
EEG - 11 year old with prolonged seizure
May 05, 2025
EEG 1:
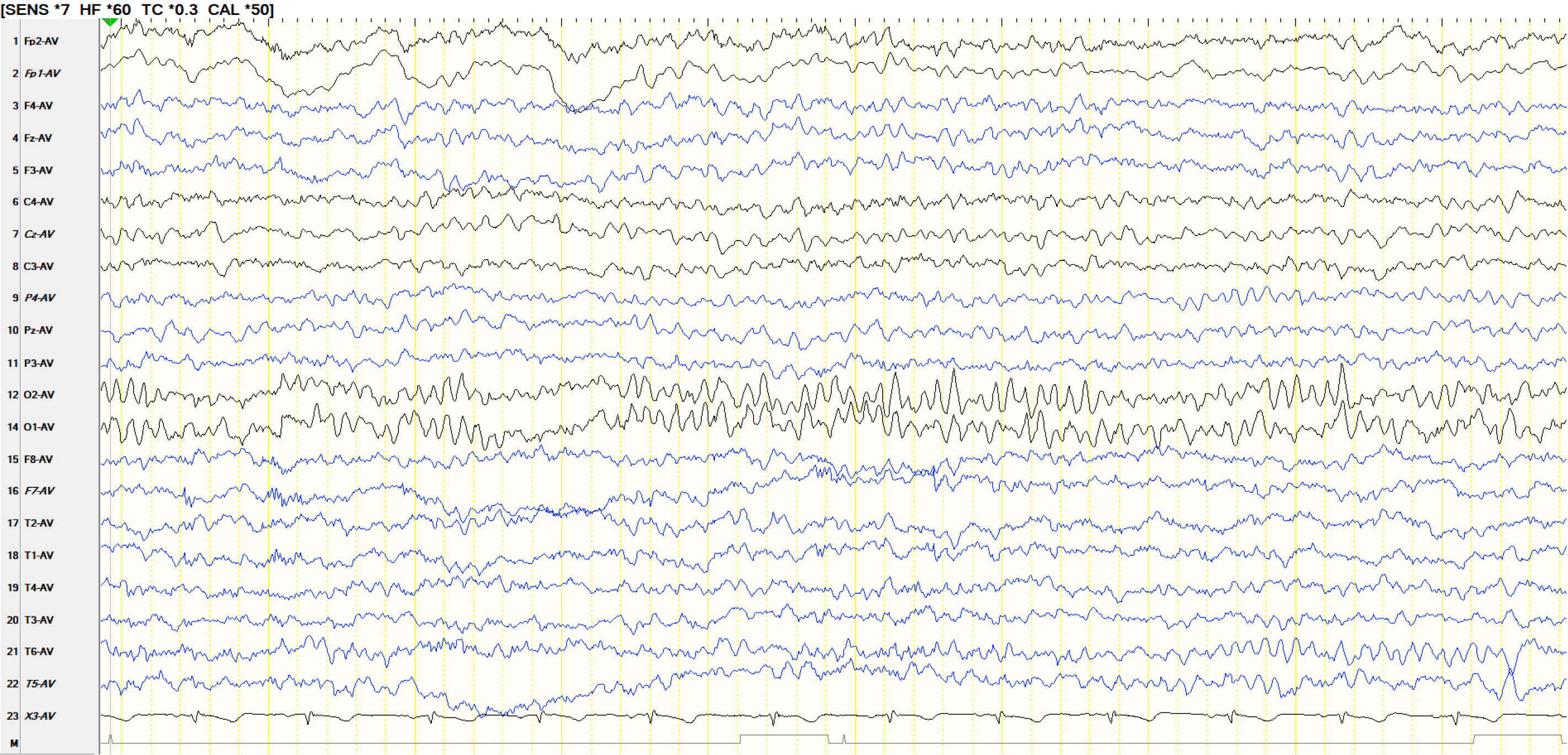
11 years old, normal awake recording. EEGs 1--10 apply to this patient.
