
Epilepsy, last seizure more than 48 hours ago
Sep 05, 2025This is the EEG of a 60-year-old patient:
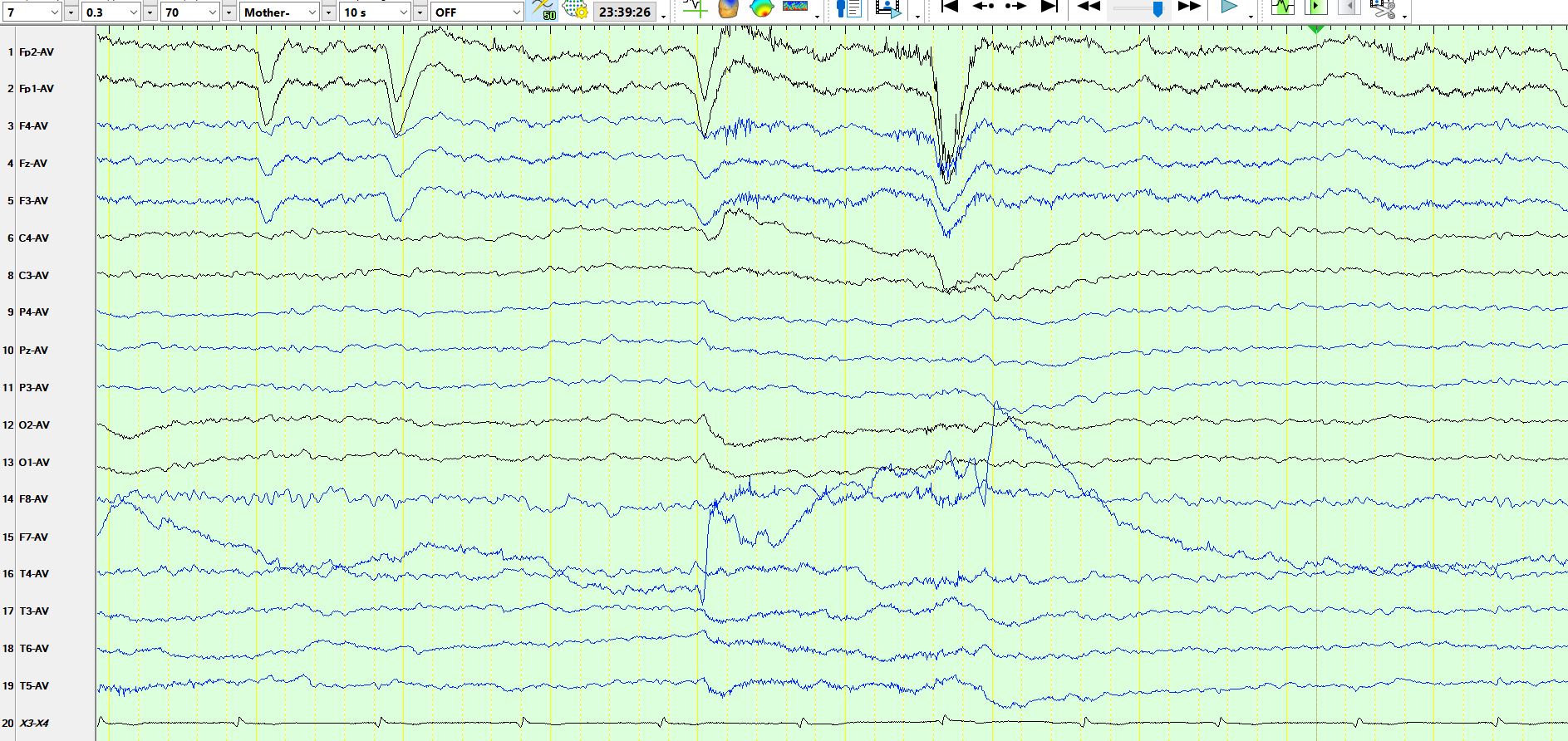
Figure 2:
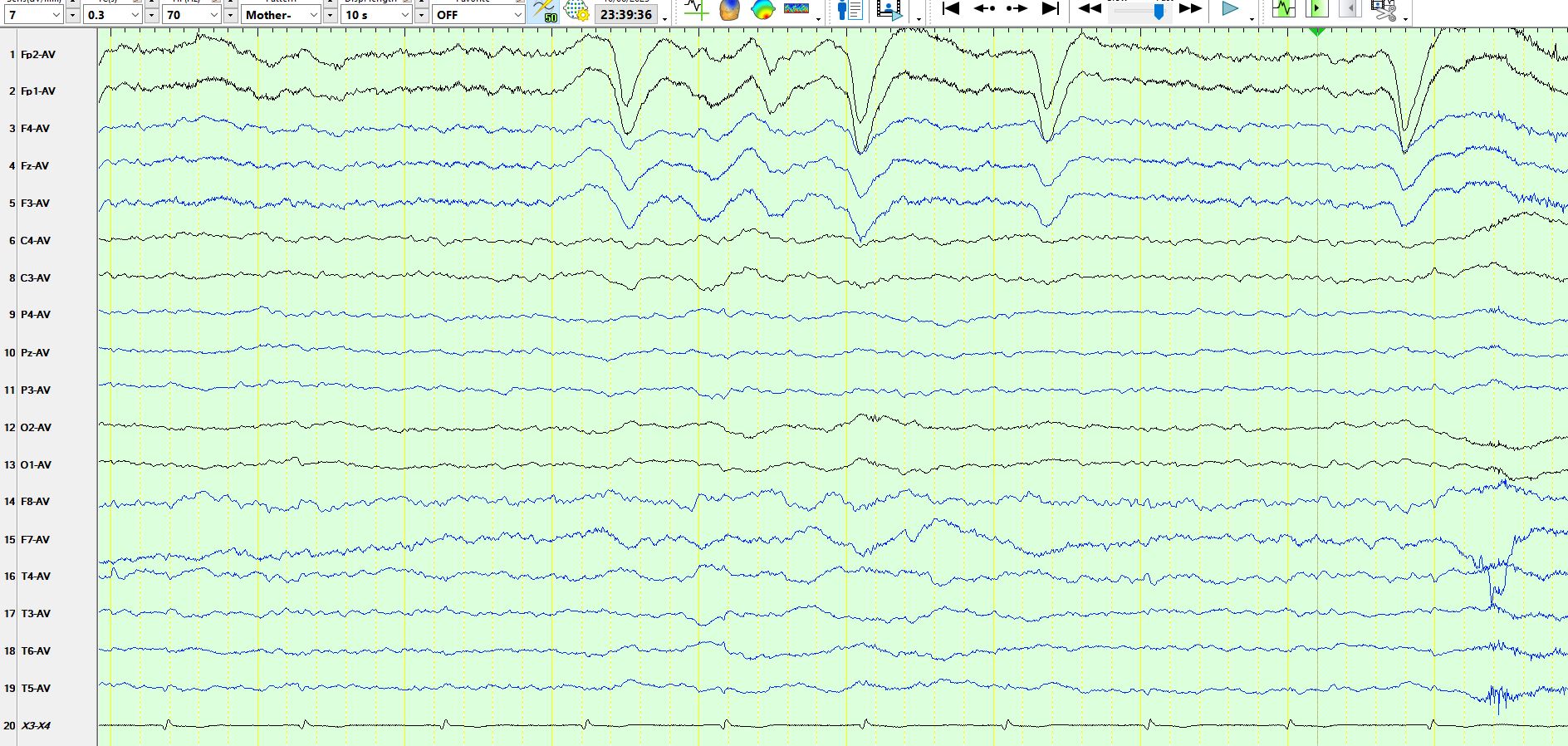
Figure 3, the AP bipolar montage of the same page:
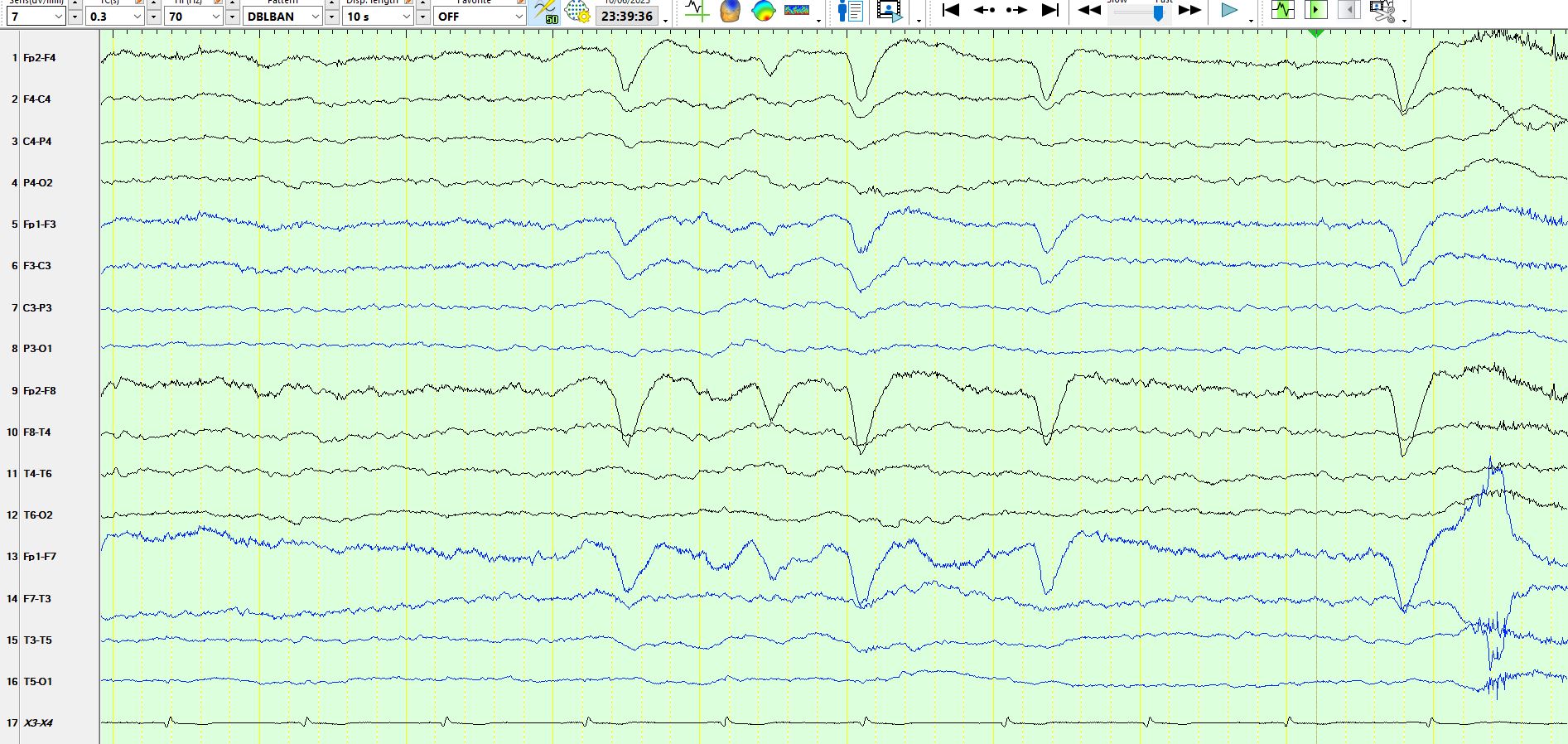
Figure 4, the coronal montage of the same page:
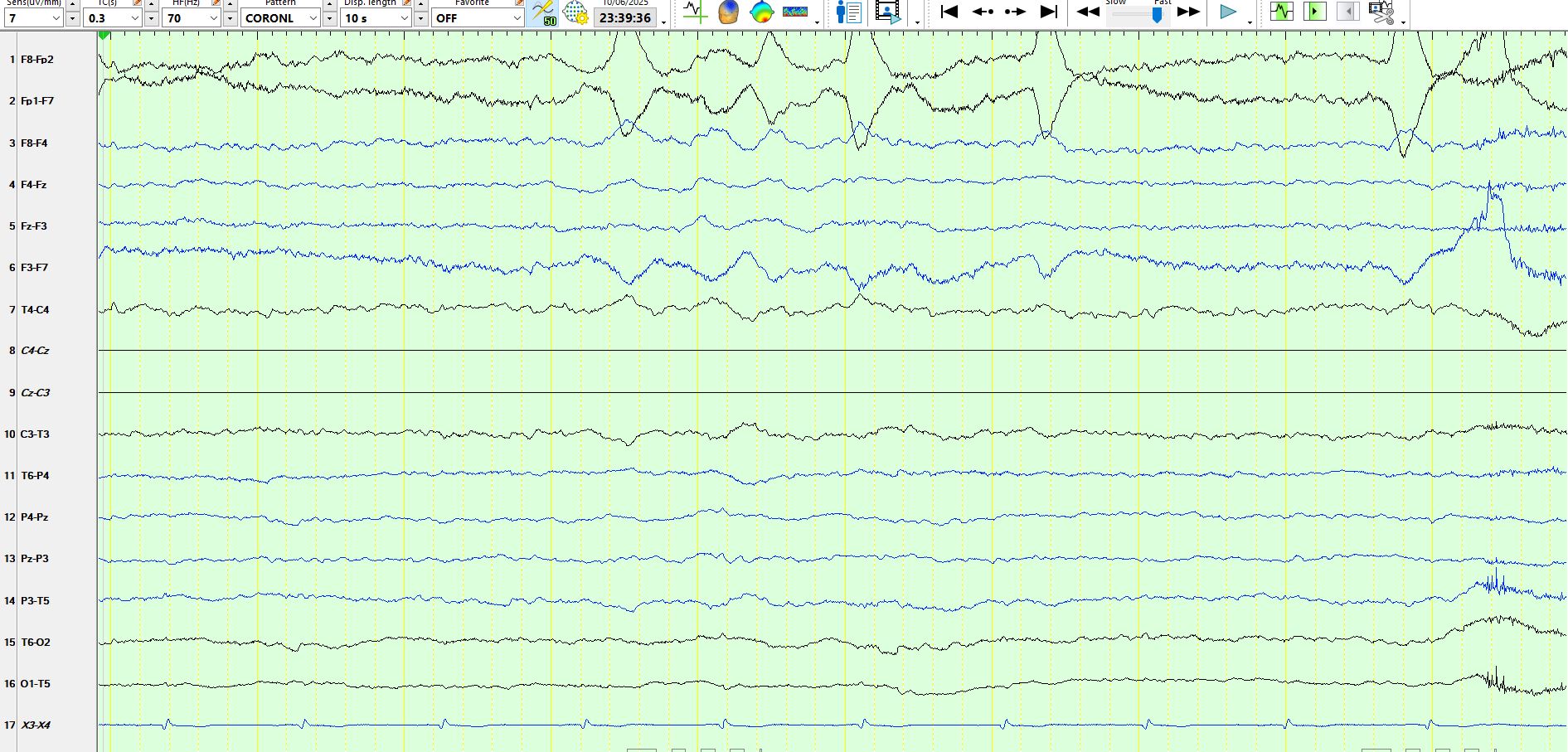
Figure 5:
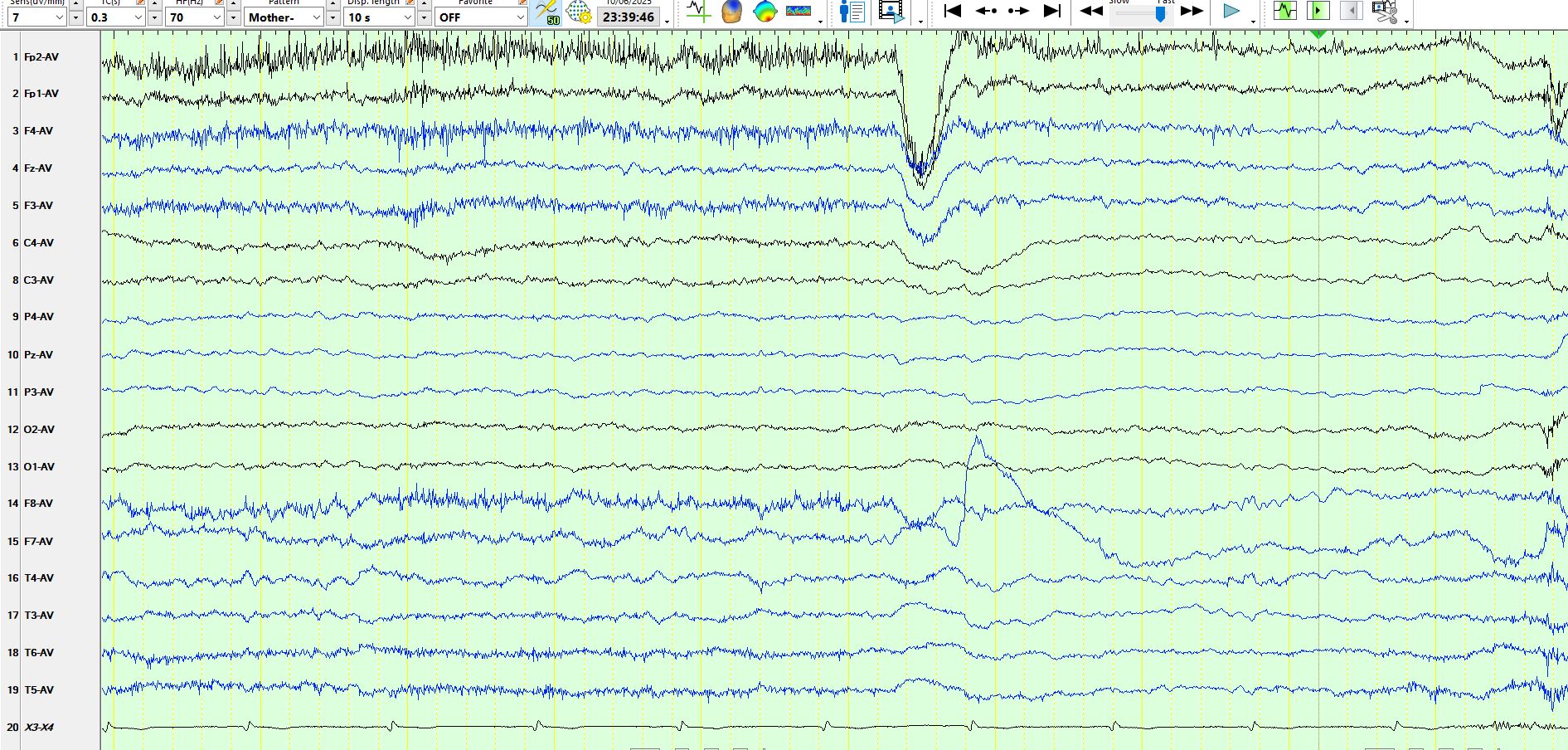
Figure 6:
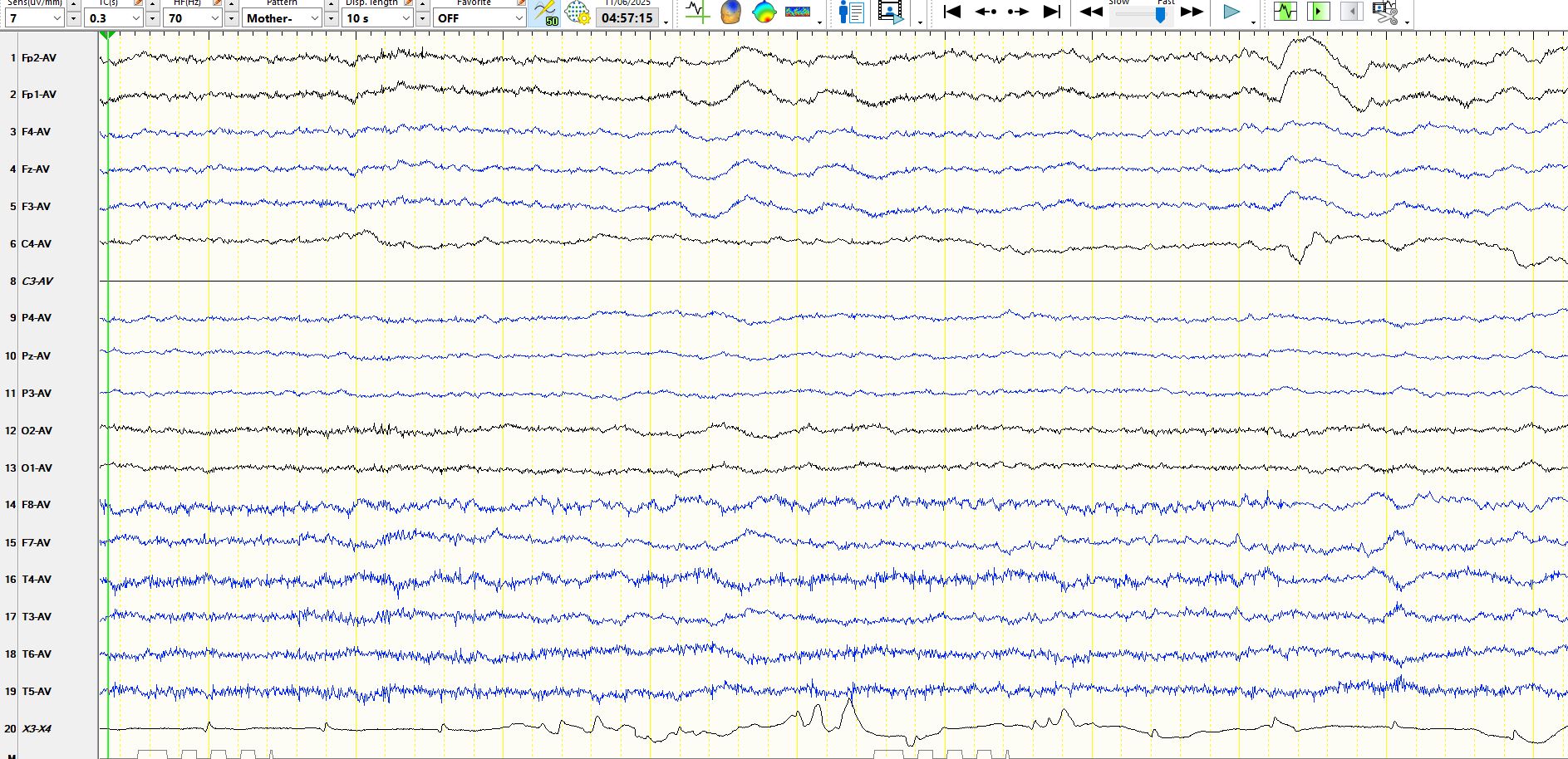
Figure 1 demonstrates theta over the frontal regions between the second and fourth second of