
Adult, epilepsy versus functional/dissociative seizures
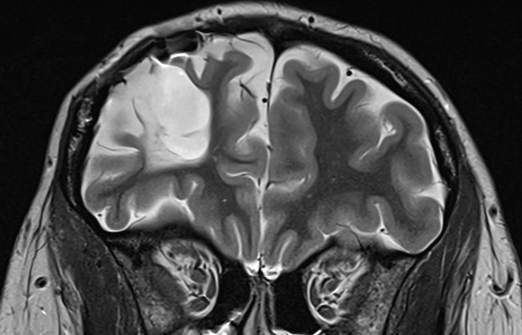
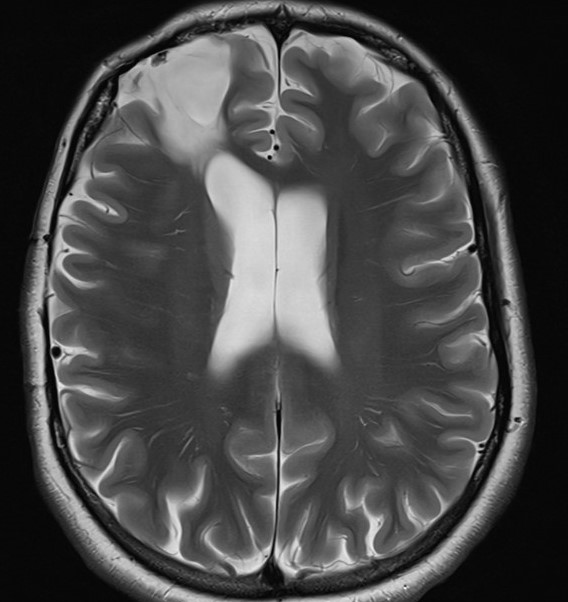
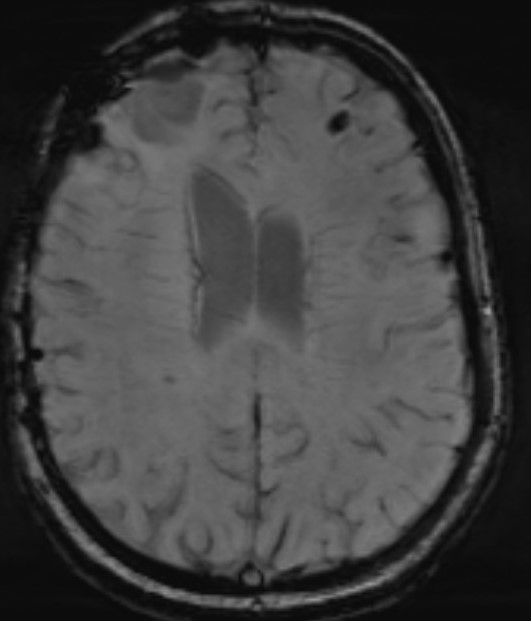
Feb 24, 2026Intellectually normal, traumatic brain injury at the age of 4 months, EEG is normal while awake. The MRI scan is reported to show extensive spongiosis and cavitation in the right frontal lobe. A colleague has treated the patient with lamotrigine for epilepsy for the past few years. He requested a review of the diagnosis.
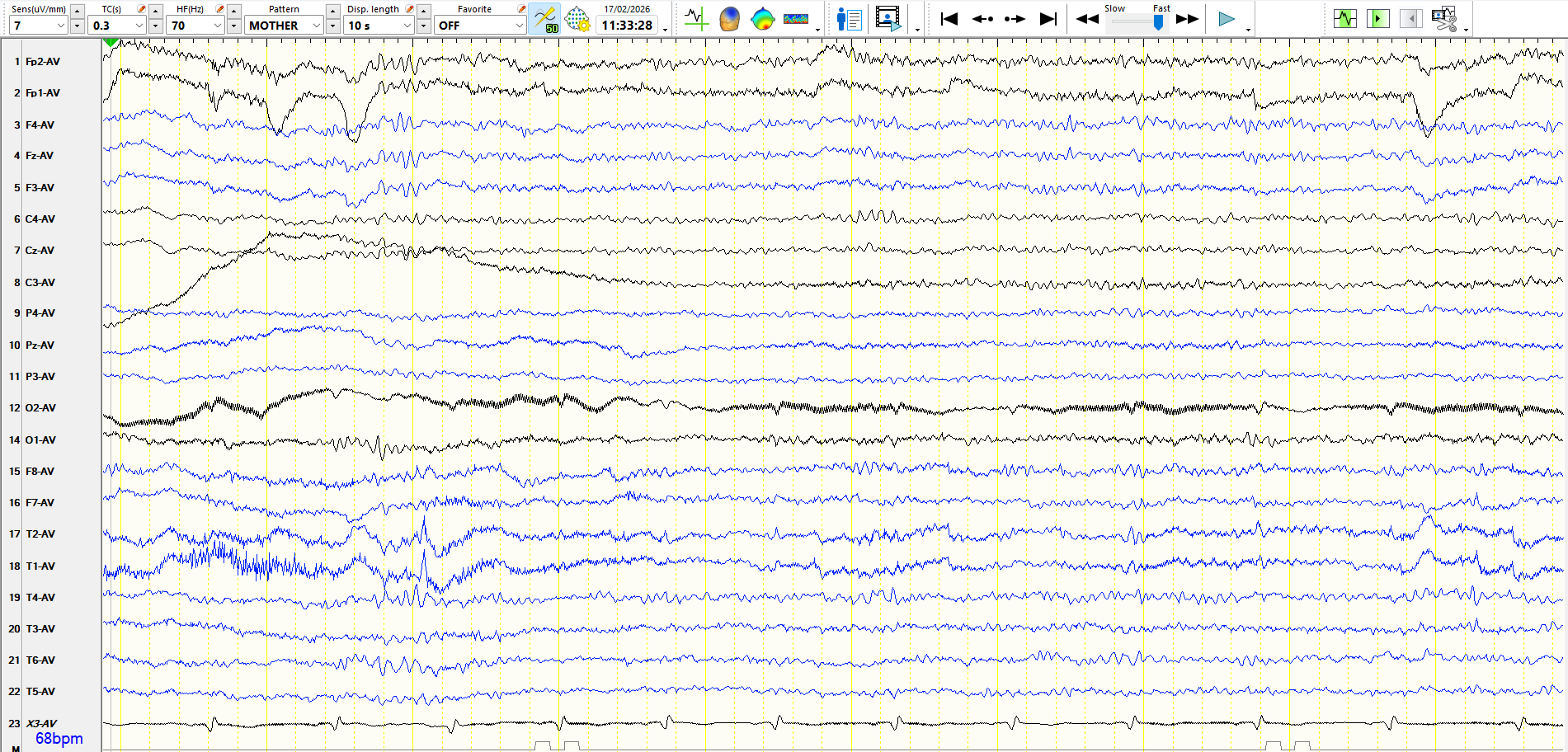
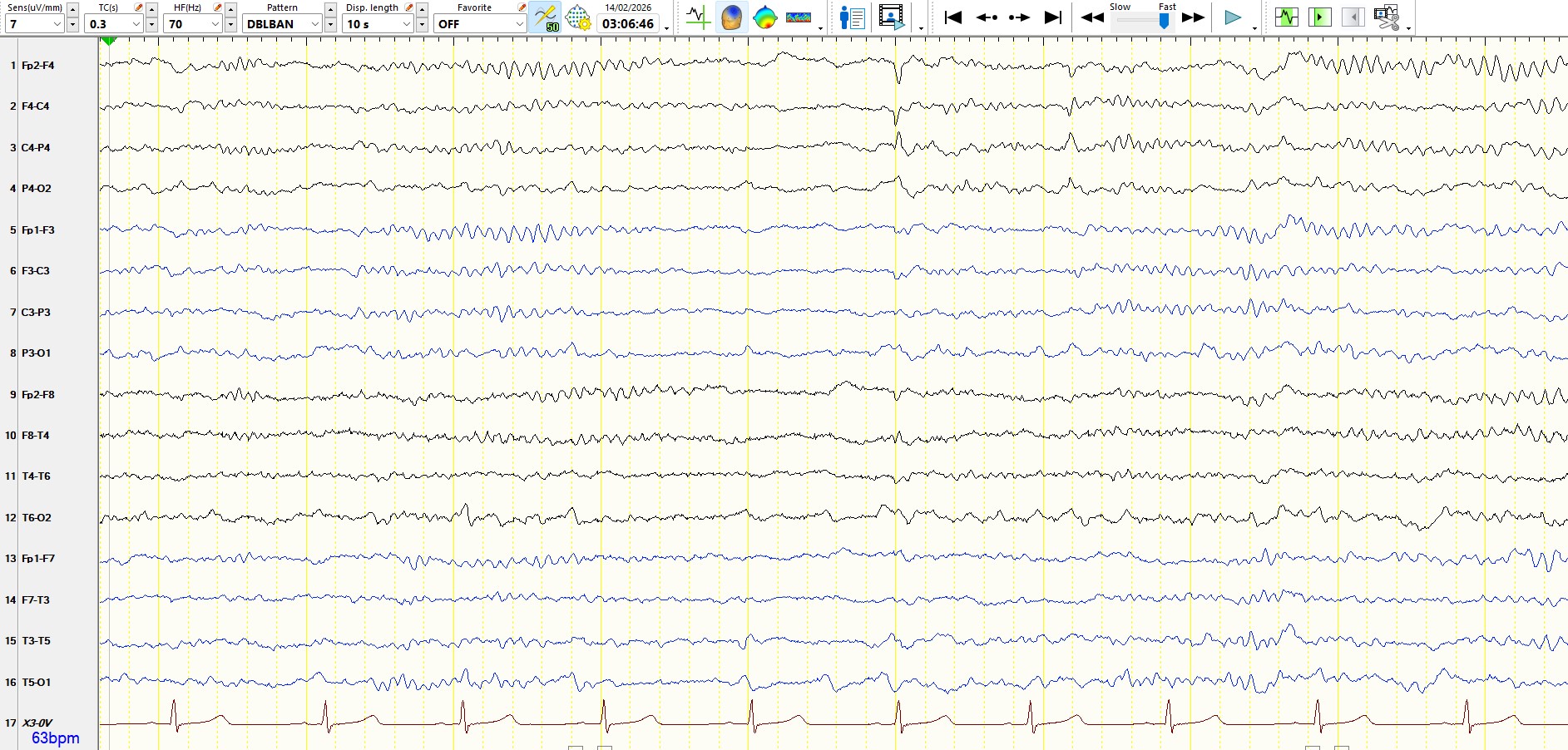