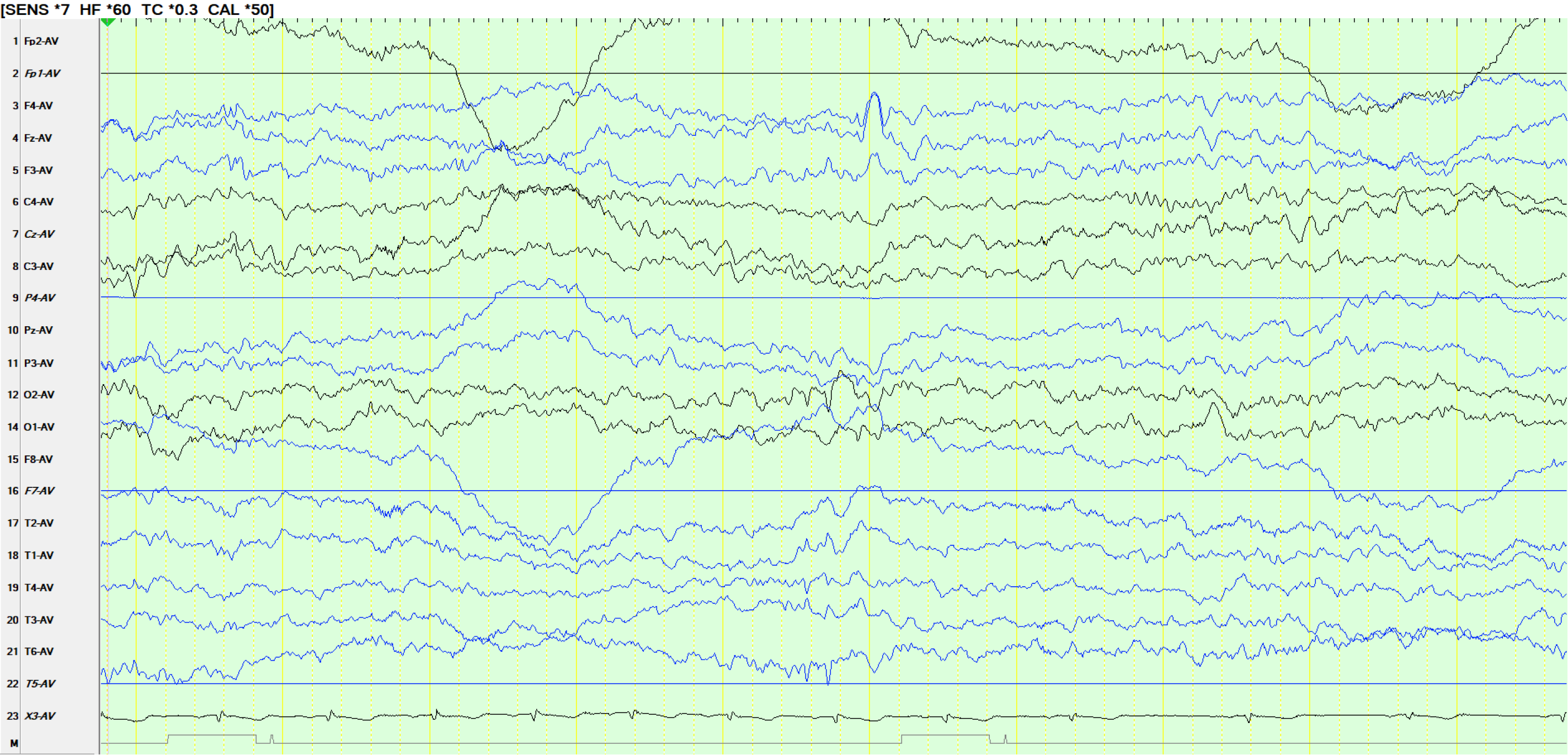
EEG 2:
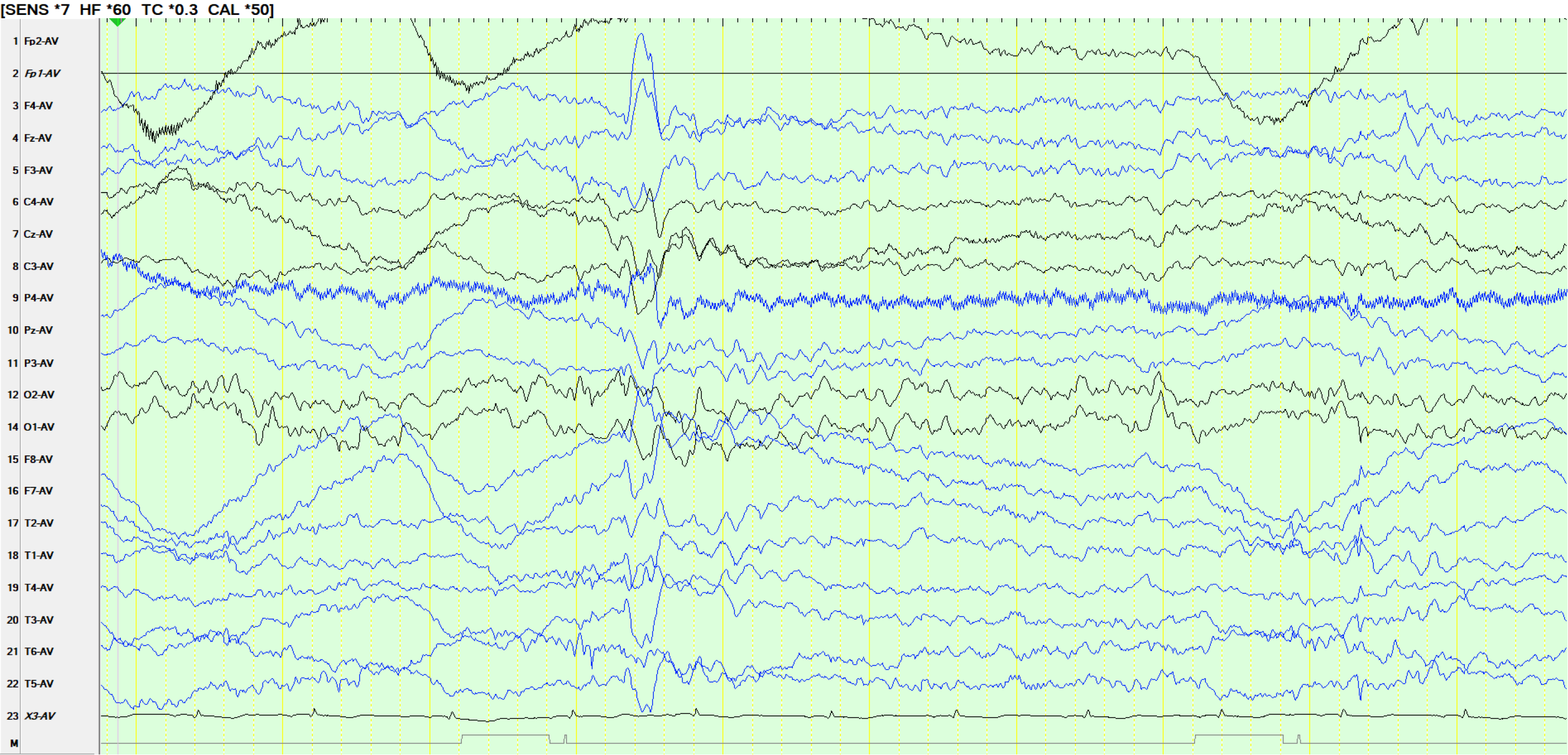
Sleep, notice "14- and 6-Hz positive bursts", most clearly seen in channel 21 (as the 14 Hz discharge) just above the 4th QRS complex. This is followed by a more widely-synchronous slower wave (the "6 Hz component). Small sharp