
Newly diagnosed focal epilepsy; be prepared for a battle
Sep 08, 2025 
https://jamanetwork-com.ez.sun.ac.za/journals/jamaneurology/article-abstract/2838122
Key Points
Question Can treatment response to antiseizure medication (ASM) in people with newly diagnosed focal epilepsy be quantified and predicted?
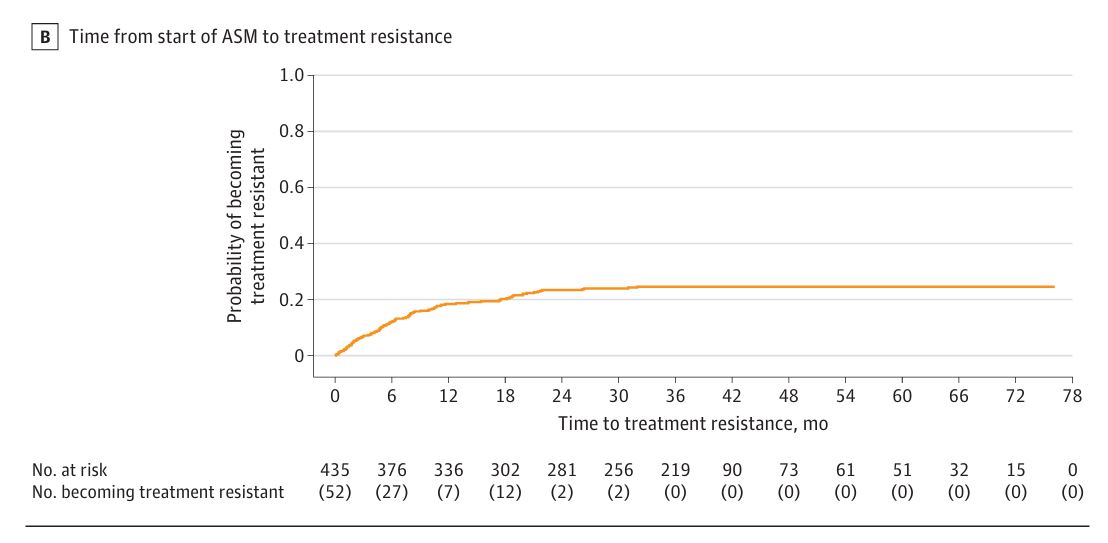
Findings In the Human Epilepsy Project cohort study, most patients with newly diagnosed focal epilepsy took longer than 1 year and more than 1 ASM to become seizure free. Treatment resistance occurred in almost one-quarter of patients and was identified earlier in those with very frequent seizures at baseline, and those with a history of psychiatric disorder(s) had a 1.8-fold increased risk of developing treatment resistance.
Meaning Early identification of ASM failure may reduce time to seizure freedom; pretreatment seizure frequency and psychiatric comorbidities are important prognostic factors.
Importance Epilepsy affects approximately 65 million people worldwide, and 60% have focal seizures. Predicting seizure response and drug resistance to antiseizure medications (ASMs) in people with focal epilepsy remains difficult.
Objective To describe the expected short- and long-term response to treatment with ASMs in people with focal epilepsy using recognized definitions by the International League Against Epilepsy.
Design, Setting, and Participants The Human Epilepsy Project is an international, prospective, observational cohort study that followed up people with newly diagnosed focal epilepsy for up to 6 years between 2012 and 2020. Data were analyzed from 2023 to 2024. The Human Epilepsy Project was conducted at 34 tertiary epilepsy centers across the US, Australia, and Europe. Participants with confirmed diagnosis of focal epilepsy aged 12 to 60 years were enrolled within 4 months of treatment initiation with ASM(s). Data were analyzed from February 2024 to July 2024.
Exposure ASM (variable).
Main Outcomes and Measures The primary outcome was seizure freedom, defined as a period without seizures for 12 months or 3 times the longest pretreatment seizure-free interval, whichever was longer. Treatment response was categorized as sensitive, meaning seizure free receiving 2 or fewer adequate ASM trials; resistant, meaning having 2 or more adequate ASM trials fail; or indeterminate (neither treatment sensitive nor resistant).
Results Among 448 enrolled participants, 267 (59.6%) were female, and median (IQR) participant age was 32 (21-44) years at treatment initiation. Median (IQR) follow-up duration was 3.13 (2.33-3.55) years. Most achieved seizure freedom (267 participants of 448 [59.6%]), largely without relapse (223 [83.5%]). There were 245 treatment-sensitive participants (54.7%), 102 treatment-resistant participants (22.8%), and 101 indeterminate participants (22.5%). Among treatment-sensitive participants, most (217 [89.3%]) responded to monotherapy and half (121 [49.4%], or 27% of total cohort) became seizure free while receiving their first ASM. In the first year of treatment, 251 participants (63%) had ongoing or worsening seizures. Median time to first seizure freedom was 12.1 months (95% CI, 9.7-16.1). This occurred earlier in those who never relapsed (median, 2.2 months; 95% CI, 0.8-3.2) than those who did (median, 7.4 months; 95% CI, 4.0-10.7). Those with infrequent pretreatment seizures were 0.41-fold more likely to be treatment resistant than those with very frequent seizures (relative risk [RR], 0.41; 95% CI, 0.18-0.89; P = .03; HB-corrected P = .02). Participants with self-reported comorbid psychological disorders were 1.78-fold more likely to be treatment resistant than those without (RR, 1.78; 95% CI, 1.26-2.52; P = .001).
Conclusions and Relevance In the Human Epilepsy Project multicenter prospective cohort study, most people with newly diagnosed focal epilepsy took more than a year and more than 1 ASM to become seizure free. Drug resistance can be identified earlier in those with frequent pretreatment seizures, and a history of psychiatric comorbidities at epilepsy diagnosis is an important prognostic factor.
PS: many institutions schedule patients for follow-up with 3-6 monthly visits. If you are having frequent seizures, this is a long time to wait to see the neurologist. These long waits for seizure control may be substantially reduced if patients have a hotline to inform the neurologist that seizures have not abated. Don't forget that steady state with most of the antiseizure medications takes no more than a few days.
Here is a question for you; 40% of patients had an epileptiform abnormality on the EEG and only 17% had a relevant MRI lesion. What percentage of patients in this study have functional seizures and what percentage of patients have been misclassified as having focal epilepsy, when they have generalised epilepsy? The truth is that we will never know! I pose this question deliberately so that you might start thinking about these possibilities when you first diagnose people with focal epilepsy.