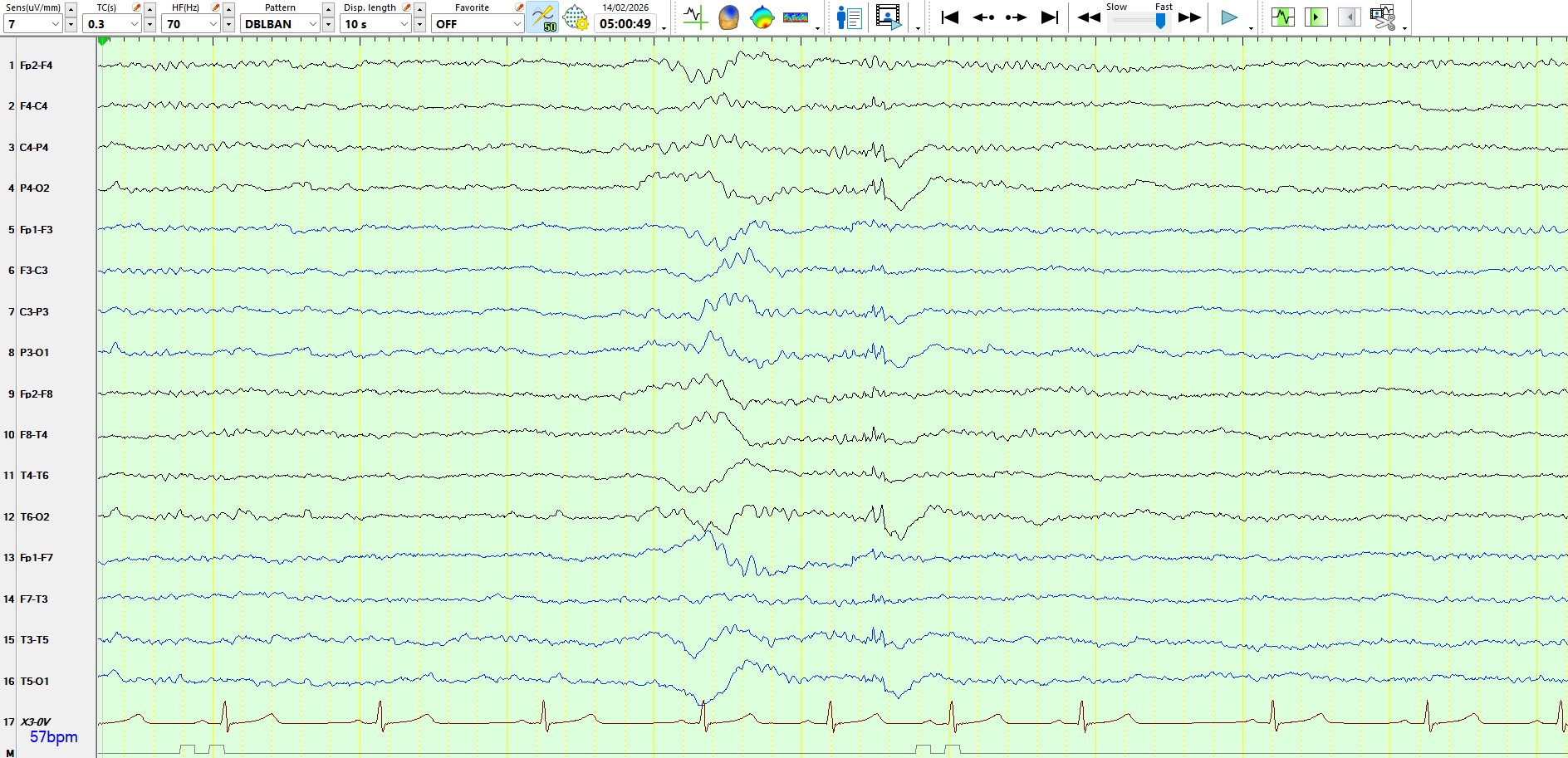
Awake:
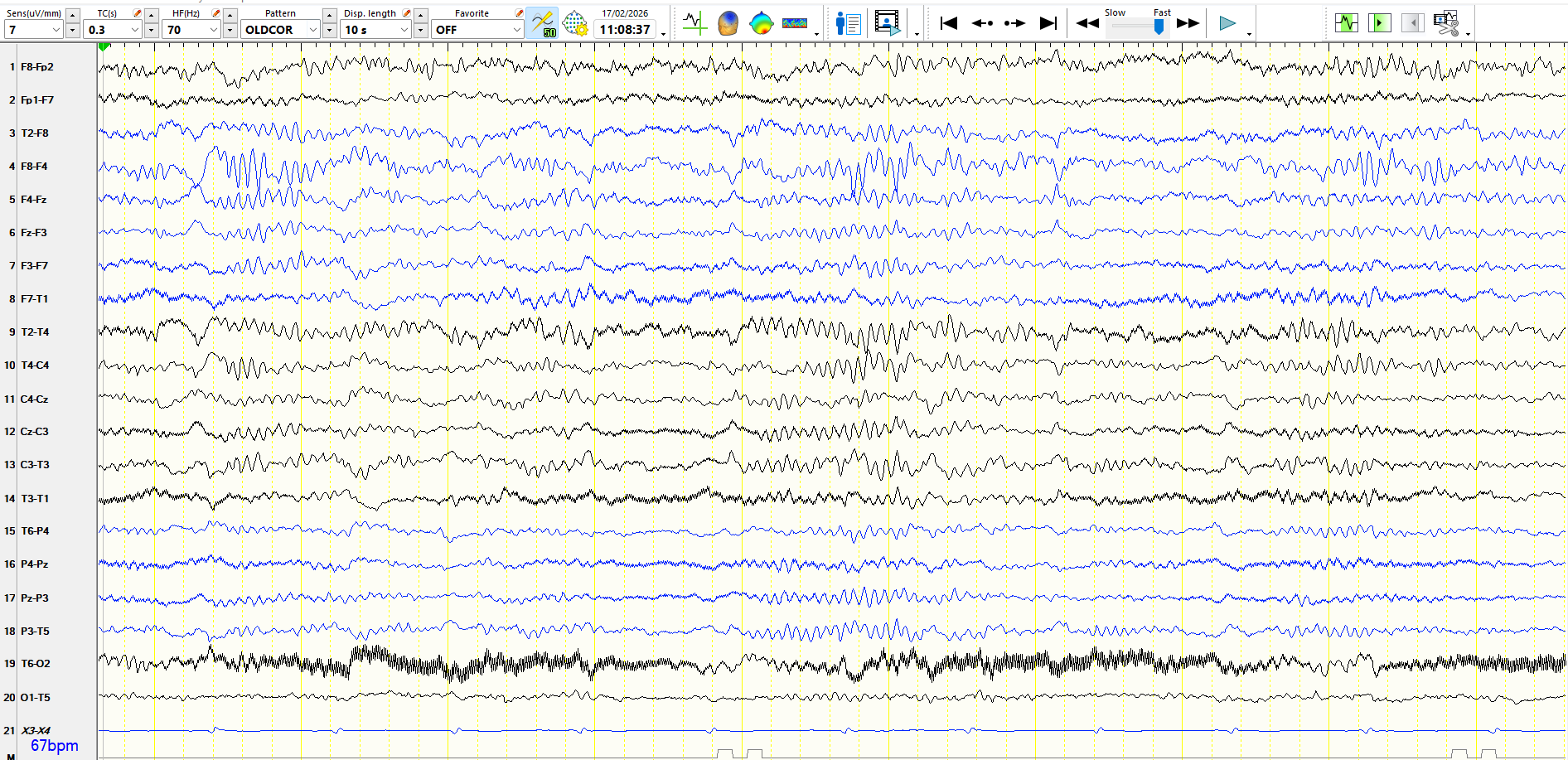
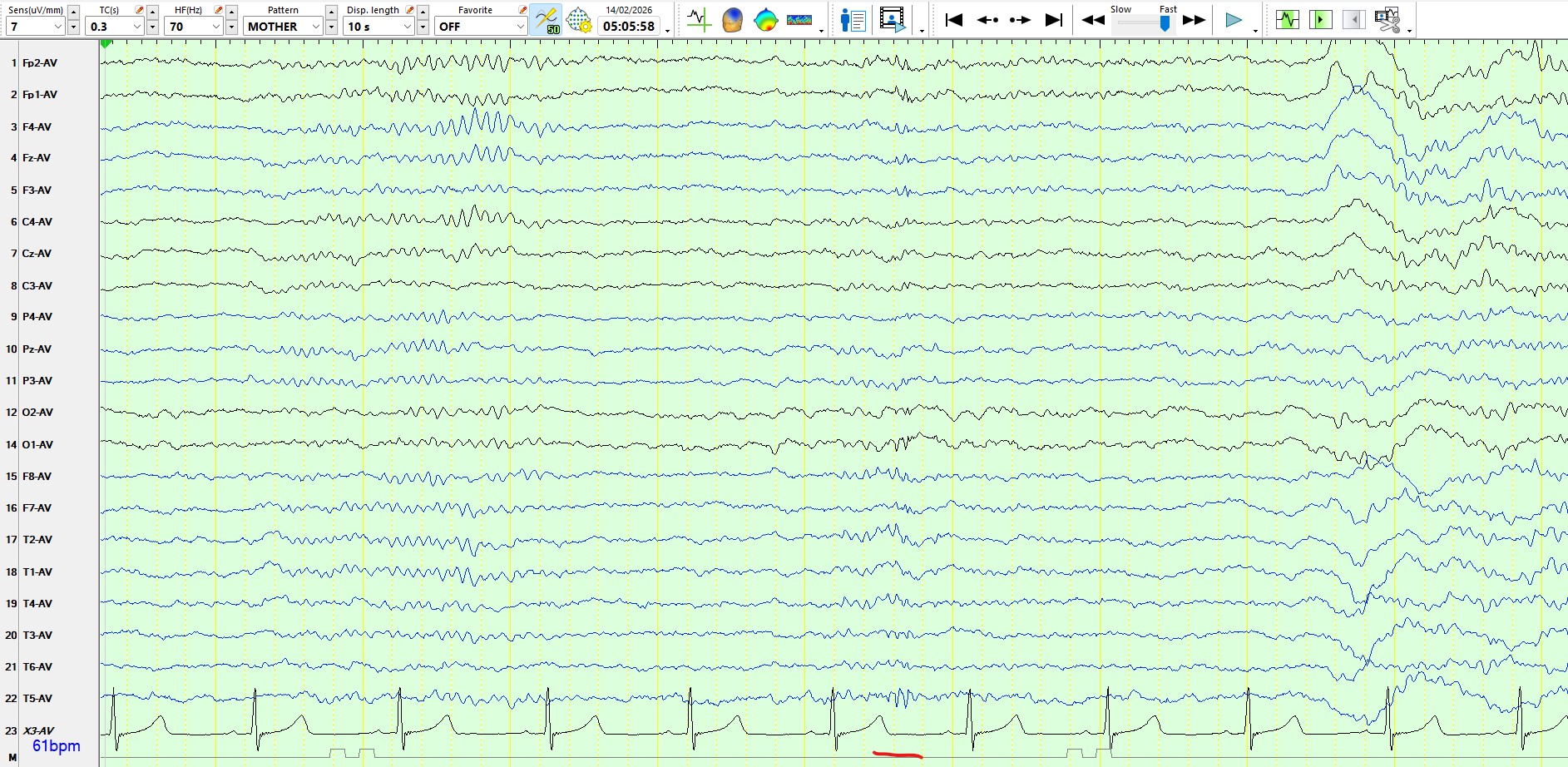
Drowsy:
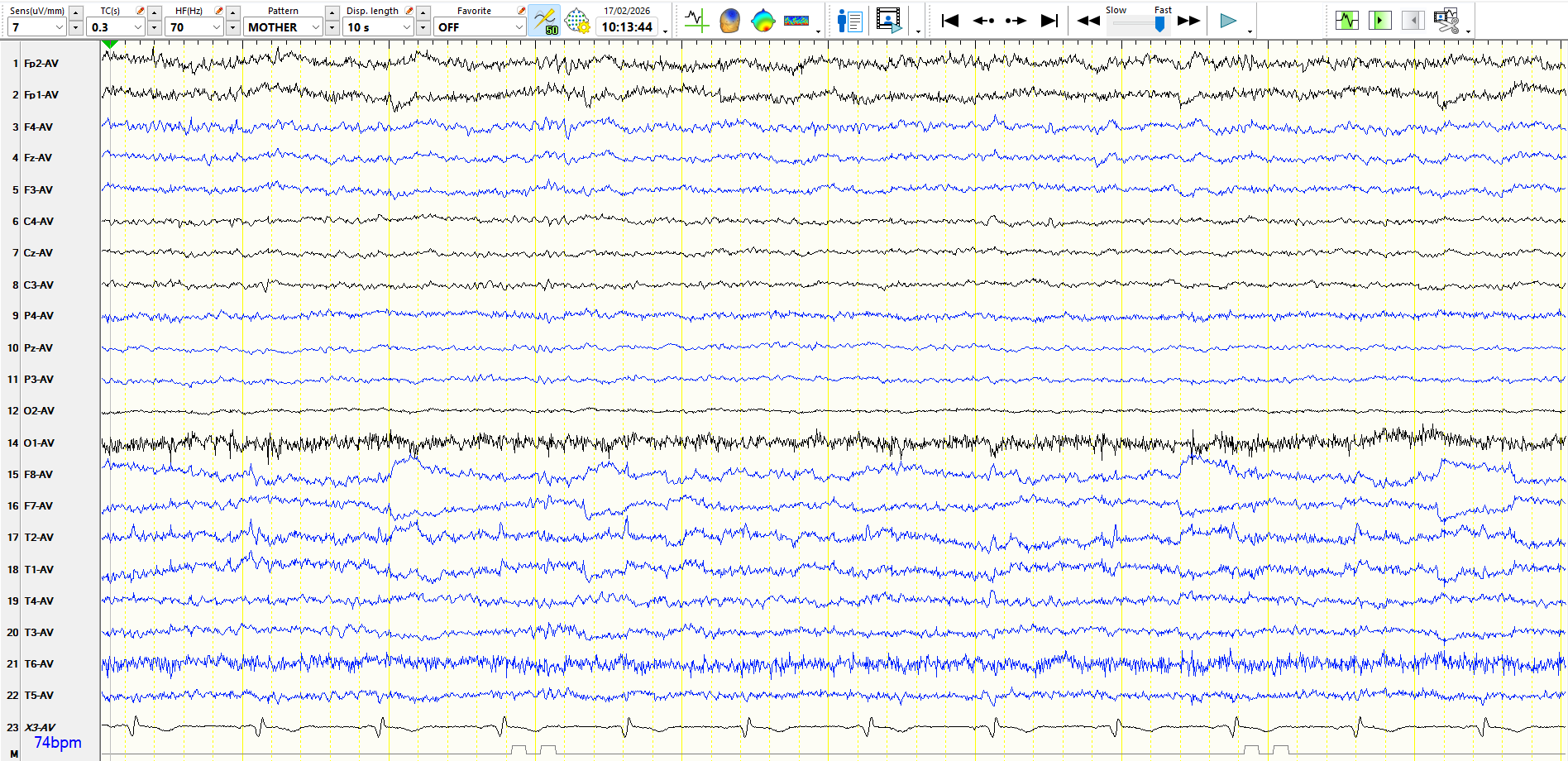
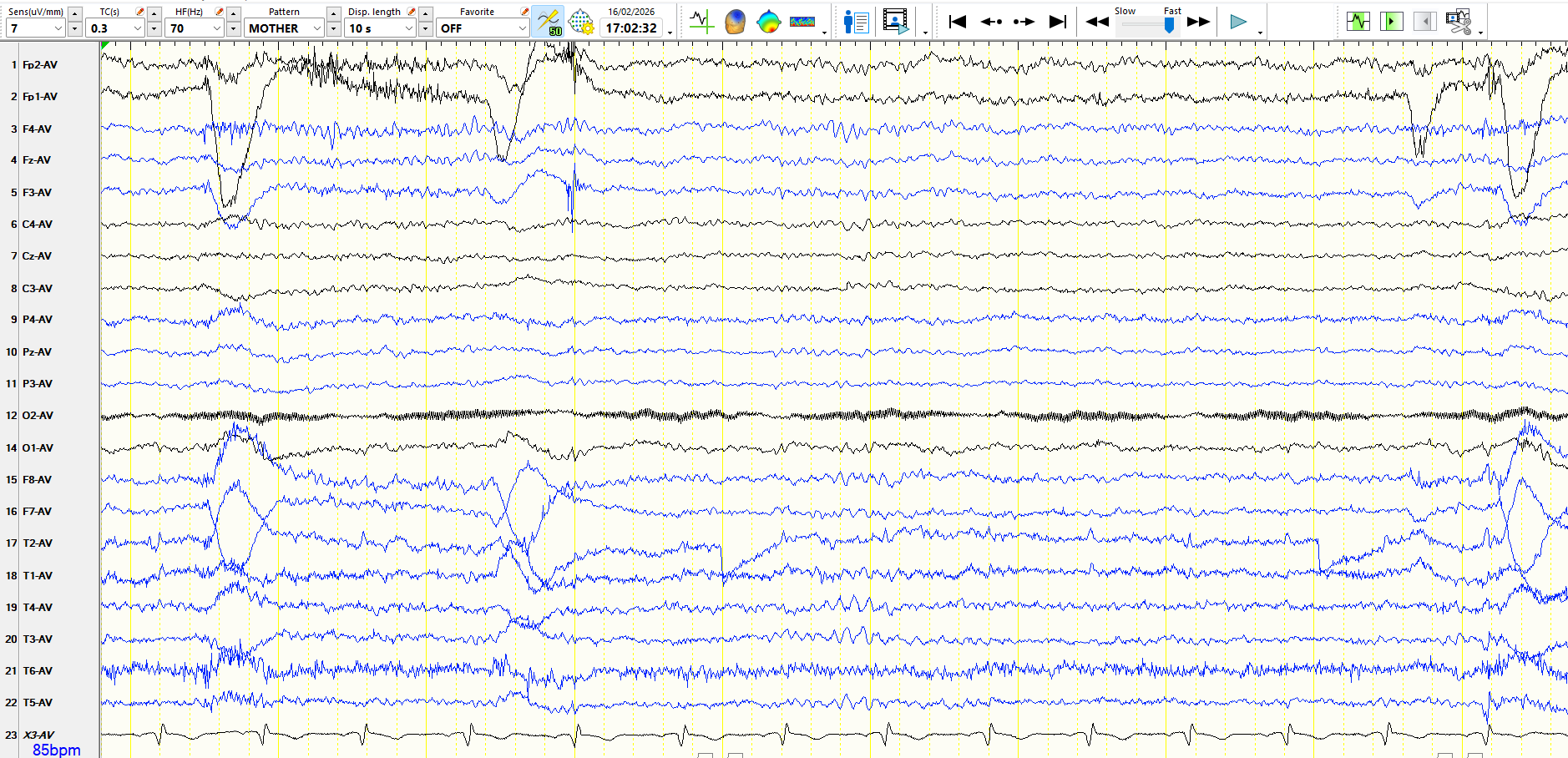
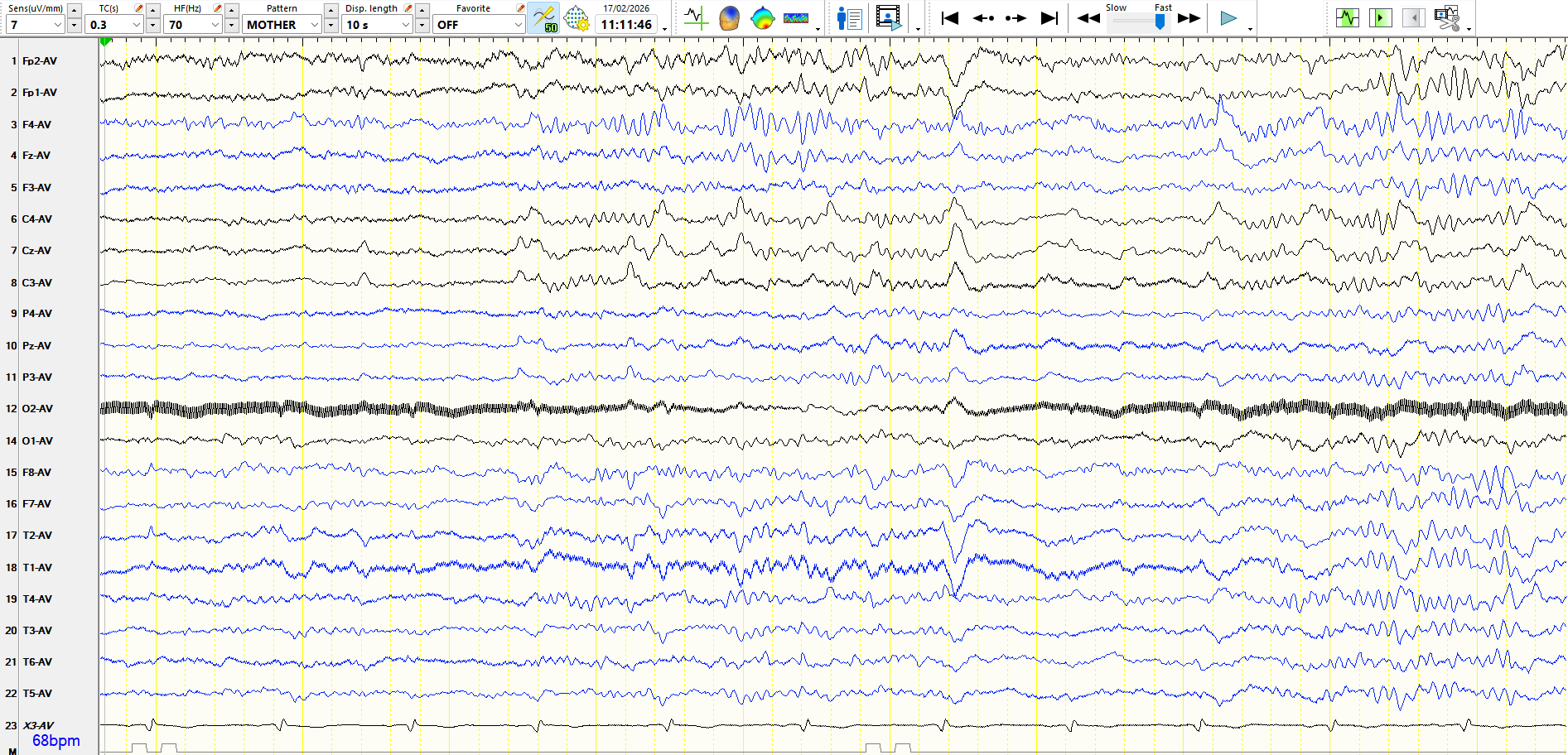
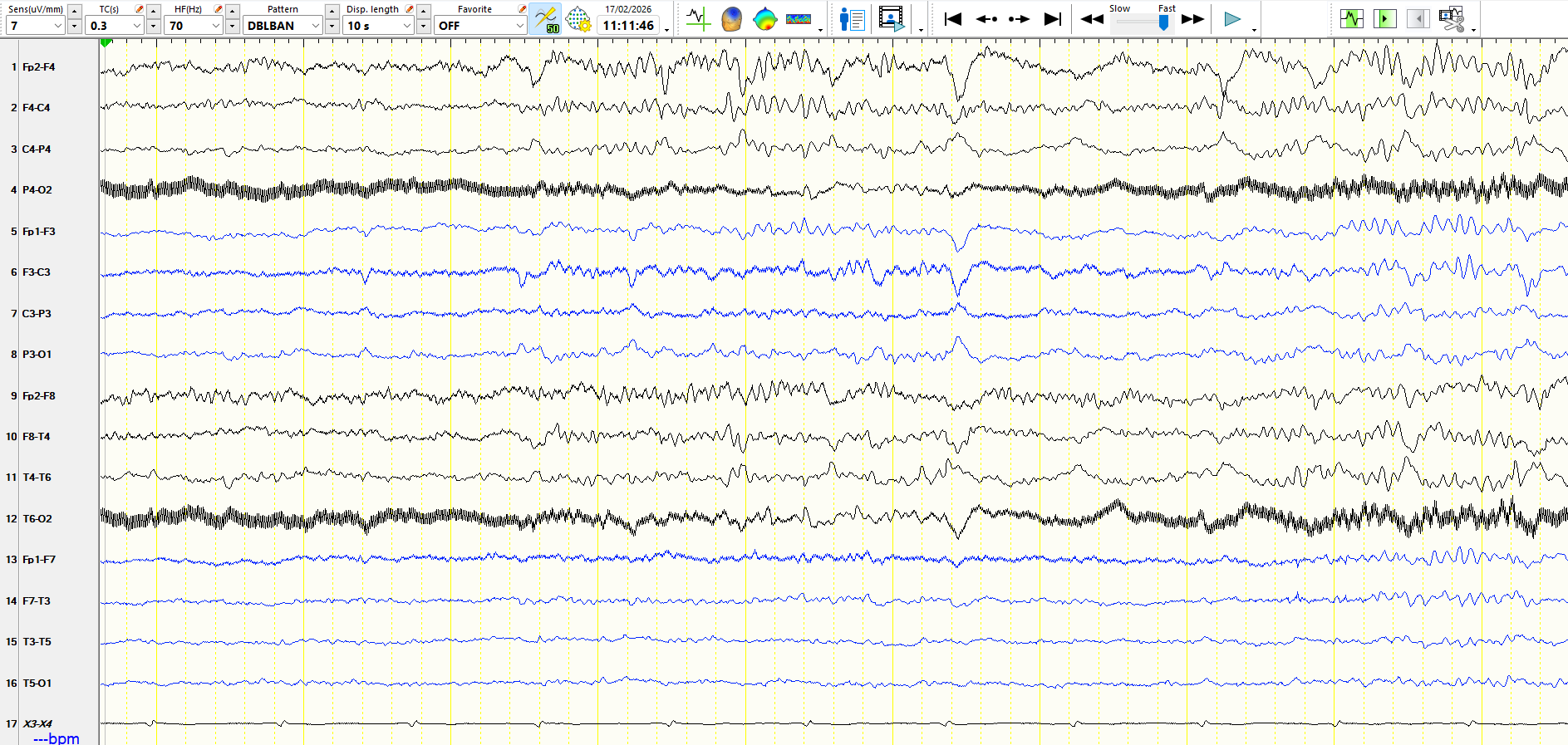
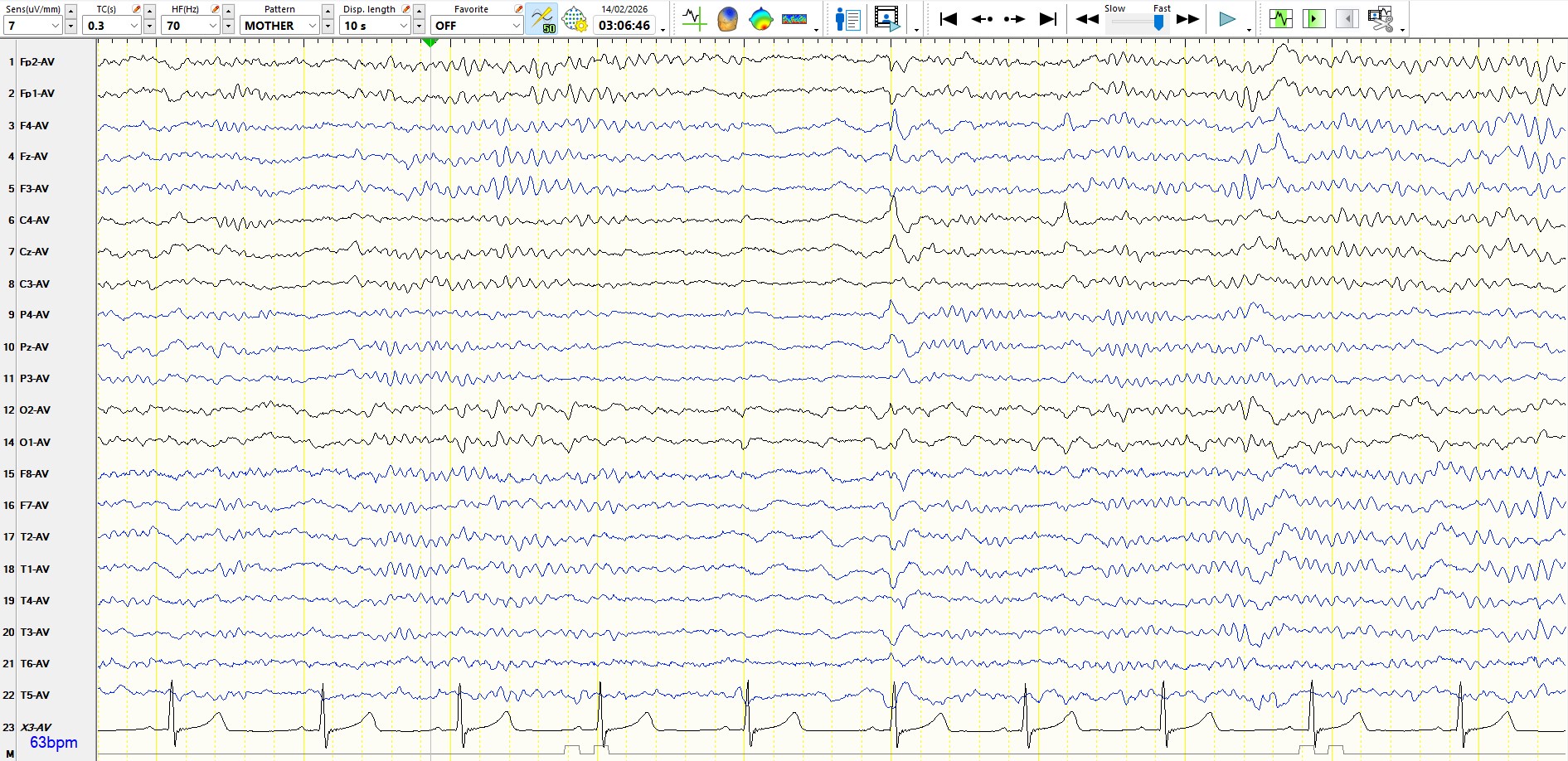
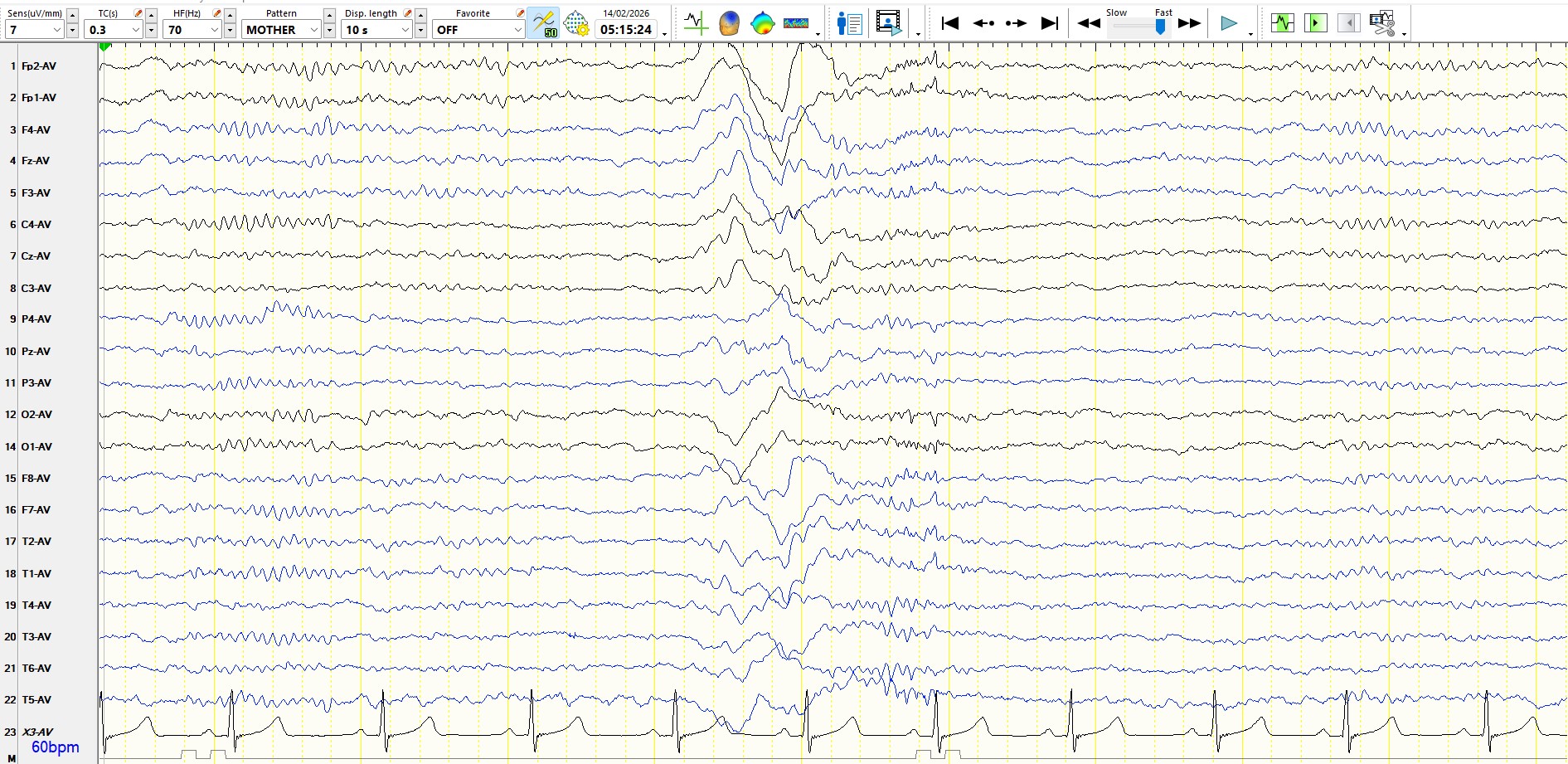
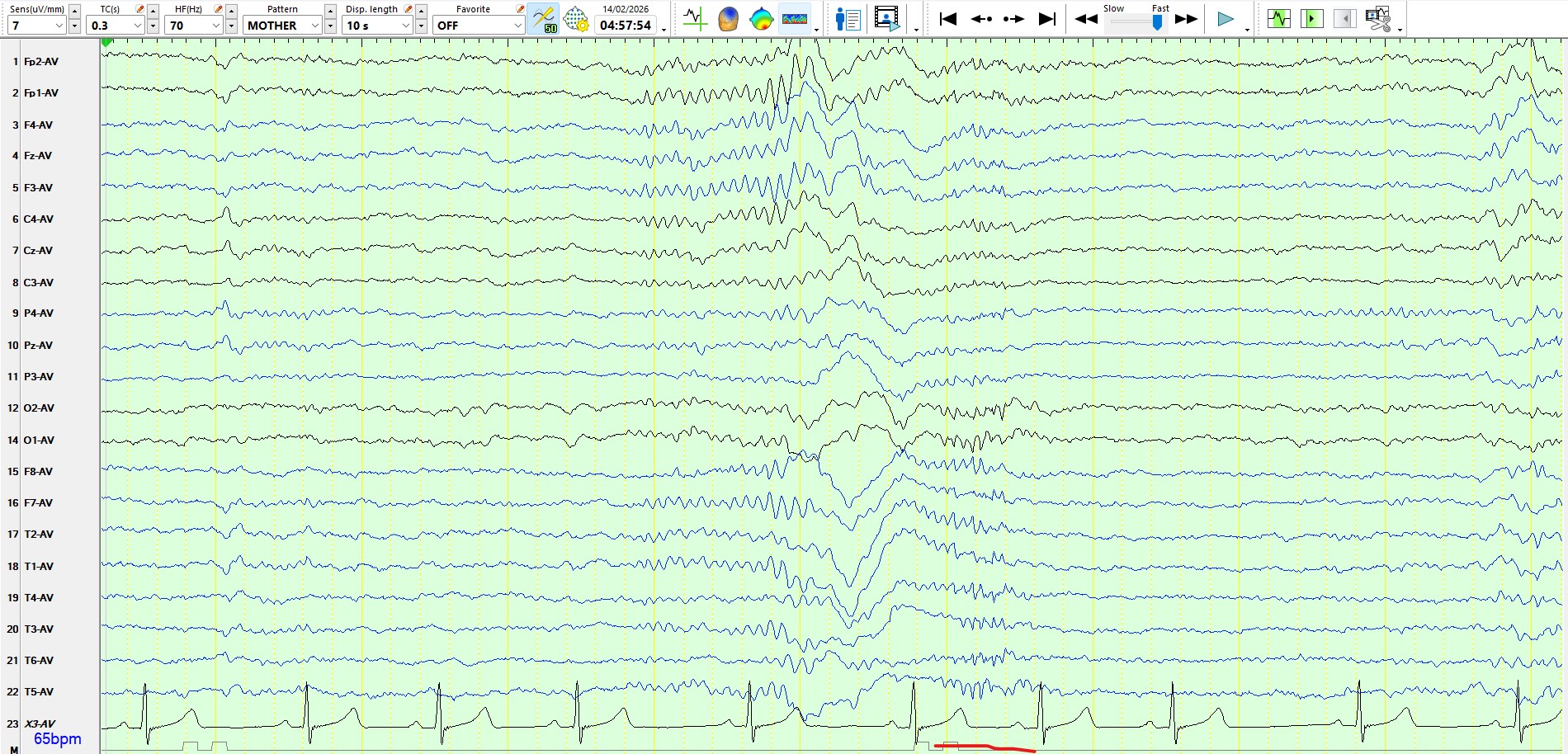
The following is representative of stage II sleep, with many similar waveforms
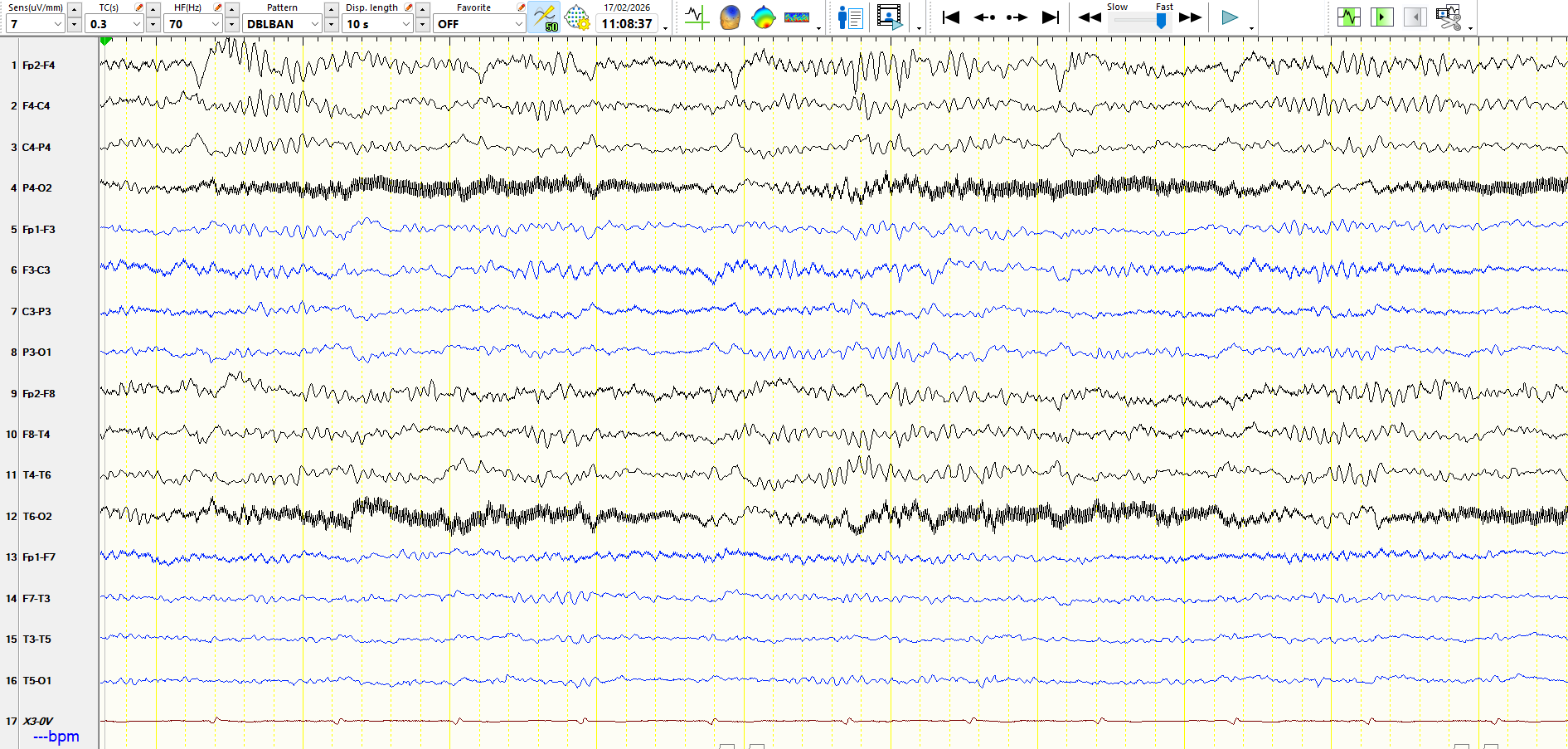
A few observations:
