
65 years old, talking, very poor history (encephalopathy)
Jun 06, 2025
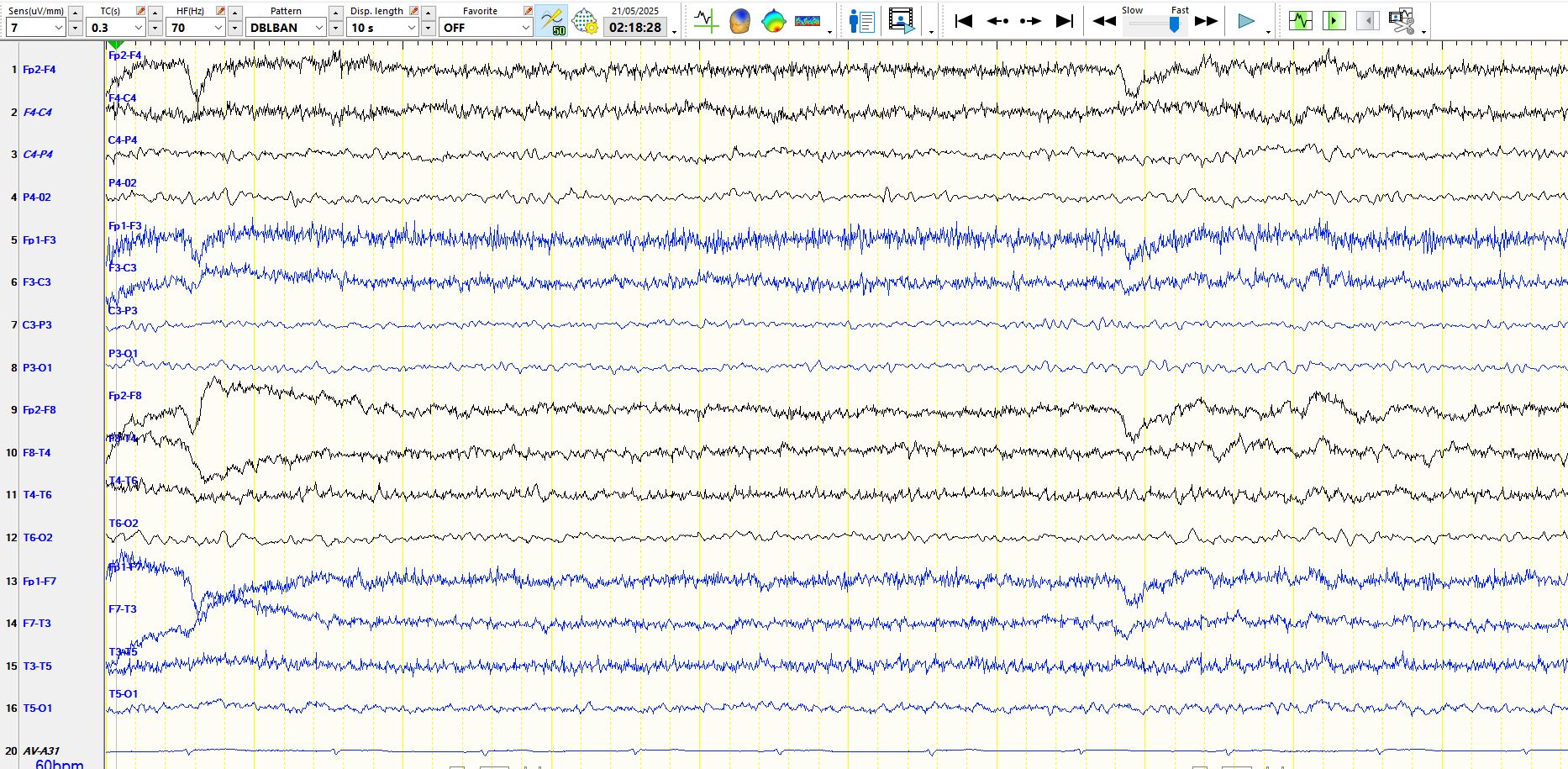