spikes seen 2 seconds from the end of the recording.
EEG 3:
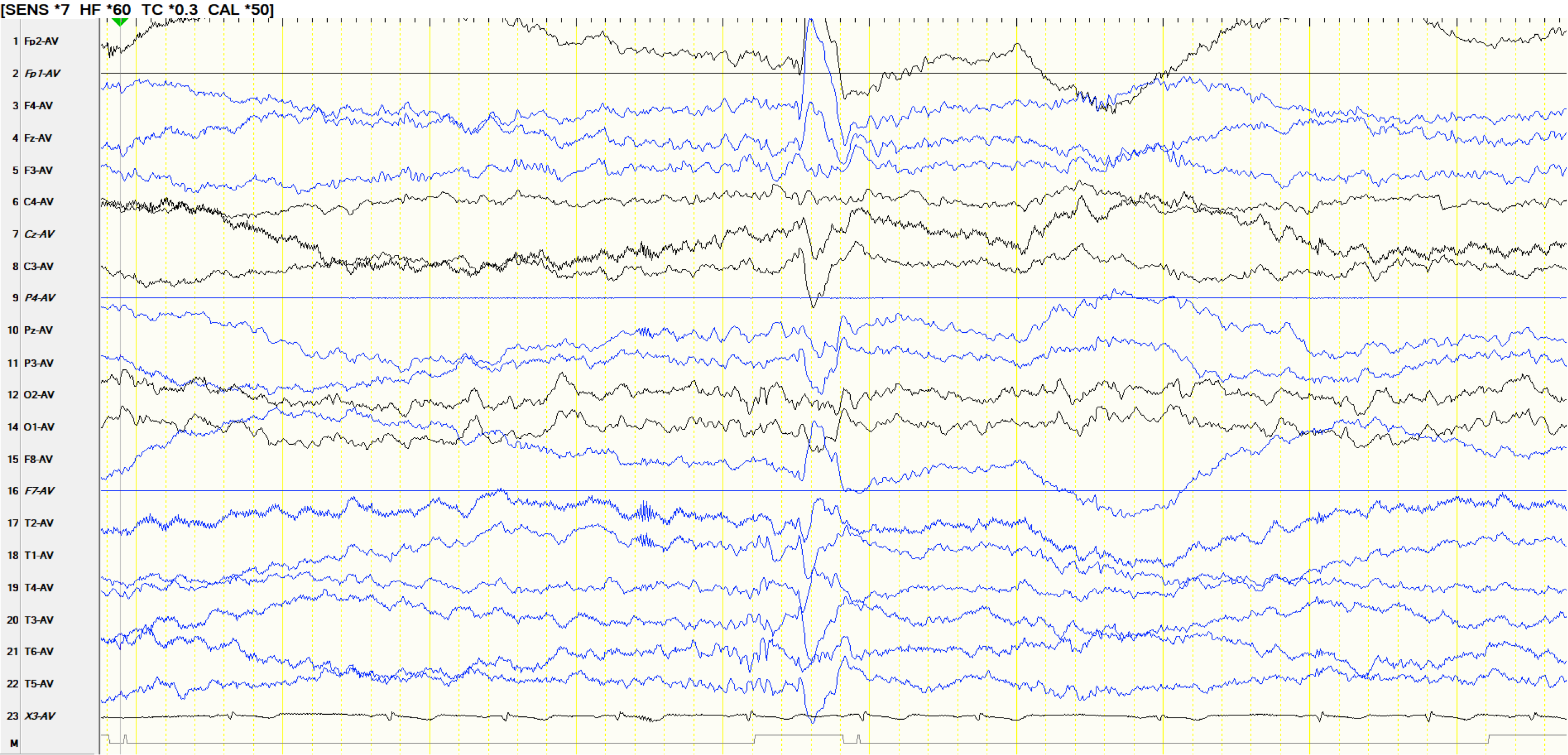
Similar discharge to the previous event. The slower wave following the 14 Hz discharge may be an F-wave, as it is not in the 5-7 Hz range. However, its association with the 14 Hz discharge suggests that it is a slower version of the "6 Hz".