1. Notice the asymmetry of beta frequencies, higher in amplitude at F4 than at F3. This likely relates to the drainage of a haematoma at the age of 4, with a consequent breach rhythm. Notice also the asymmetry of the amplitude of the sleep spindles.
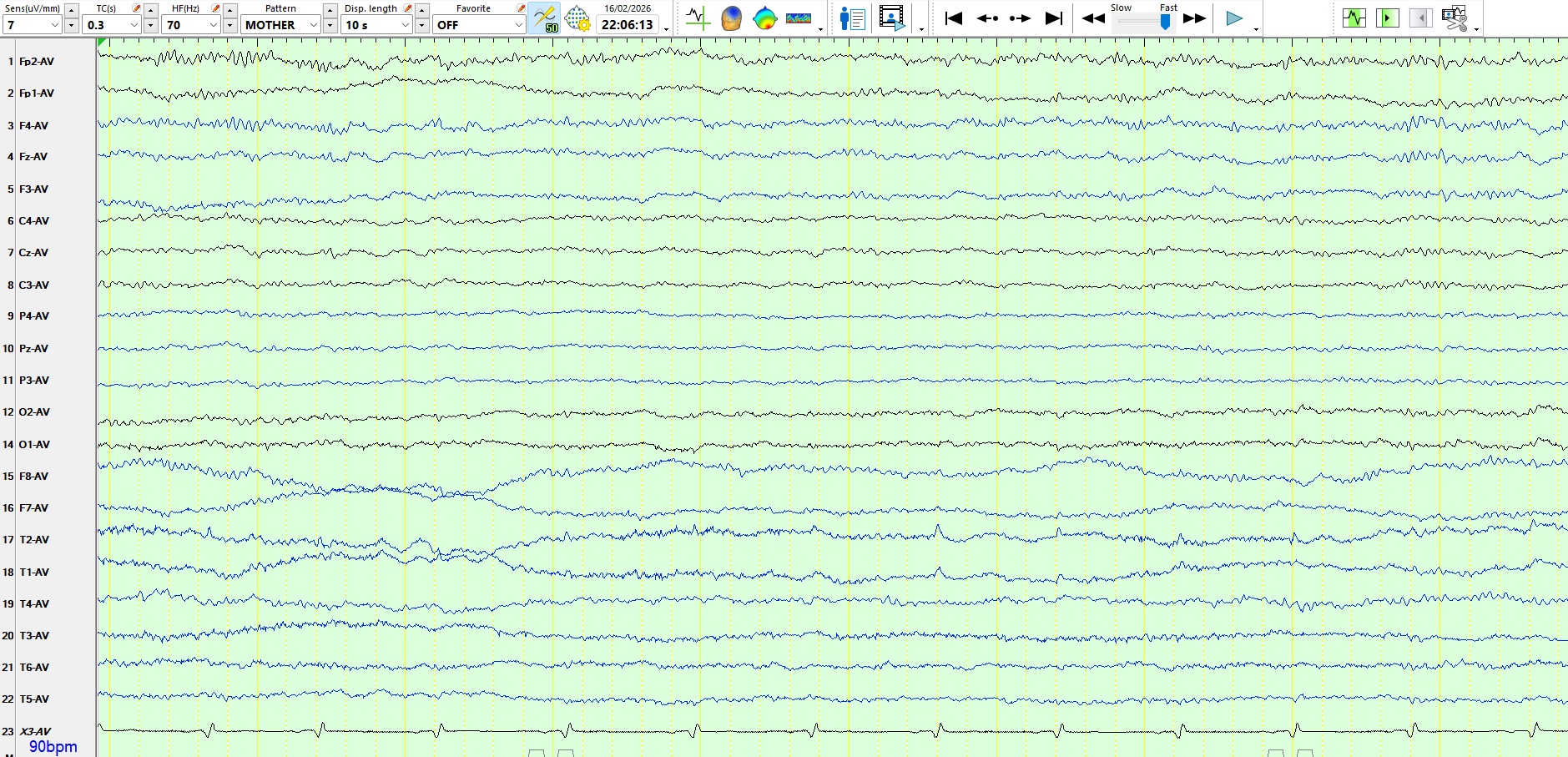
2. This is relevant, given the sharply contoured waves over the right frontal-central region. These have the morphology of vertex waves and appear exclusively during sleep. While some of these are symmetric in amplitude, some have a right-sided predominance and, on coronal montages, are primarily electro-negative