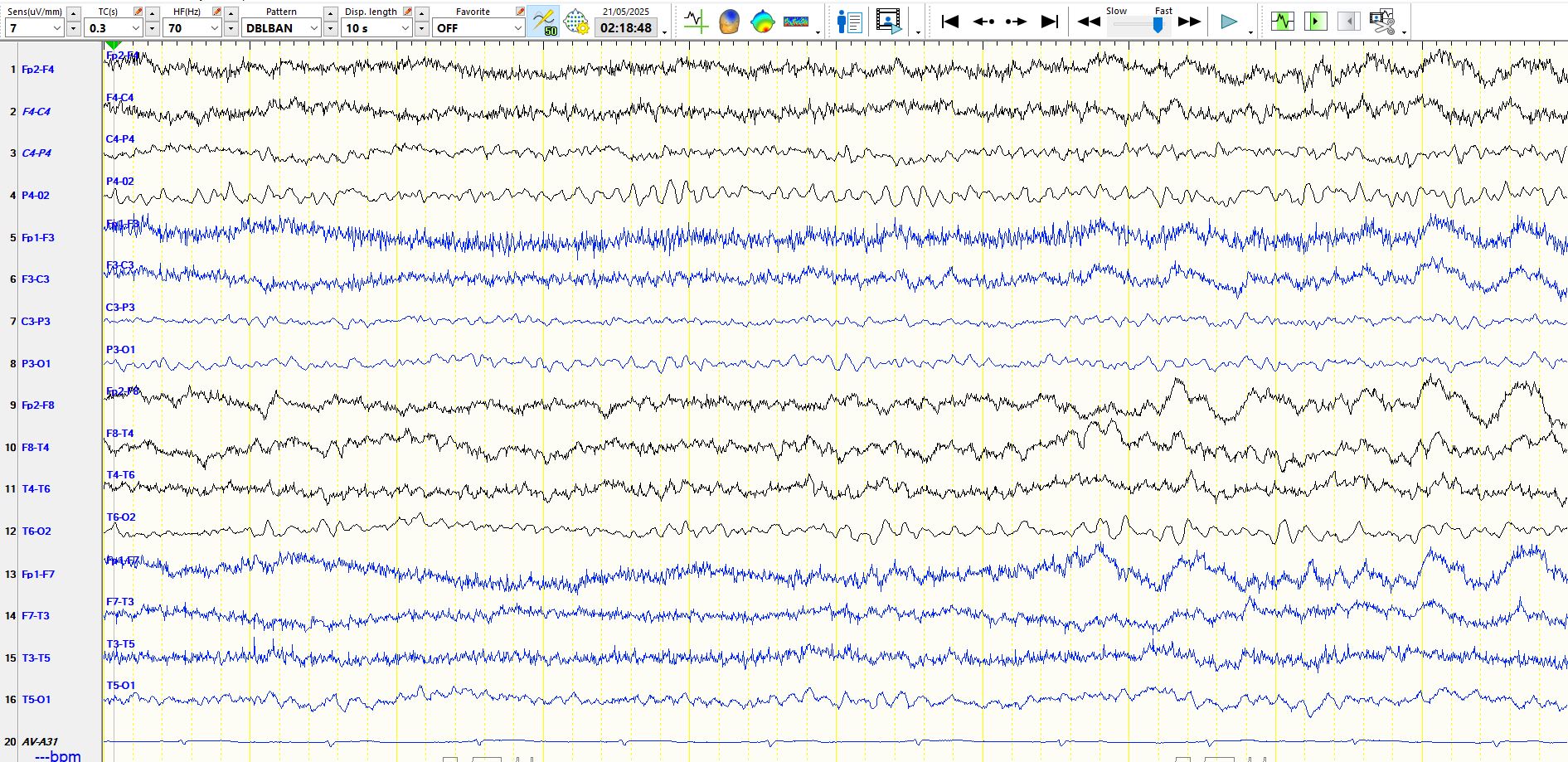
The page above is unremarkable

Notice how the EEG recording may be normal at times, despite