the page. One has to be careful of frontal theta, as it may be related to mild drowsiness. However, after the last eyeblink there are definite delta waves over the frontal regions; these are abnormal.
Figure 2 demonstrates a train of frontal rhythmic delta waves, as appeared relatively infrequently in this patient 48-72 hours after he had three tonic-clonic seizures. No other cause was apparent and therefore the FIRDA is judged to be frontal intermittent rhythmic delta waves. While these typically disappear within minutes or occasionally hours after a tonic-clonic seizure, in the minority of patients they may resolve over a period of a few days, especially when there has been a cluster of tonic-clonic seizures. This mirrors the duration of post-ictal cognitive dysfunction, which may persist for days and occasionally up to 4 weeks after a seizure or cluster of seizures. The postictal state is all too easily dismissed because of the subjective nature of the symptoms, such as concentration difficulties and fatigue. In fact, some patients may have cognitive dysfunction or fatigue four days after a focal aware seizure. One has to remind patients not to make major decisions during the period of cognitive dysfunction, no matter how mild, and likewise scholars and students should not disadvantage themselves by writing examinations during this period. It is worth saying that executive functioning may not be apparent to the individual and fatigue or mild cognitive fogginess may be the only clues to its presence. I recently advised a business owner, who was in the process of negotiating to buy another business, to put this on hold for a week following a tonic-clonic seizure, as this was in the best interests of the patient/business owner, who was feeling very tired on a Monday following a tonic-clonic seizure on the Sunday.
Figures 3 and 4 demonstrate the frontal intermittent rhythmic delta activity on the bipolar AP and coronal montages.
Figure 6 is yet another illustration of the appearance of the frontal intermittent rhythmic delta activity. While frontal intermittent rhythmic delta activity is often much higher in amplitude and more distinct, the above appearance is typical of the evolution of FIRDA. In this instance he presented 48 hours after his last seizure.
When you see frontal intermittent rhythmic delta activity, be on the lookout for other abnormalities, especially focal ones. In this instance the patient had intermittent arhythmic delta waves over both temporal regions, likely related to the focal nature of some of the dysfunction in the postictal state and reflecting a focal origin for the seizures. The patient had a good outcome following a right temporal lobectomy some 18 years ago but has retained a propensity to occasional tonic-clonic seizures in sleep. On this occasion he/she developed diarrhoea.