
Seizures are primarily about neurophysiology and not about neuroradiology
Aug 30, 2025Medial temporal sclerosis (or mesial temporal sclerosis) is essentially a pathological diagnosis; high quality MRI scans interpreted by experts who work in the field are strongly predictive of the pathological finding, but there are several reasons for separating the radiological and pathological diagnoses. The most important is a practical consideration, namely that, as a general rule, radiologists often get the diagnosis wrong, calling it when it is not present and also not calling it when it is present. This is not a criticism of anyone, simply a reflection of the usual problem in medicine of sub-specialisation, a skillset in a particular aspect of neuroradiology and having the gold standard of pathological verification. Hence, be particularly circumspect about this diagnosis on MRI reports. To complicate matters further, there are different types of medial temporal sclerosis:
International consensus classification of hippocampal sclerosis in temporal lobe epilepsy: A Task Force report from the ILAE Commission on Diagnostic Methods
To get to the point about neurophysiology, even when correctly diagnosed on MRI, mesial temporal sclerosis is hardly proof that seizures originate from within the ipsilateral temporal lobe. Consider the following example:
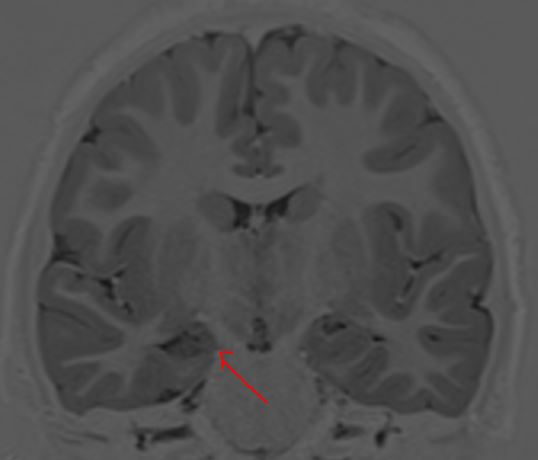