a very obvious encephalopathy at the bedside
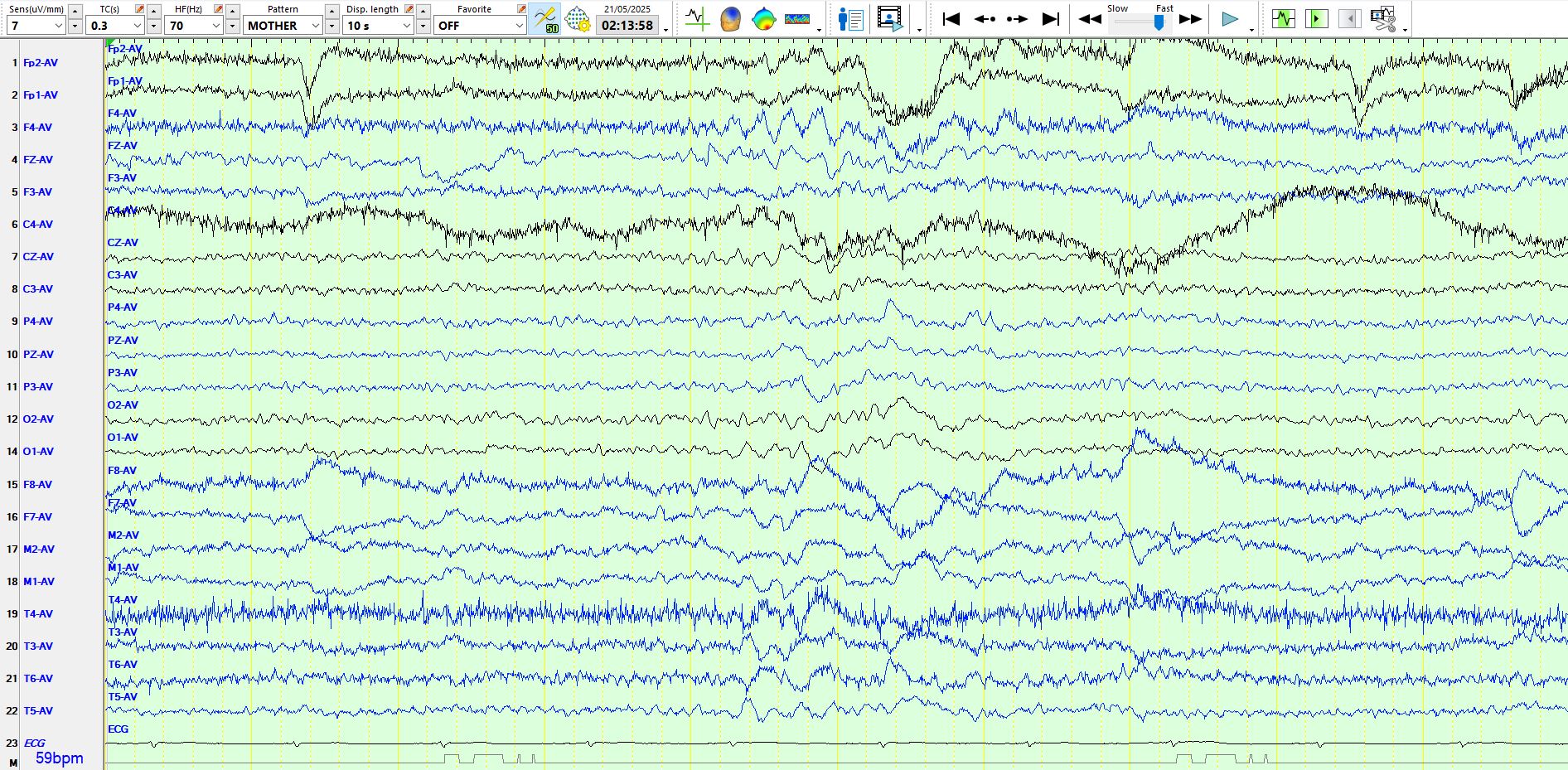
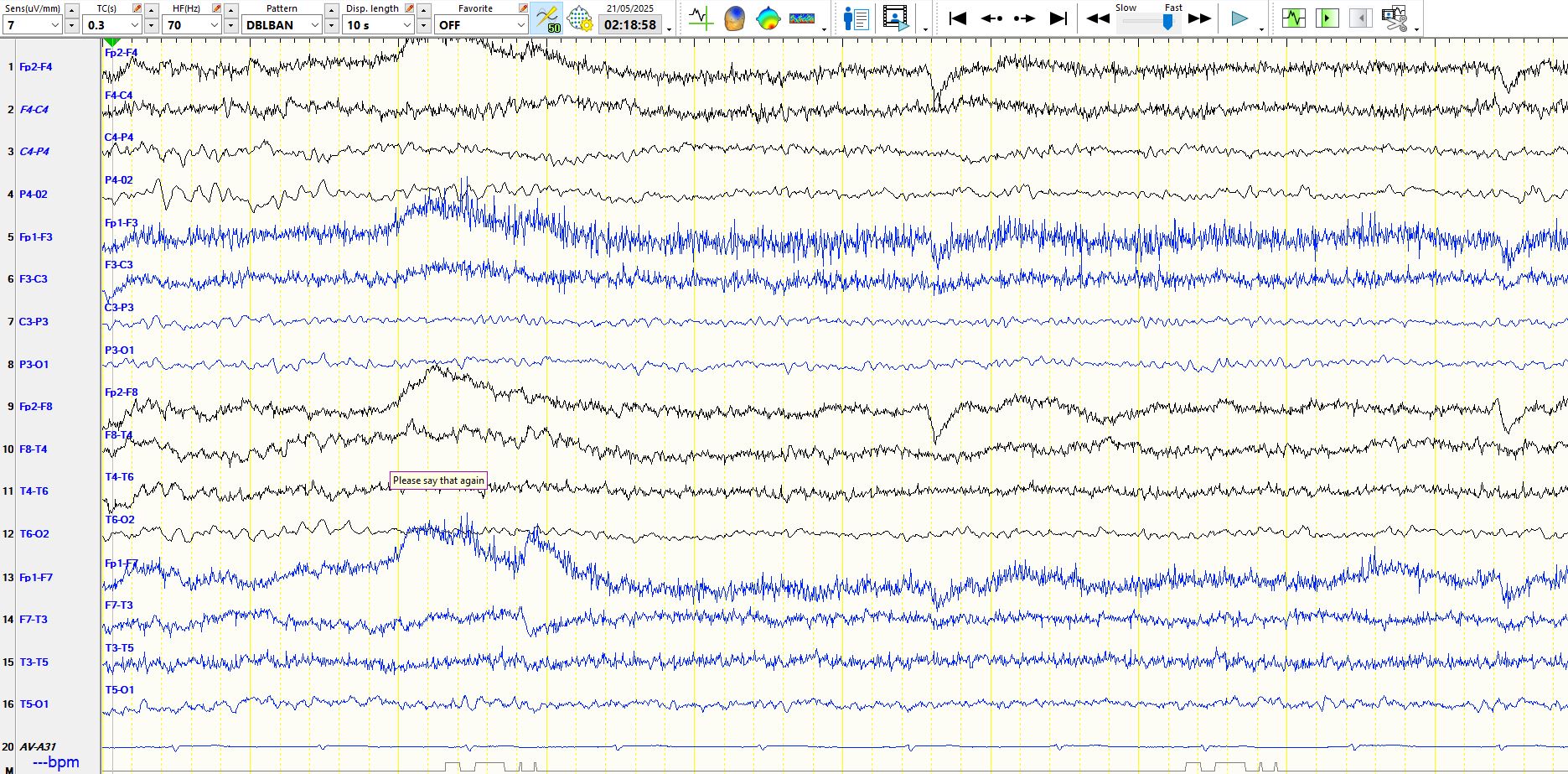
