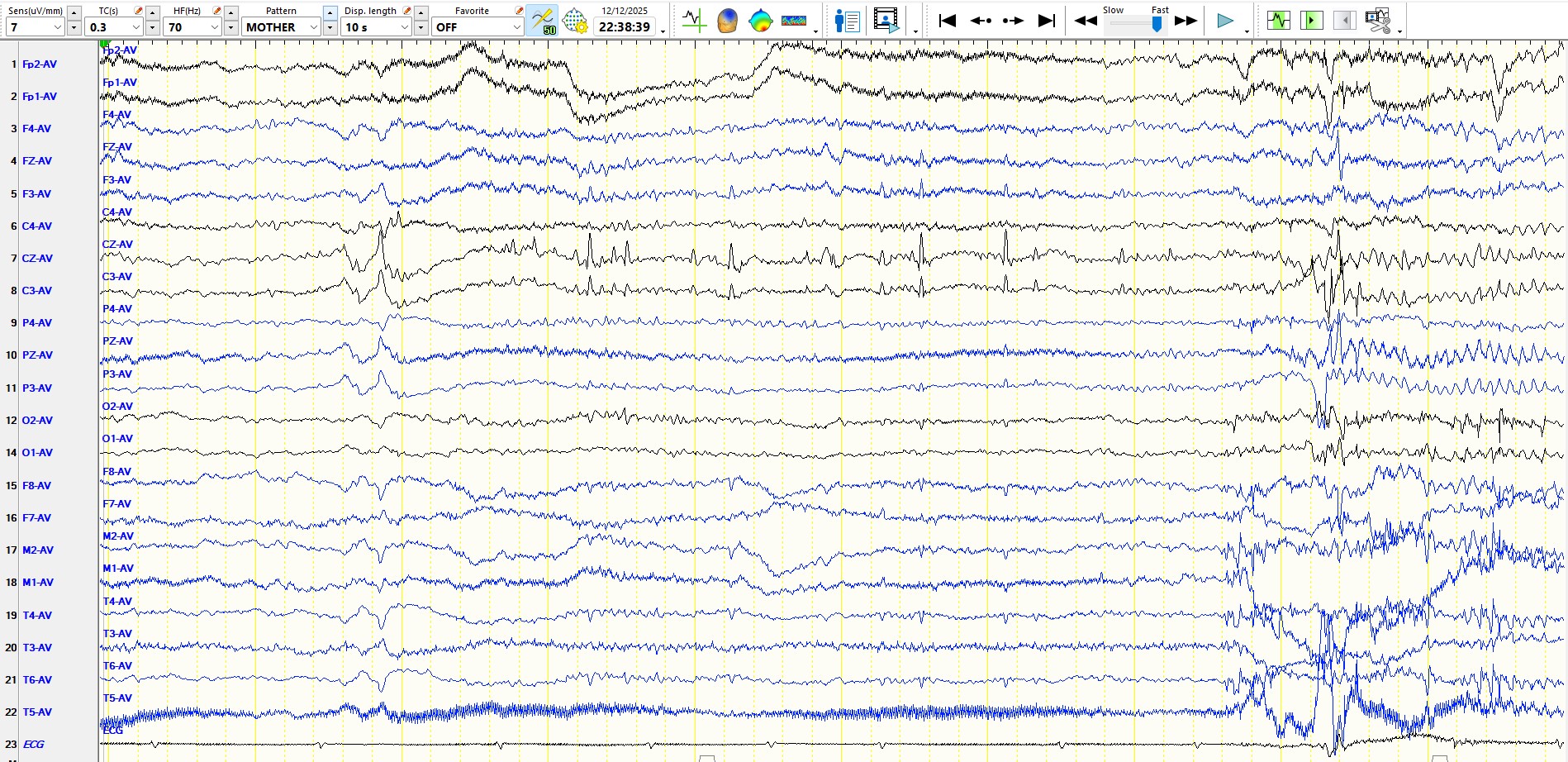

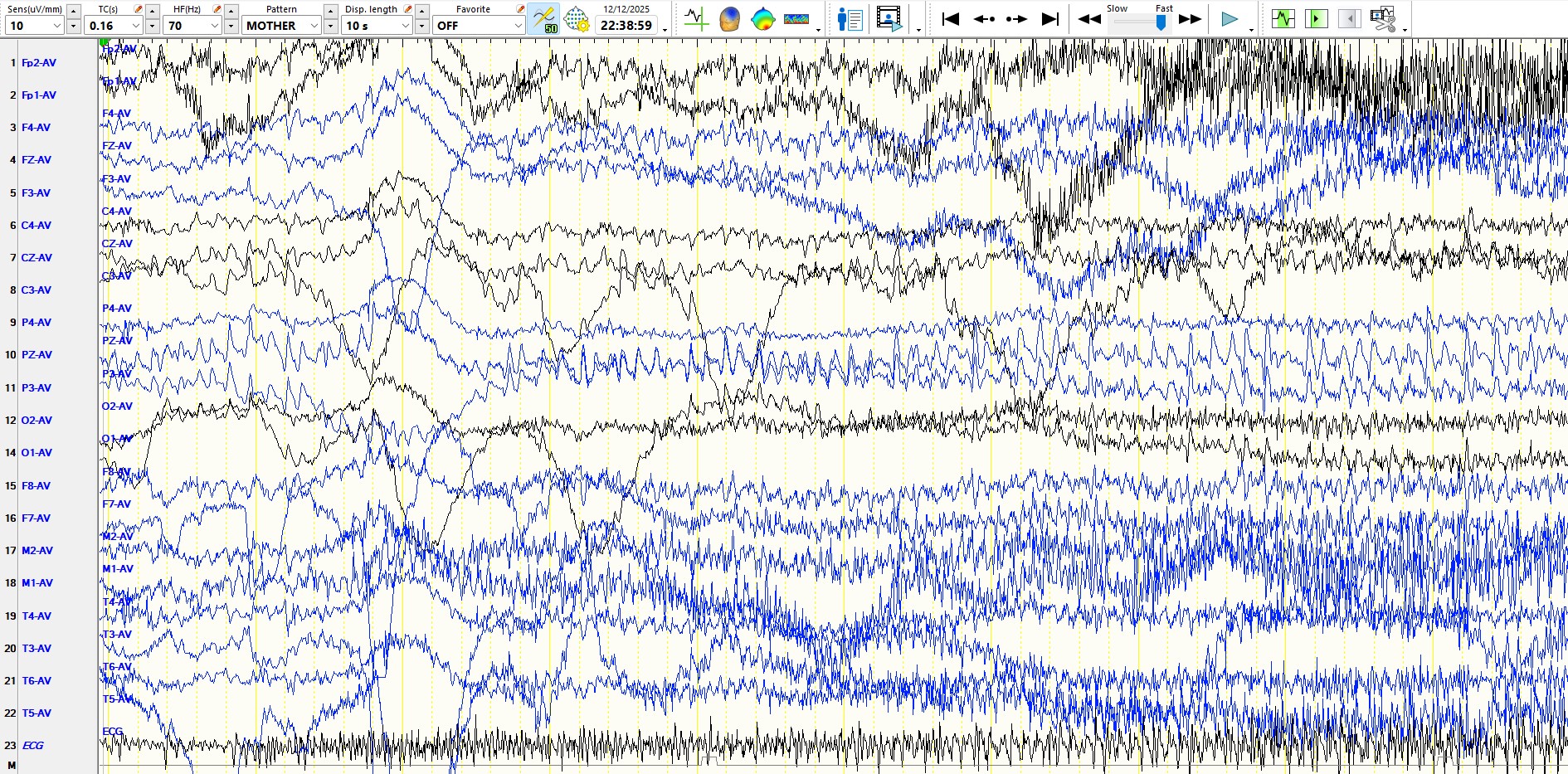

As should be evident from the above pages, this seizure commences as an alpha frequency discharge in the same derivations, at the same frequency, and with the same morphology as the inter-ictal/electrographic discharge seen further above. The latter, therefore, does not represent alpha or mu rhythms. Incidentally, the "electrographic seizure" shown above exhibits subtle but definite evolution. If in doubt, have another look at it.
You should then ask the question, Why is the discharge best seen on the left? There are three possible explanations. First, there is a possible transposition of the relevant or even all right and left hemispheric derivations (by carefully analyzing the EEG with the video, especially at times of different artifacts, this possibility can be excluded). Second, perhaps the seizure discharge originated in the left medial central cortex, representing function for the right foot, with oblique propagation to the right central convexity. Third, perhaps there is structural damage to the cortex in the right parasagittal