
Temporal lobectomy 11y ago
Jul 29, 2025The following is the recording from a 40+y patient, who has been seizure-free for 11 years. Over the past 1-2 years his/her memory has objectively declined, prompting further investigation. The 24-hour EEG was done to look for the possibility of subclinical temporal lobe seizures. The patient lives alone and hence amnestic seizures might not be known to him.
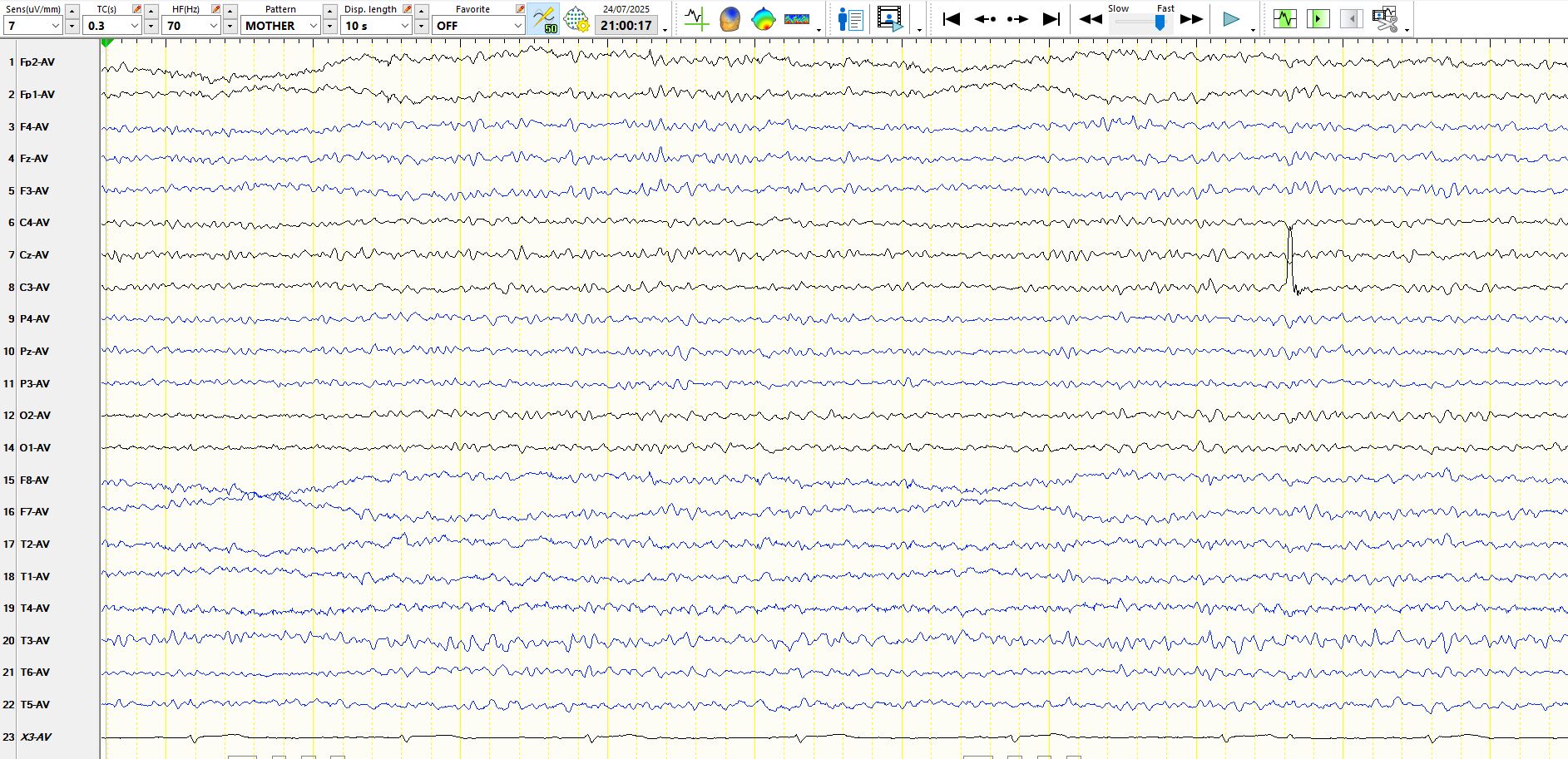
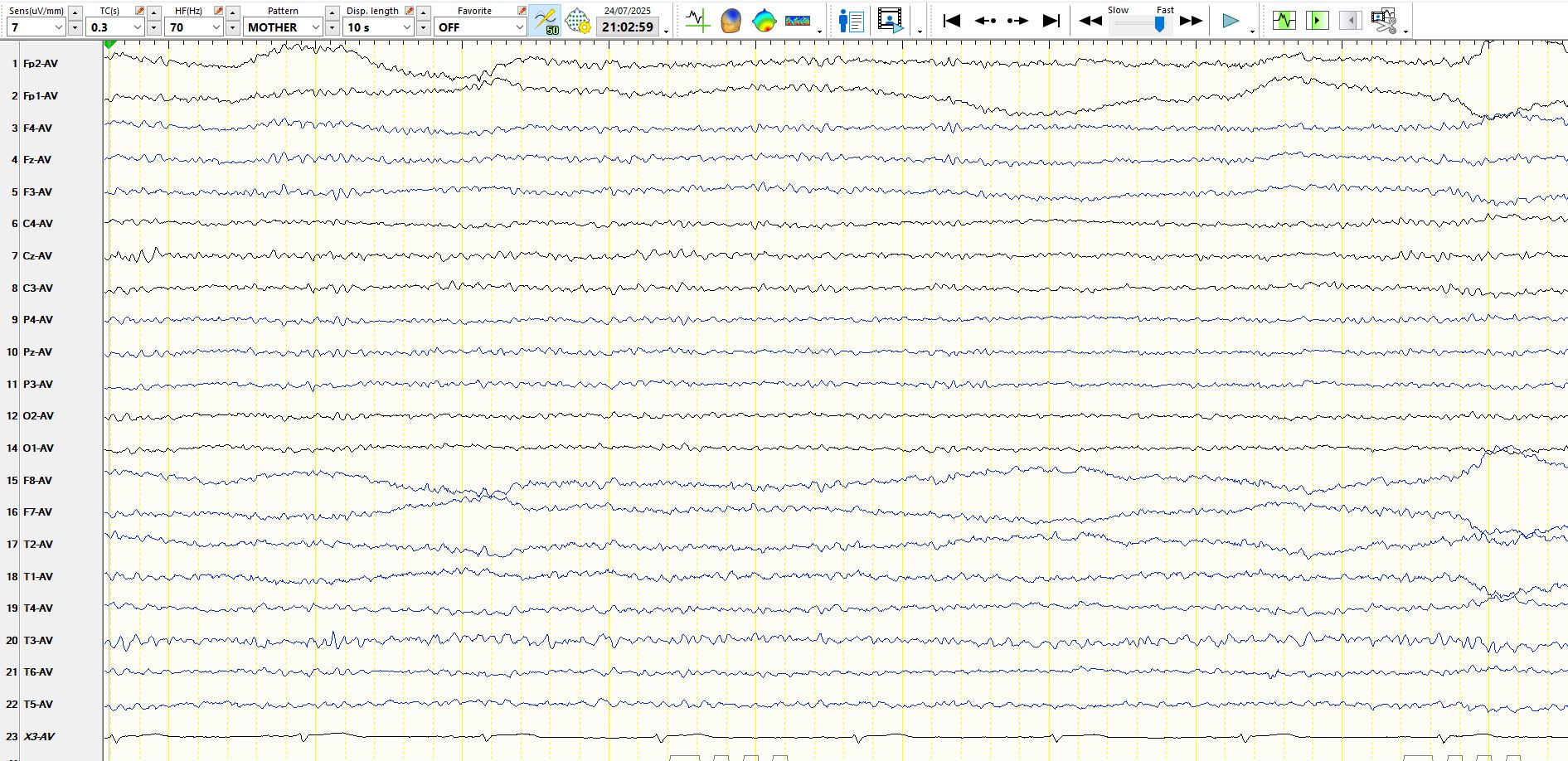
The only salient finding is of a breach rhythm at T3. The breach rhythm is characterized by a combination of beta and theta frequencies, which are physiological frequencies that are disproportionately high in amplitude by virtue of the breach. The importance of identifying a breach rhythm is to avoid the problem of interpreting theta waves and apiculate waves as abnormalities, when these are simply the consequence of a breach rhythm. A good rule of thumb is to avoid interpreting apiculate waves over a breach as spikes, unless there is compelling corroborative evidence, such as the presence of unambiguous spikes in adjacent derivations and discharges that markedly exceed the highest amplitude waveforms in the derivation overlying the breach rhythm. You need to look at the EEG in its entirety to determine the latter.