In the coronal T1 weighted image above, the body of the right hippocampus is atrophic, with reduced signal within the same hippocampus, predicting neuronal loss and spongiosis. in this example, the hippocampal atrophy likely is a consequence of the seizure disorder, rather than the cause. Furthermore, the symptomatology of the seizures is primarily of motor seizures, typically tonic-clonic with some motor asymmetries implicating the right hemisphere. However, it is the absence of a history of temporal lobe seizures that is equally important. Then there is the interictal EEG recording:
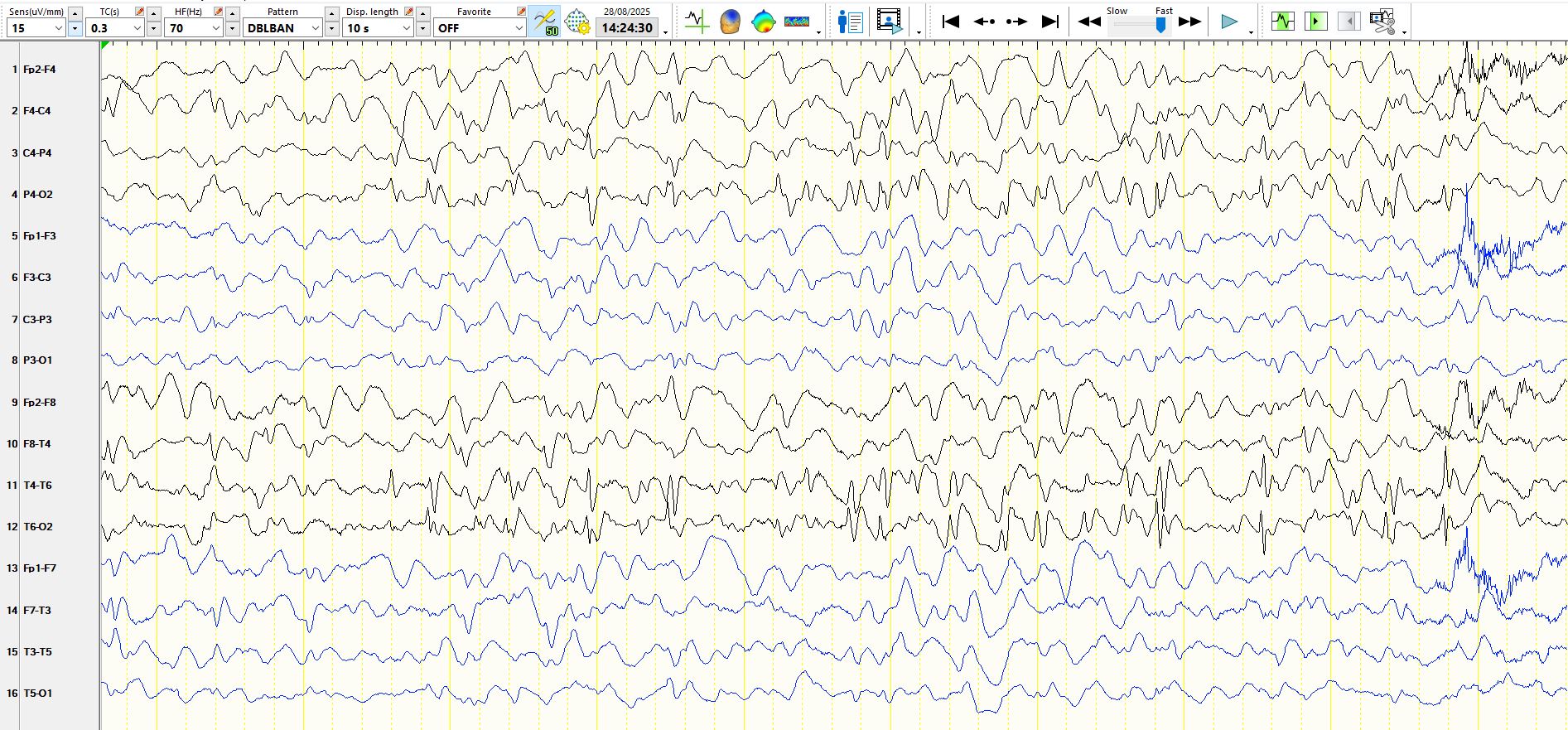
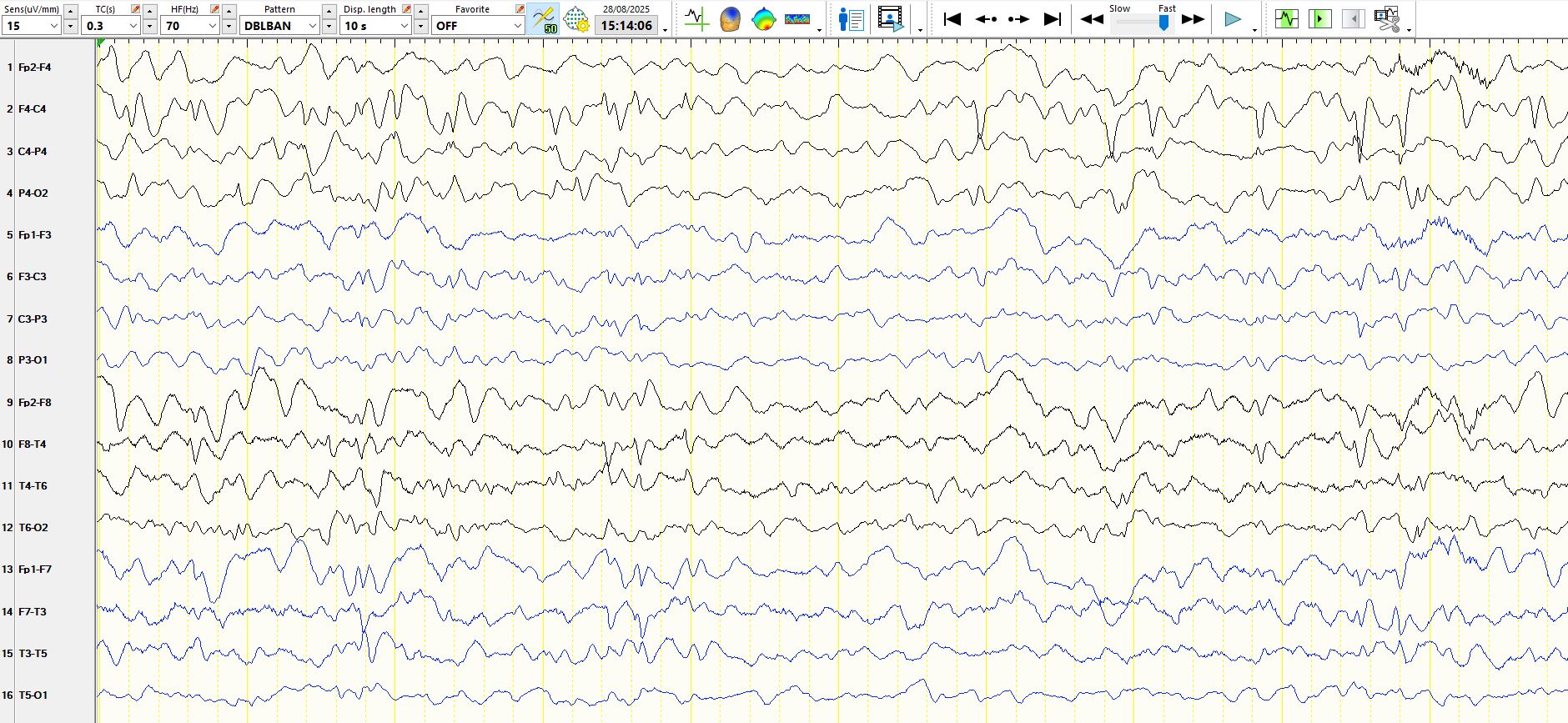
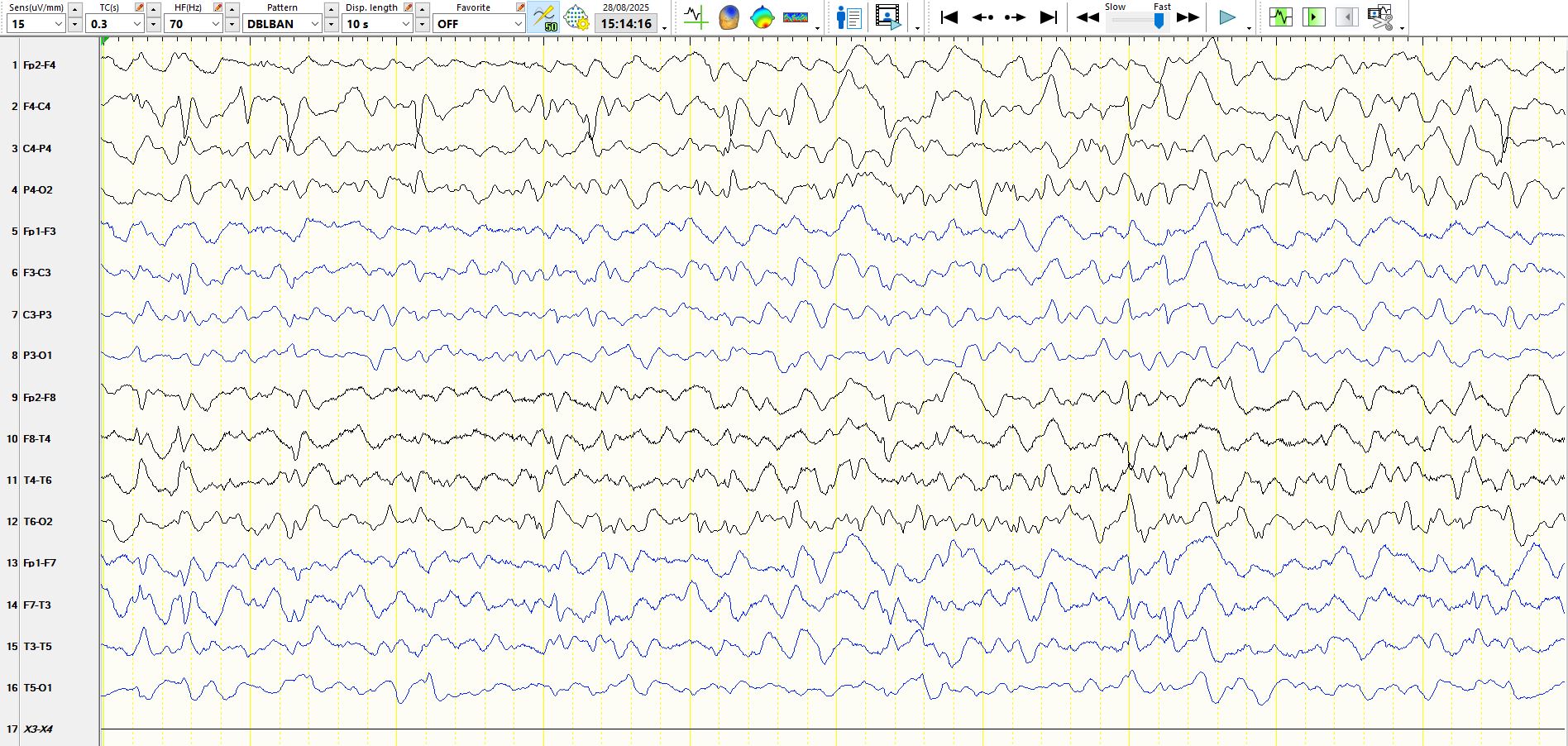
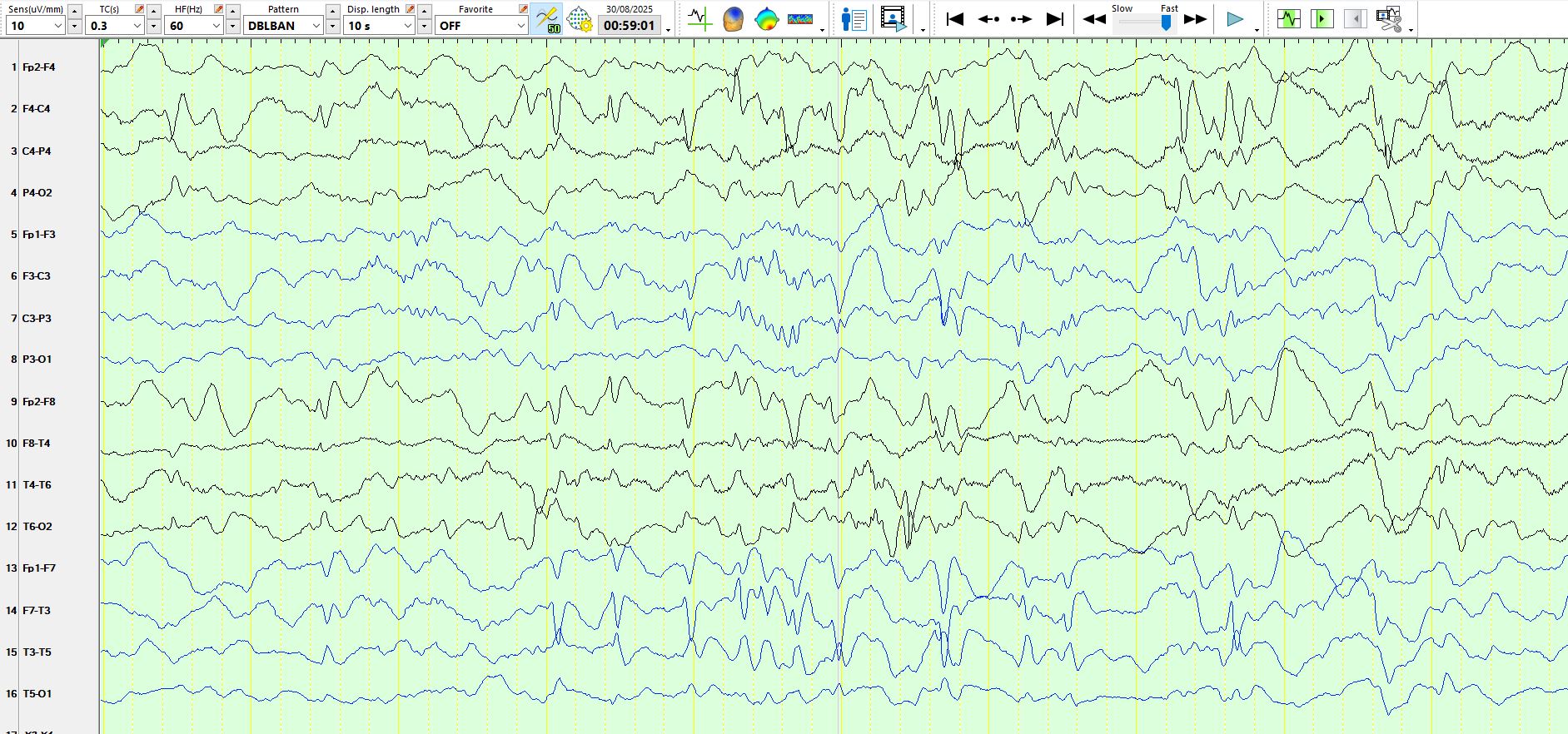
There are multifocal spikes, including over the right and left mid-temporal regions, the right central region, the right posterior temporal and occipital regions, the right prefrontal region and the left central region, with the notable absence of spikes over the right anterior, inferior temporal region. There is also evidence of a generalised encephalopathy, consistent with the history of developmental delay and intellectual impairment. While successful epilepsy surgery may sometimes be possible in people with multifocal inter-ictal epileptiform discharges, in this case it is unlikely that habitual seizures originate in the right medial temporal lobe, even though seizures have not been recorded yet.
PS: the patient has had one seizure over the right occipital region and another over the left posterior temporal region.