convexity, precluding expression of the seizure discharge from within the superior right frontal-central-parietal convexity. There are several reasons why the third possibility explains the apparent discordance between the EEG and the clinical manifestations. First, notice that the interictal EEG recording demonstrates relative suppression of background rhythms over the left central-periatal region. Second, the patient has a spastic hemiparesis of the left leg and, to a lesser extent, of the left hand and arm. Third, the MRI scan demonstrates evidence of cavitation (loss of cortex) within the superior aspect of the right frontal-central-parietal convexity, related to a haemorrhagic stroke that occurred at the age of seven years:
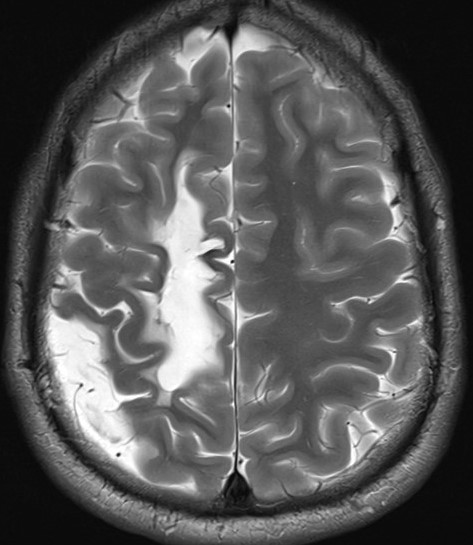
It should be clear from the MRI scan why the left leg is disproportionately severely involved when compared to the hand and arm, and you may appreciate why the seizure appears over the convexity of the left hemisphere, contralateral to the side of origin of the seizure within the right mesial hemisphere. Hence, the second and third possible explanations are correct.