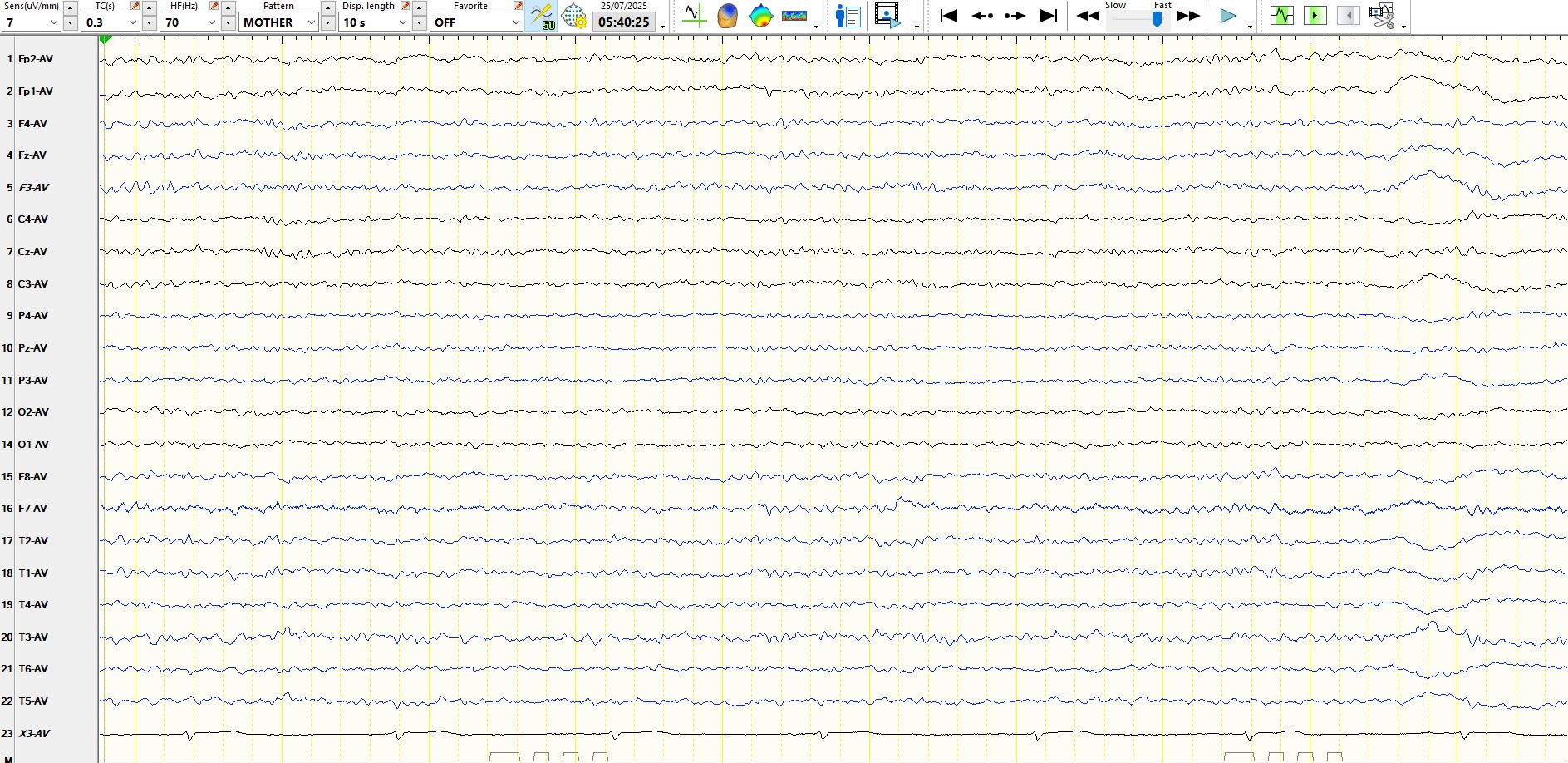
Below is an example of a sharply contoured theta wave that you can safely ignore; It appears just above the first ECG beat. They might get a lot sharper than this. Notice that this wave has a large field. The patient's heart rate is slow by virtue of a lot of exercise.