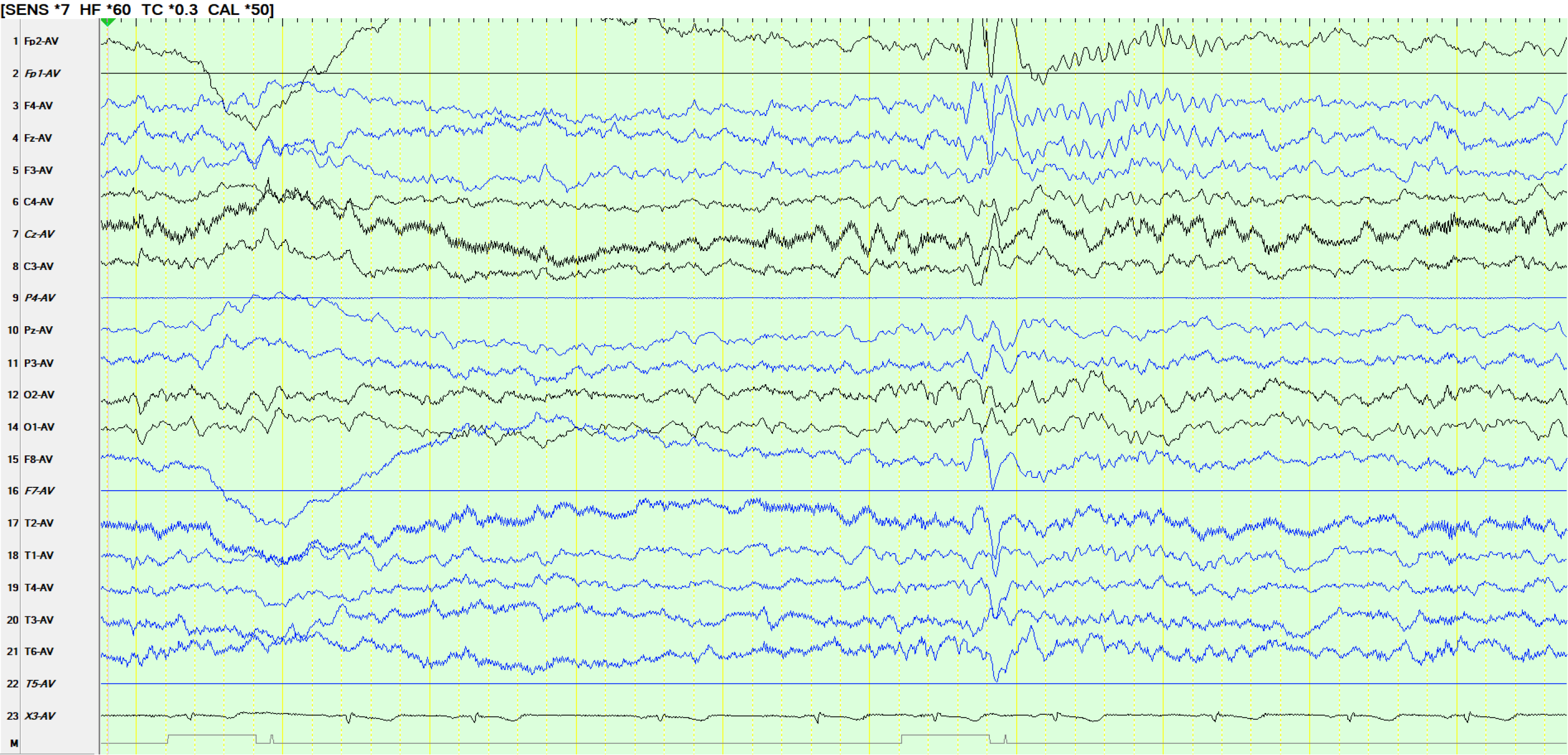
EEG 4:
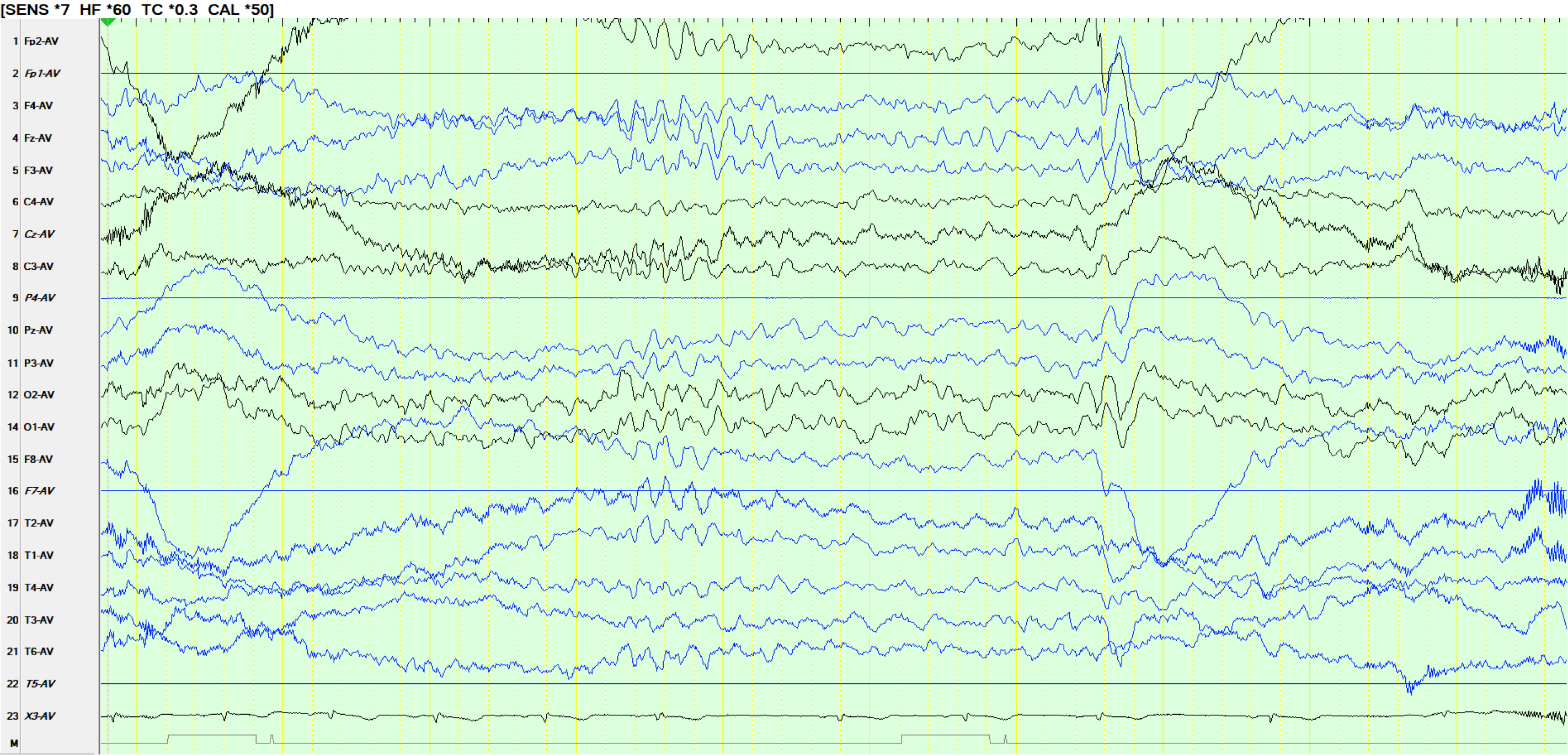
On this occasion the occurrence of the very sharply-contoured wave form at FP2-FZ-F4-F3 (FP1 artifactual) raises concern about a fragment of generalized spike-and-wave. Because of the possibility of the 6 Hz component of 14- and 6-Hz positive bursts (which are present in the same patient elsewhere during sleep), it is best to avoid calling this a generalized spike-and-wave until there is further evidence of this during the same recording. Burst of hypnagogic hypersynchrony at about 4s from the beginning of the page.