over the right frontal-central region. Unsurprisingly, there is a vertex wave that is primarily electro-negative over the left front-central region on the 3rd and 4th images from the top. Asymmetries of vertex waves are common. These waves above, therefore, likely represent asymmetric vertex waves, rather than sharp waves; if you are in doubt, a conservative interpretation is once again prudent. Don't be fooled by your biases related to having viewed the MRI scan. Just for good measure, at the foot of this page, I have appended an EEG from a 20-odd-year-old patient with "POTS", who does not have epilepsy. The patient has a normal EEG, including these asymmetric V-waves.
3. The history provided by the patient and her boyfriend suggests that she either has left frontal lobe seizures or non-epileptic seizures or both. The MRI scan demonstrates an additional, potentially highly significant lesion in the left frontal lobe that was not mentioned in the report.
4. The video-EEG recordings were entirely normal over a period of 8 days, with a single recorded functional/dissociative seizure on the penultimate day. This was an atypical seizure for her, and hence, there is still a little uncertainty about the nature of these. She will erect a video camera at home, and her family, boyfriend, and friends will video any seizures that occur.
5. The weight of the evidence indicates that she has functional/dissociative seizures, while there is no proven diagnosis of epilepsy. The probabilities for epileptic seizures have diminished markedly. However, it is worth being vigilant for the possibility, while not continuing indefinitely with antiseizure medications, with their potential harms and unproven benefit for her. All seizures will be judged on merit.