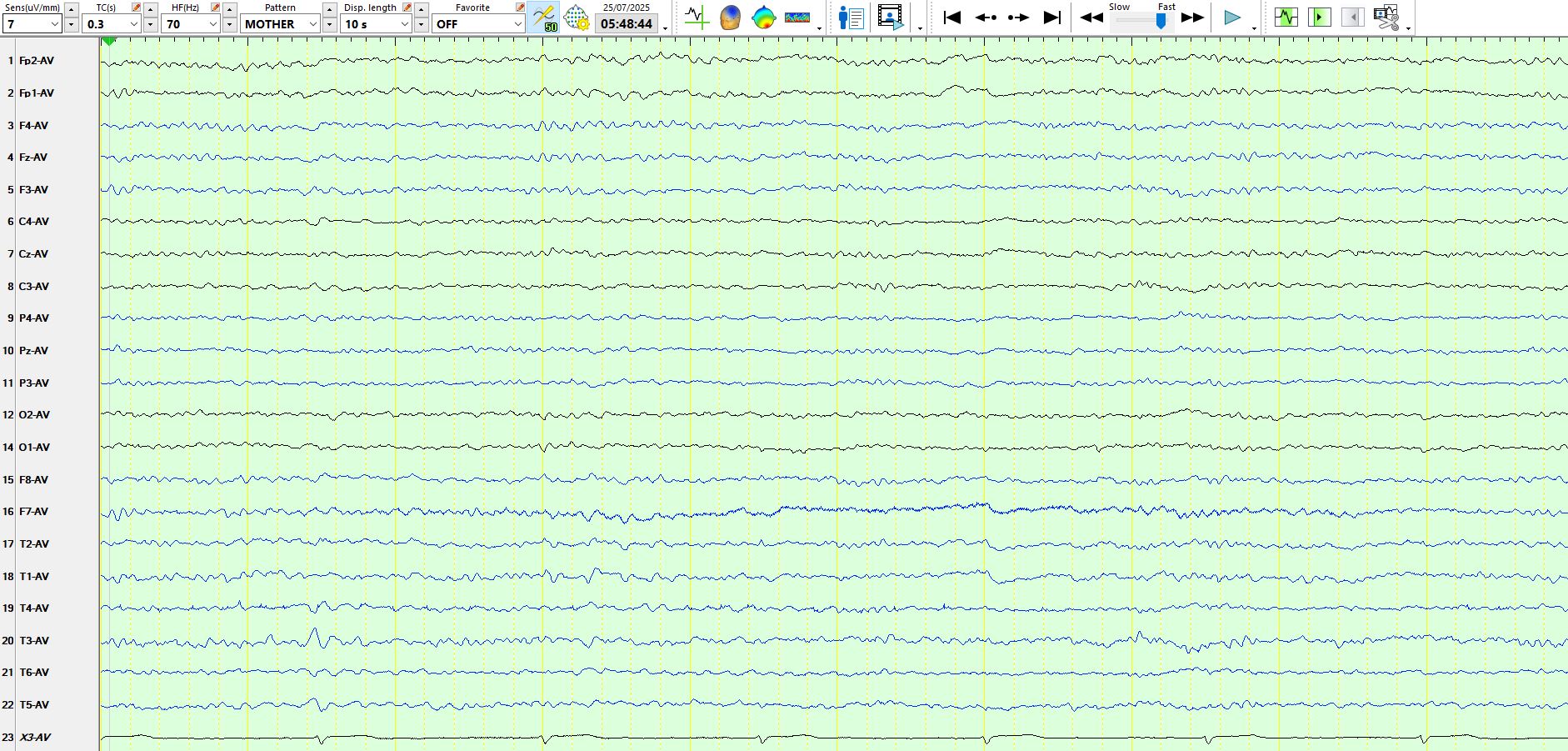
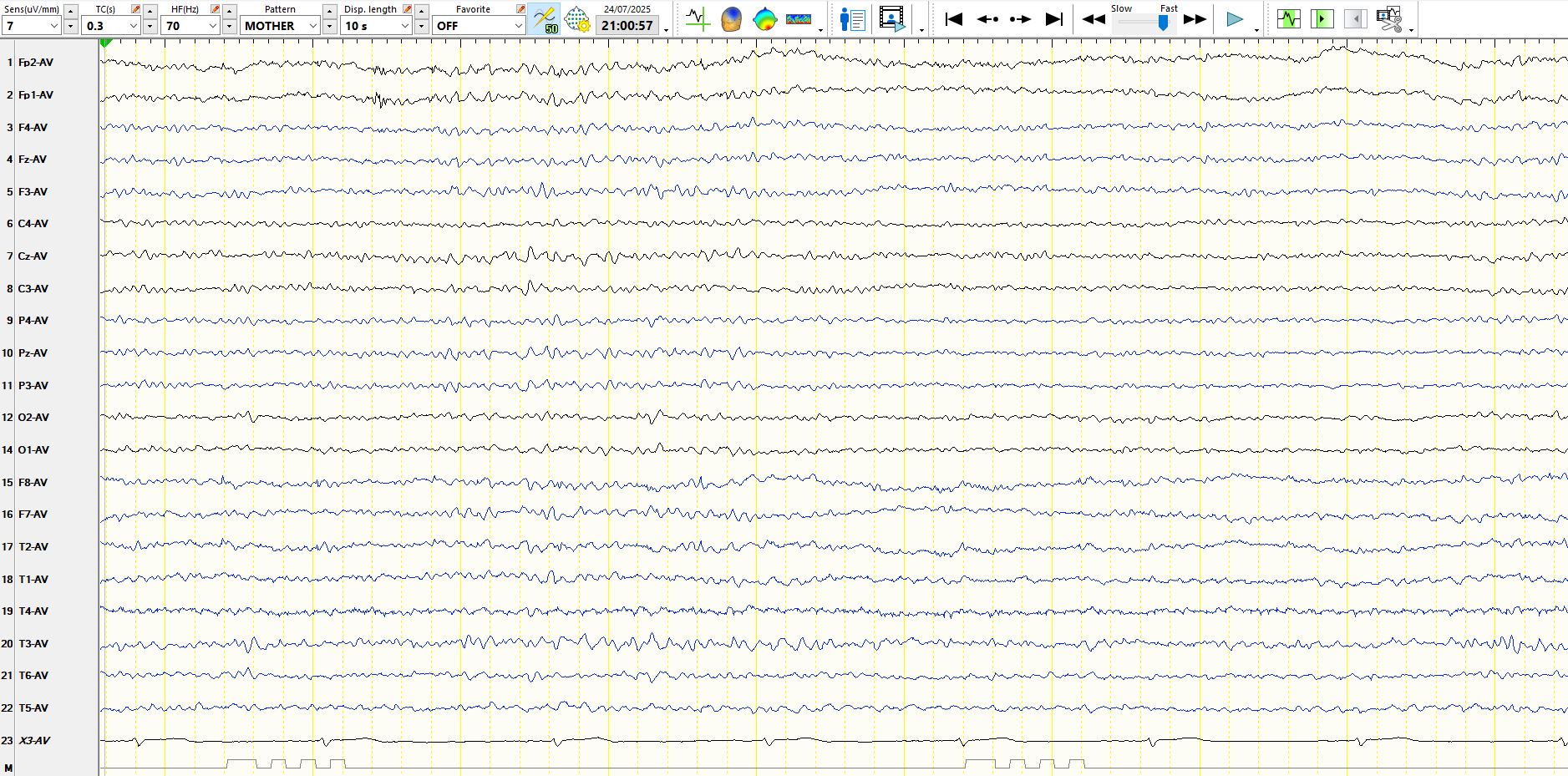