EEG 5:
The 14 component of 14- and 6-Hz positive bursts is well seen in channel 21 and 12, with opposite polarity at 20, 18. Some of the 6 Hz waves can be seen in channel 12. This is followed by a slower wave in channels 3, 4 and 5, either representing the "6 Hz" component of 14- and 6-Hz positive bursts or an F-wave. The temporal association suggests the former
EEG 6:
The patient is still asleep. There is a sharply contoured waveform after the first of 2 slow waves and this occurs synchronously with a similar discharge at F8, FZ, F4. However, notice that this is preceded by the 14 Hz discharge in channel 21 and the latter appears to be time-locked to the former waveform, making it likely that this is the 6 Hz component of 14- and 6-Hz positive bursts. While it may be tempting to do so, this should not be called generalized spike-and-wave or right frontal spike-and-wave. Notice that the sharply contoured wave forms preceding frontal slower waves in all the epochs above are relatively low in amplitude when compared to the slow waves.
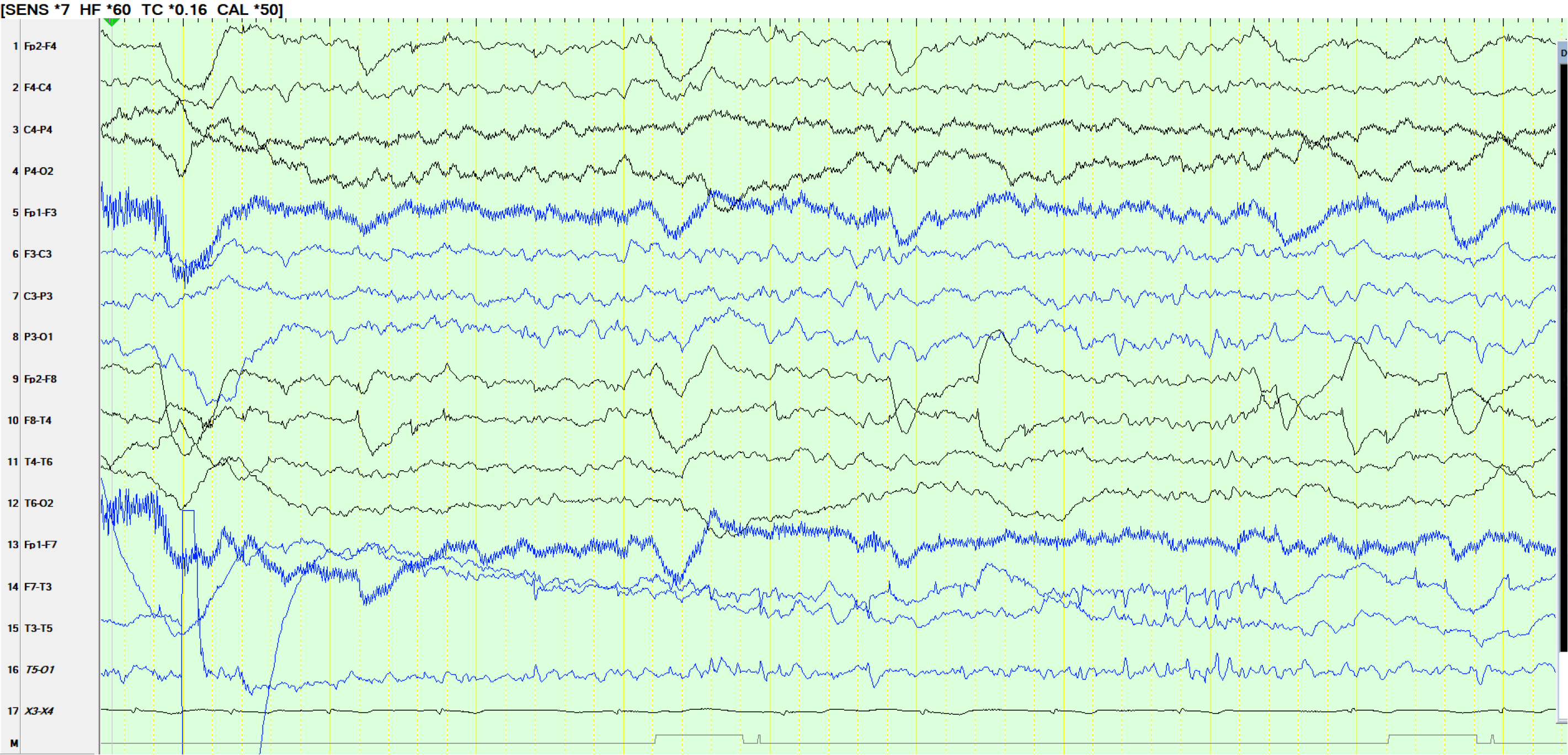
EEG 7:
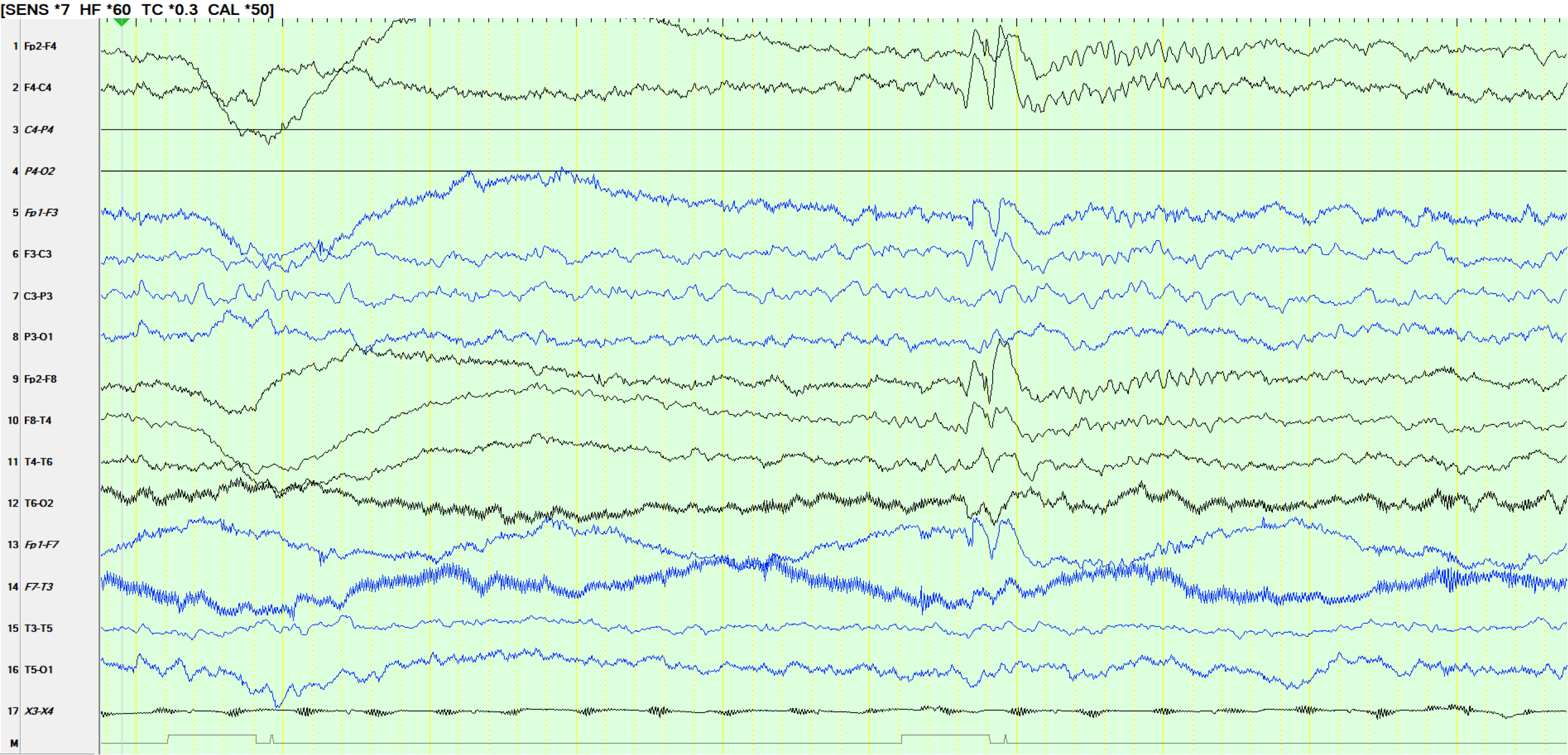
The same page as above on bipolar montage but notice how you would miss the 14 Hz and therefore erroneously call this a spike and wave. Such low amplitude "spike-and-wave" should always mandate caution about calling these spike-and-wave discharges.
EEG 8:
More of the 14 Hz, resembling polyspikes (which they are not). The widely synchronous slower waves at the end of the 14 Hz discharge represent fragments of the "6 Hz" discharge.