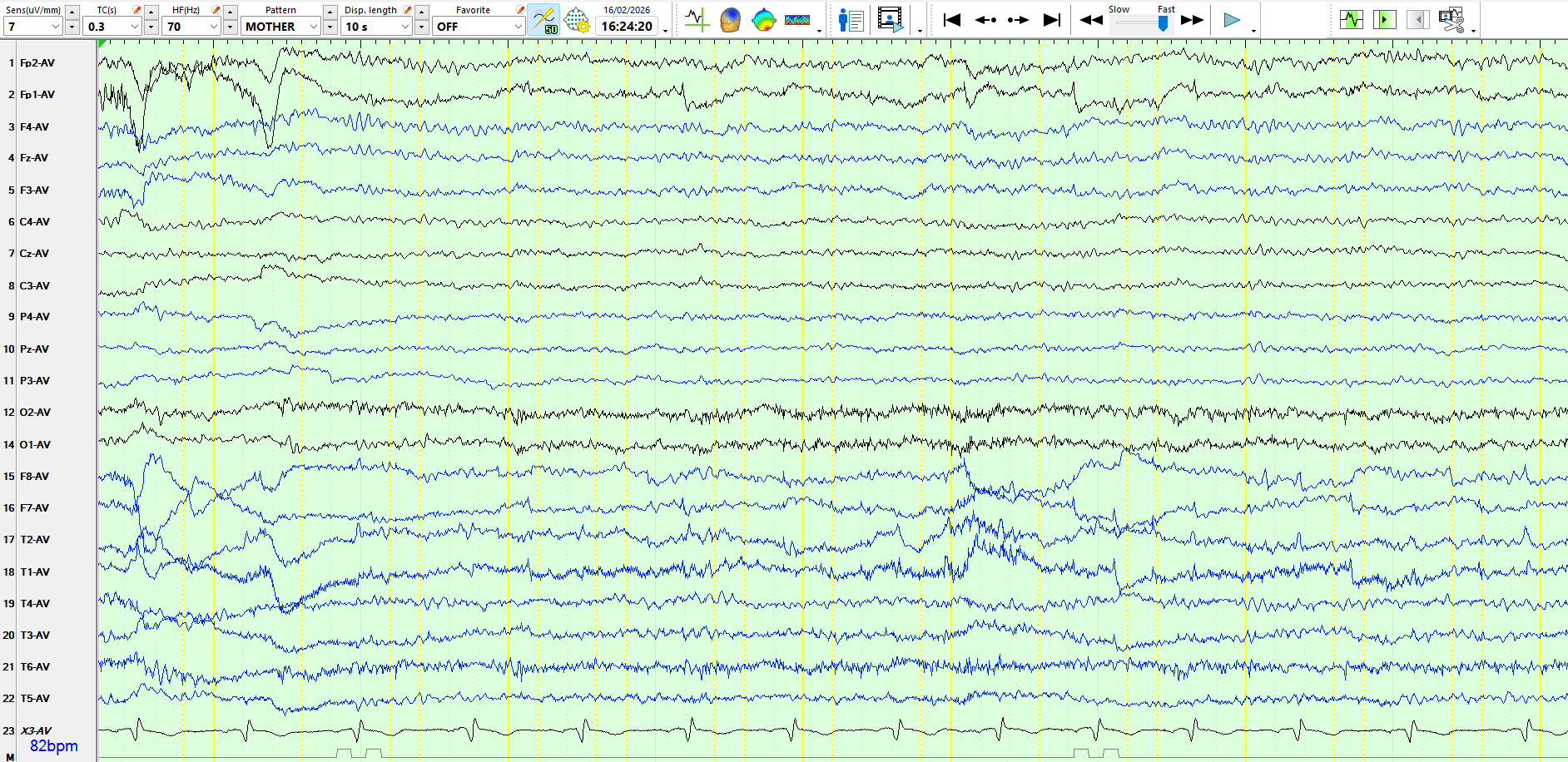
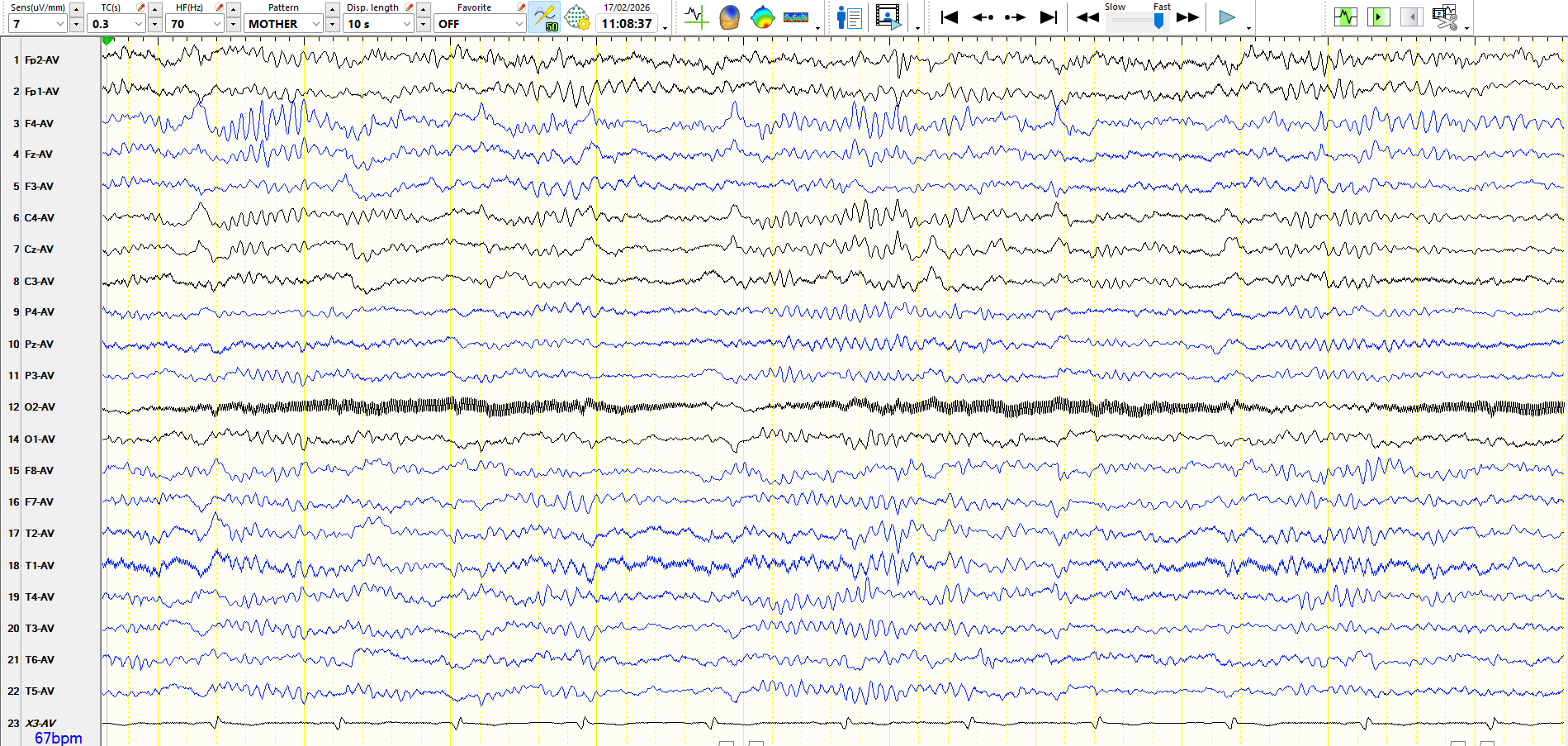
Just for good interest, from the latter patient:
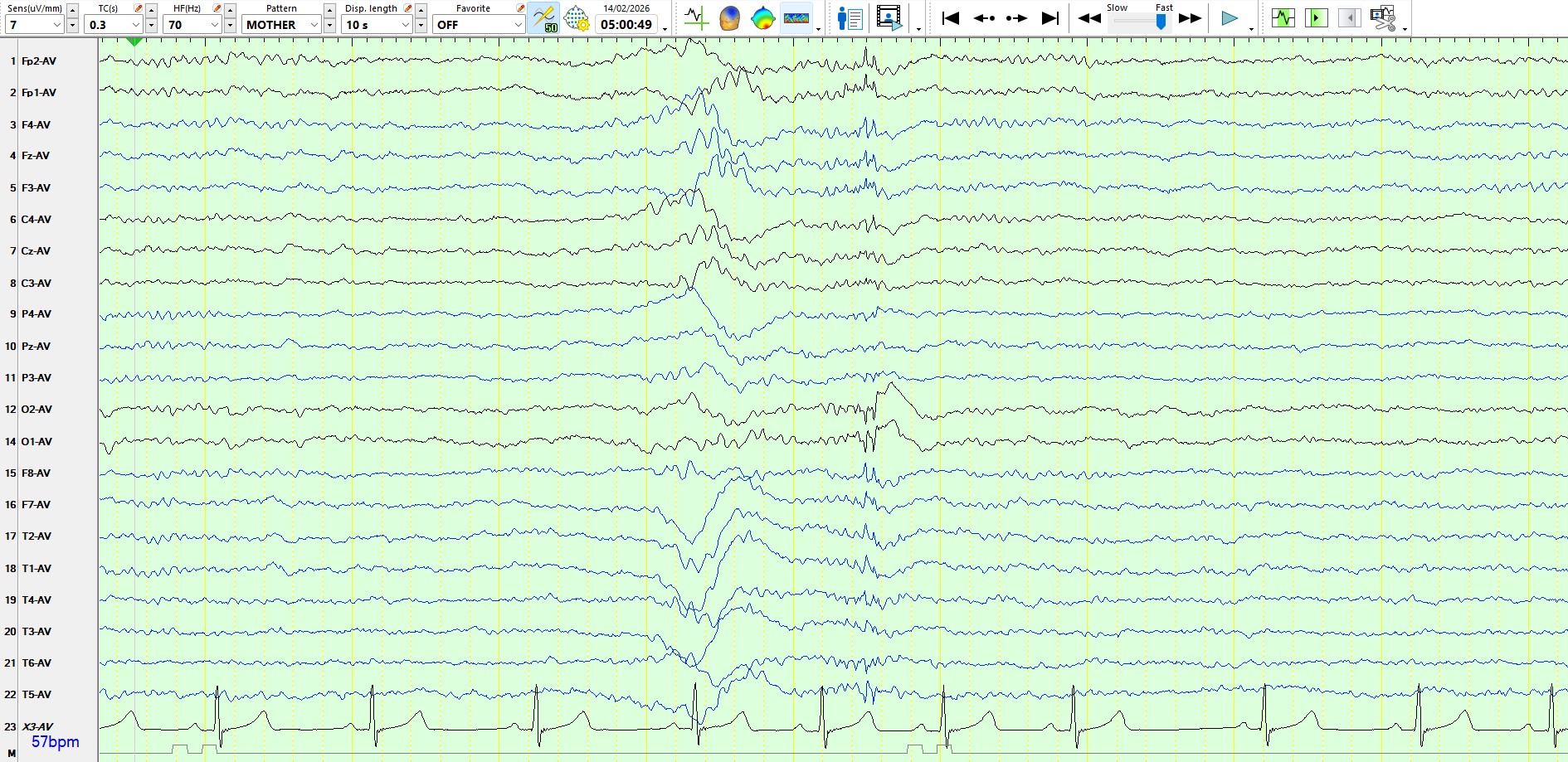
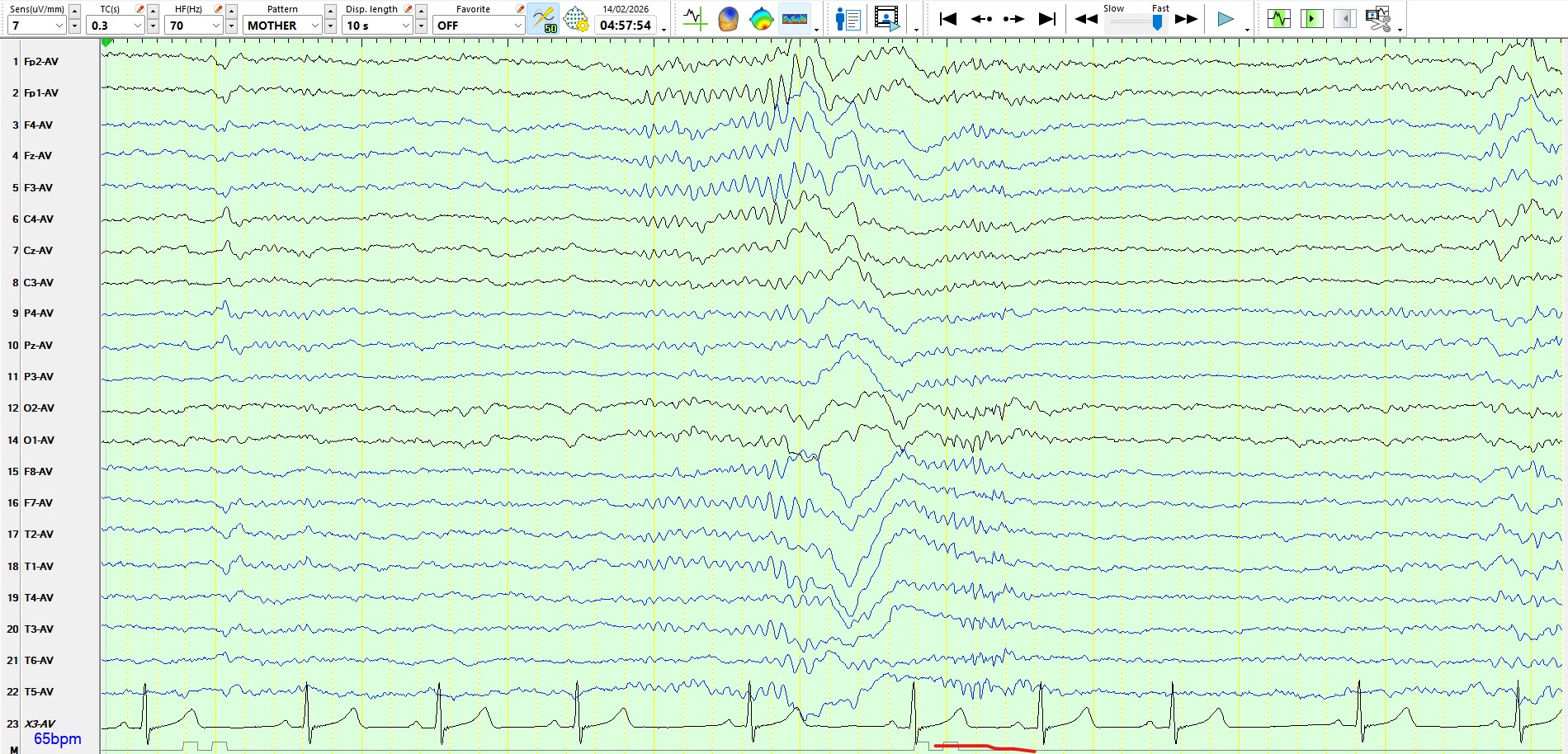
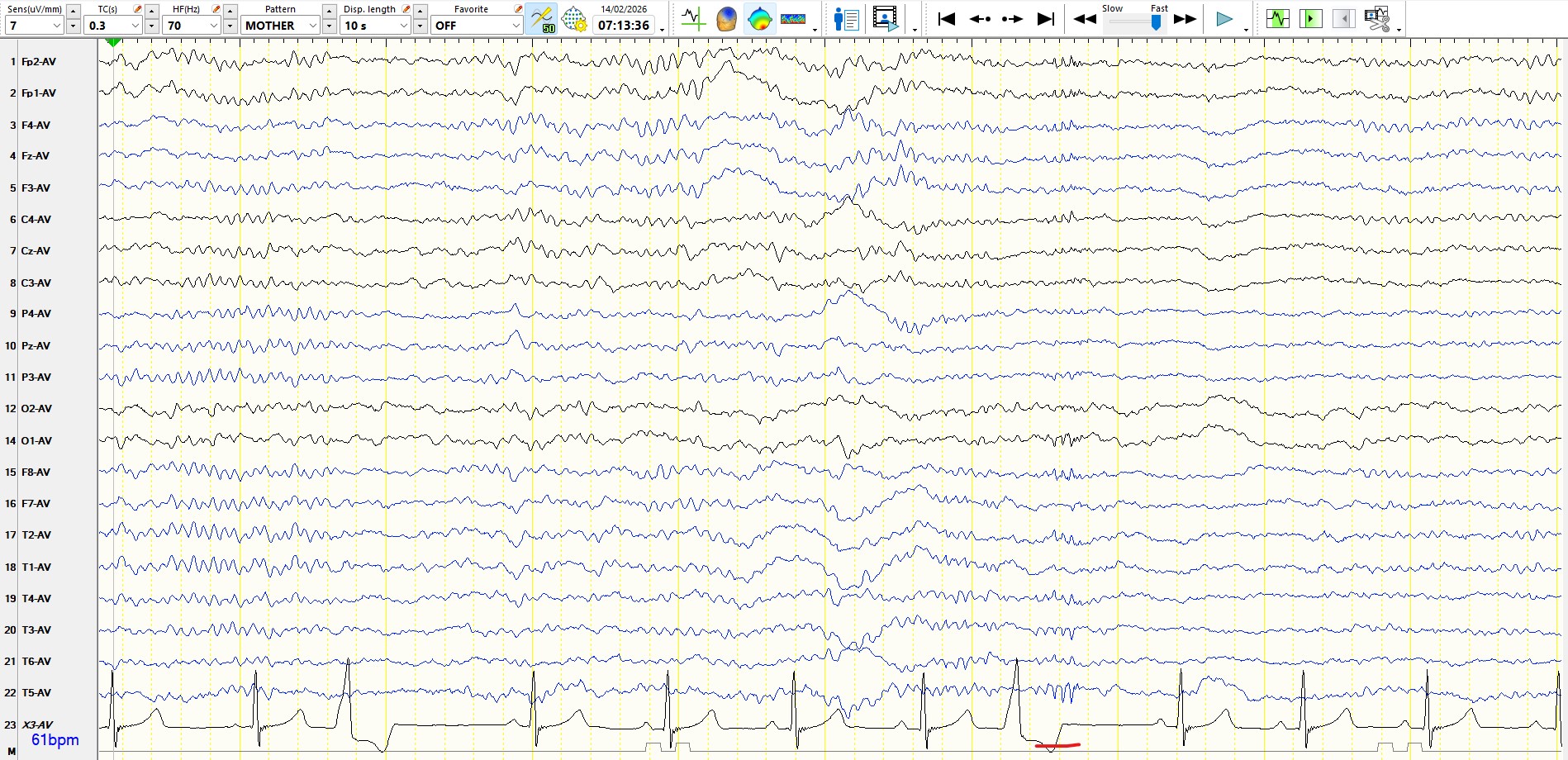
These are good examples of 14- and 6-Hz positive bursts. Sometimes, a very slow-wave following these can be particularly unsettling and misleading. The top image is a good example of the 14 Hz, followed by a wave that is certainly not within the 5-7 Hz range. However, this remains a 14- and 6-Hz positive burst! After all, the patient is in her early 20s, there are other typical 14- and 6-Hz positive bursts, and this burst has near-identical features to the other 14 Hz positive bursts.