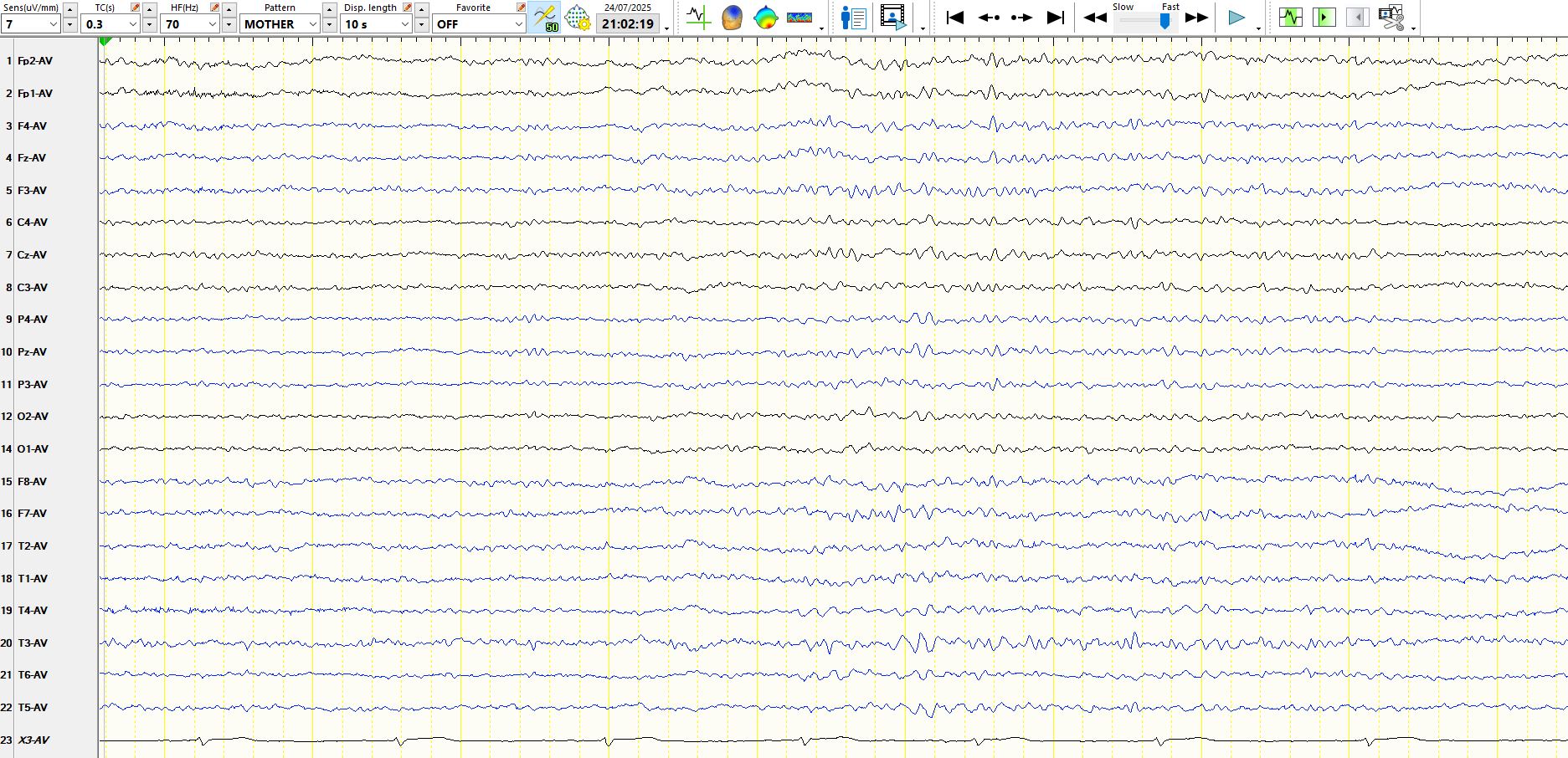
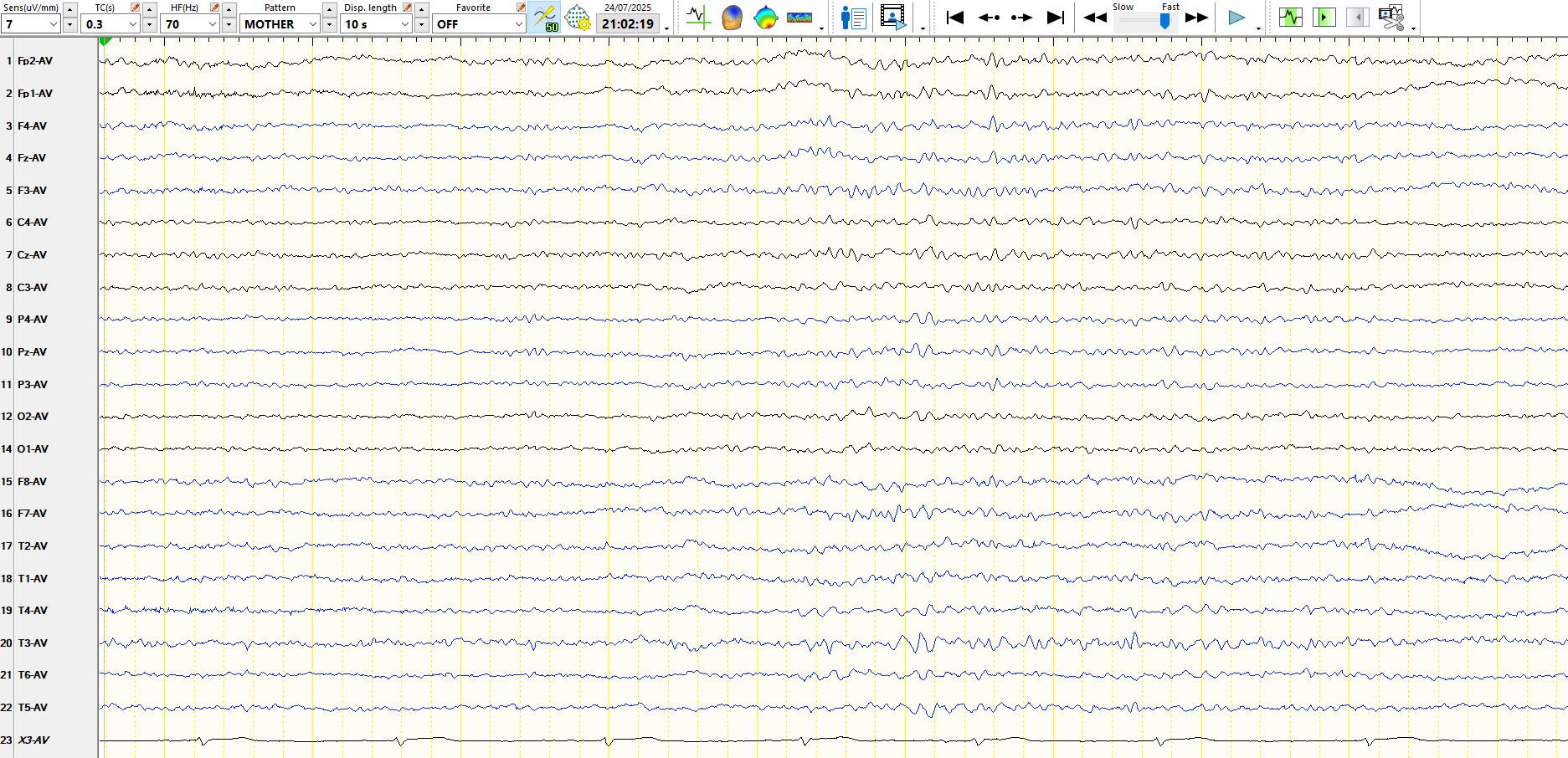
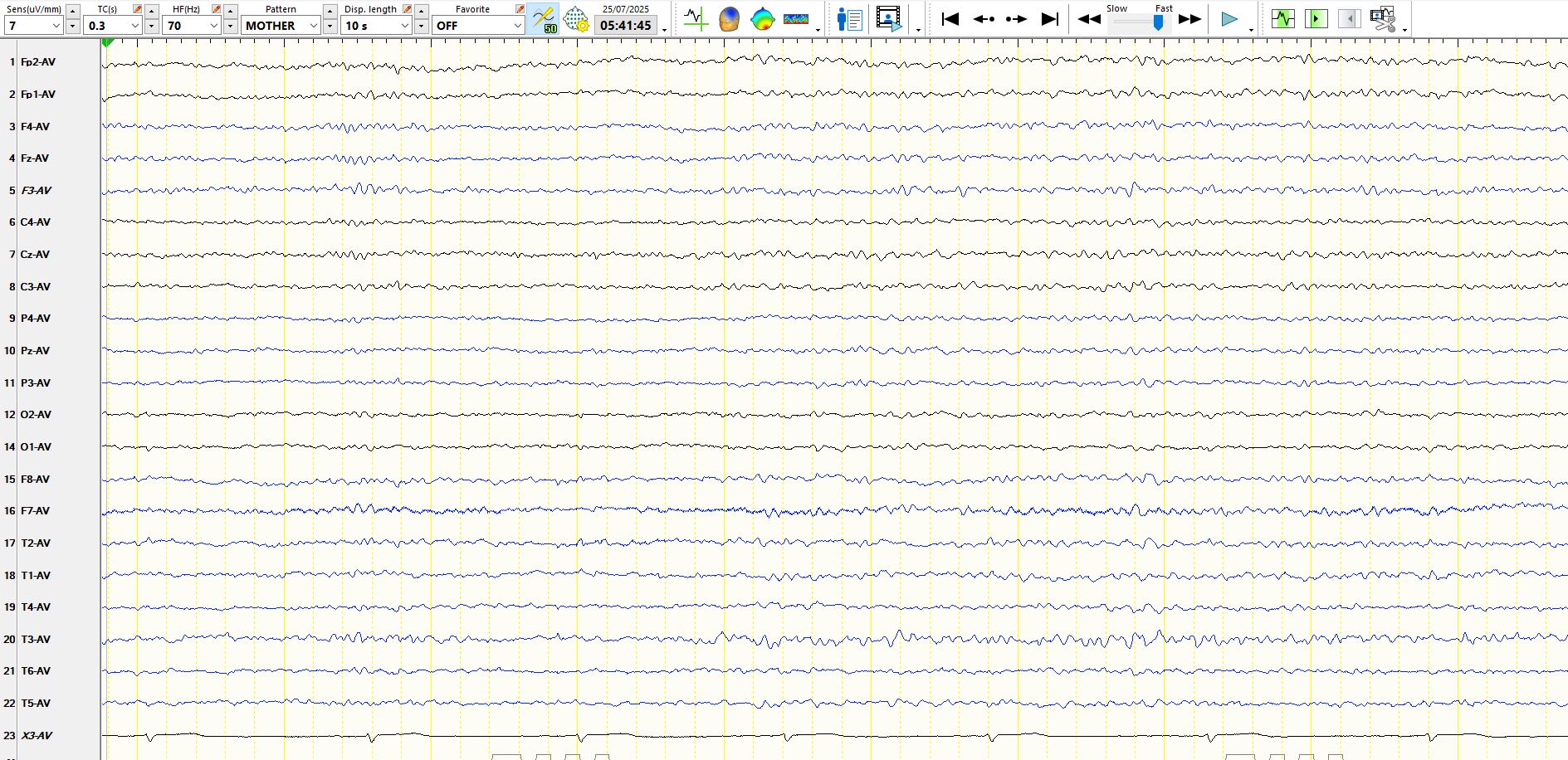
The following is not the best example of such waveforms, but you might get the idea by looking at the waves denoted by the red line. The breach rhythm can be clearly seen.