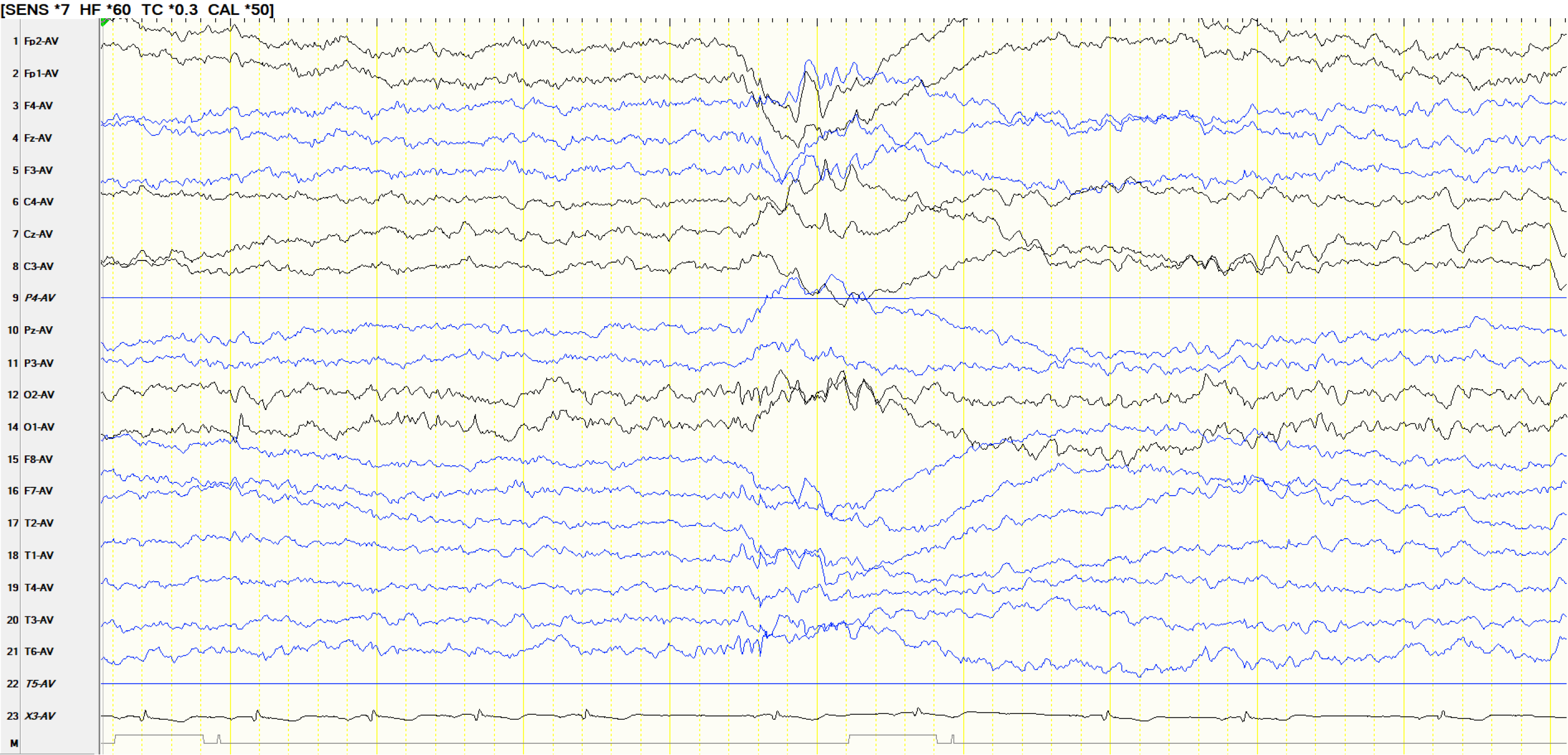
EEG 9:
This is the first direct EEG evidence of a prolonged seizure, here seen over the left mid-posterior temporal region, in the same patient as above. The patient woke up approximately 40 seconds earlier.
EEG 10:
The inter-ictal is normal during wakefulness and sleep. Left mid-temporal spikes (T3-P3-01; T5 is artifactual) appear exclusively during the early post-ictal period. These are congruent with the first appearance of the seizure on EEG and very useful in this patient as there is no clear discharge for the first 40 seconds of the seizure posted above.
Please maintain patient confidentiality by refraining from discussing cases presented in the meetings with others, in the same way that you would do for your patients. Please also avoid recording the meeting. Remember that breaches of confidentiality that lead to a patient complaint are likely to result in severe censure from HPCSA. Such breaches of confidentiality are likely to be traced.