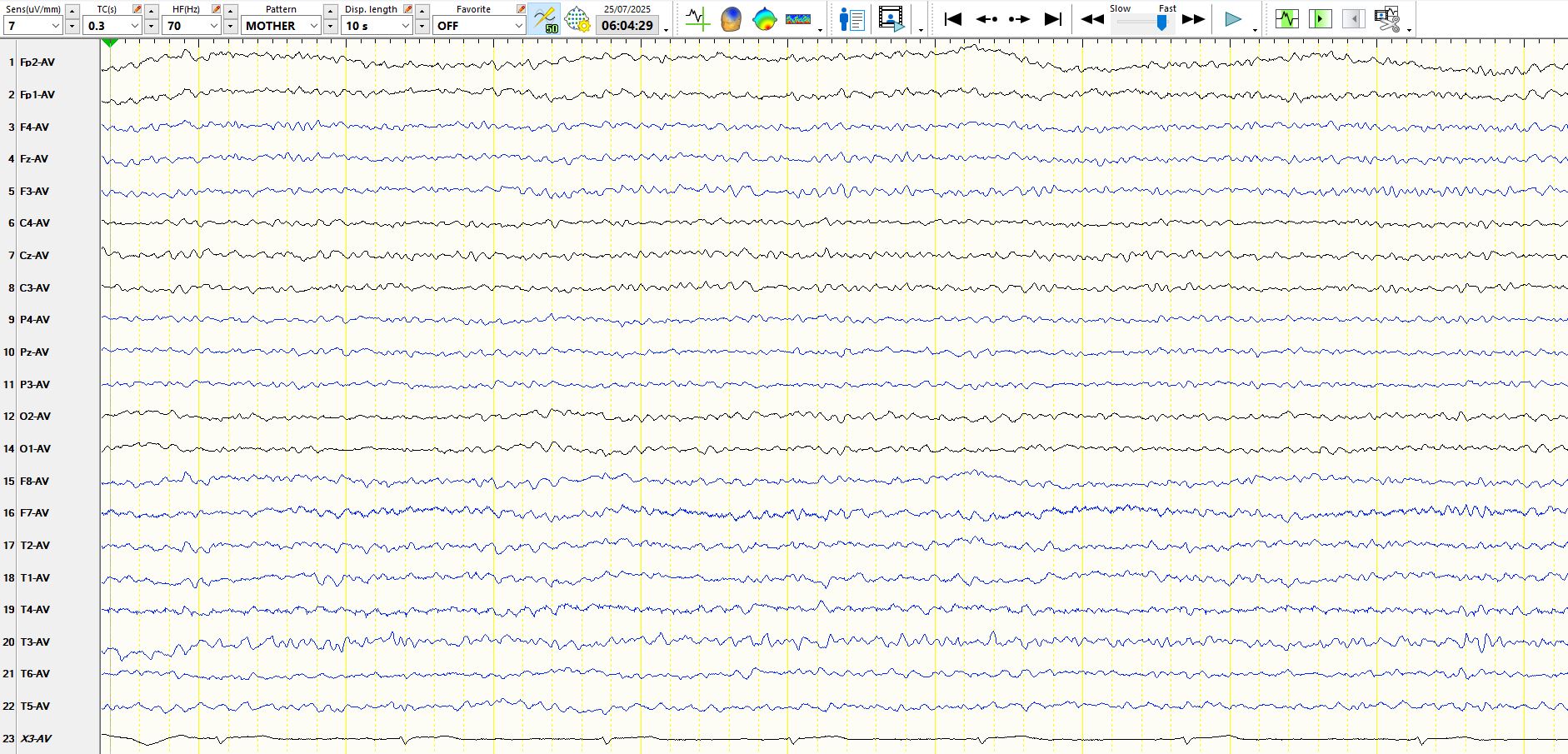
The bottom line? Keep an eye out for breach rhythms or run the risk of over-interpreting the nature of various waveforms over a breach.
PS: He fortunately has another cause for his memory decline and this is reversible.