In the middle of the page above there is a burst of theta and delta waves, indicative of the encephalopathy
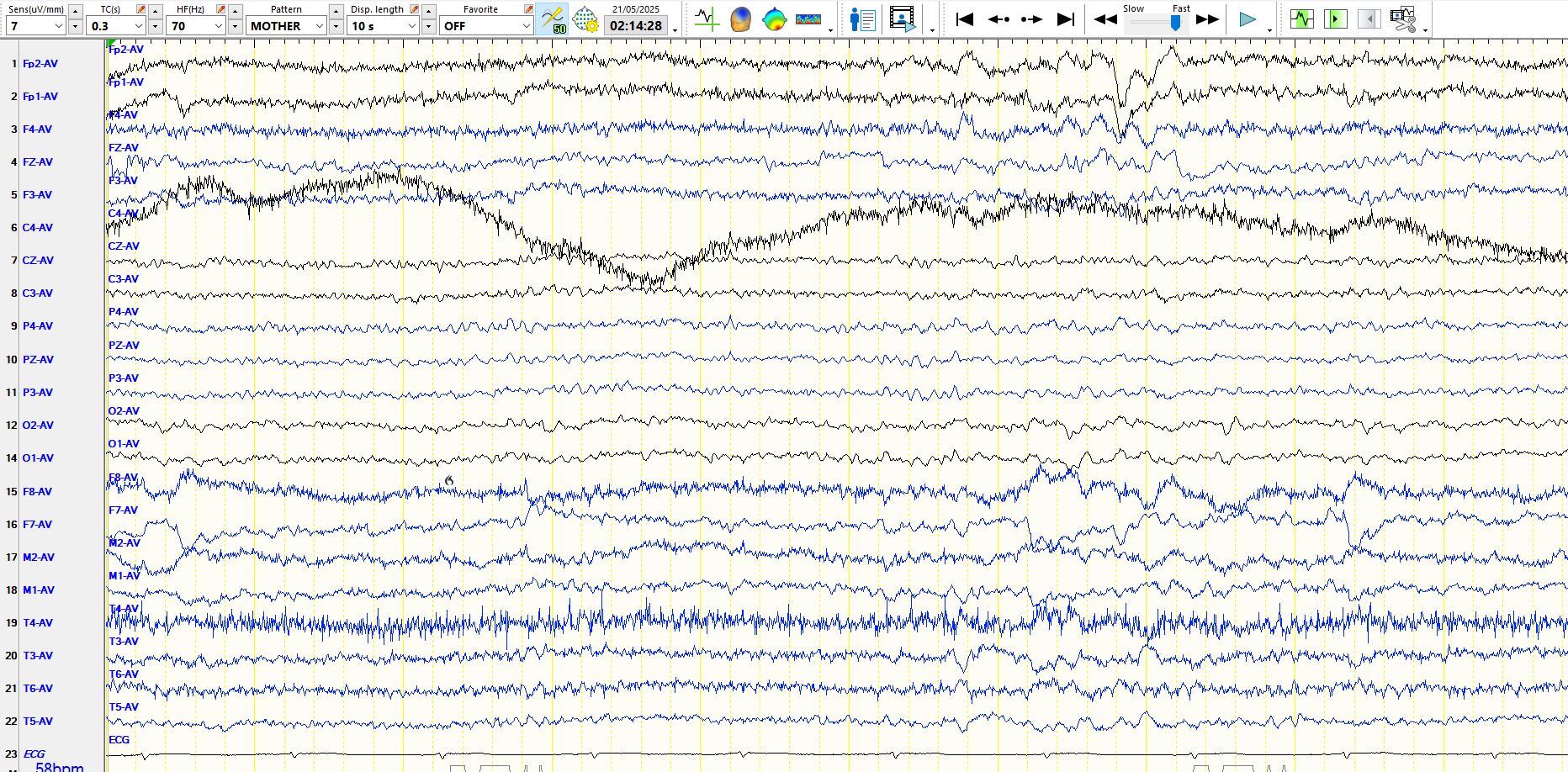
Similarly, the EEG above shows diffuse the term Delta in the second half of the page
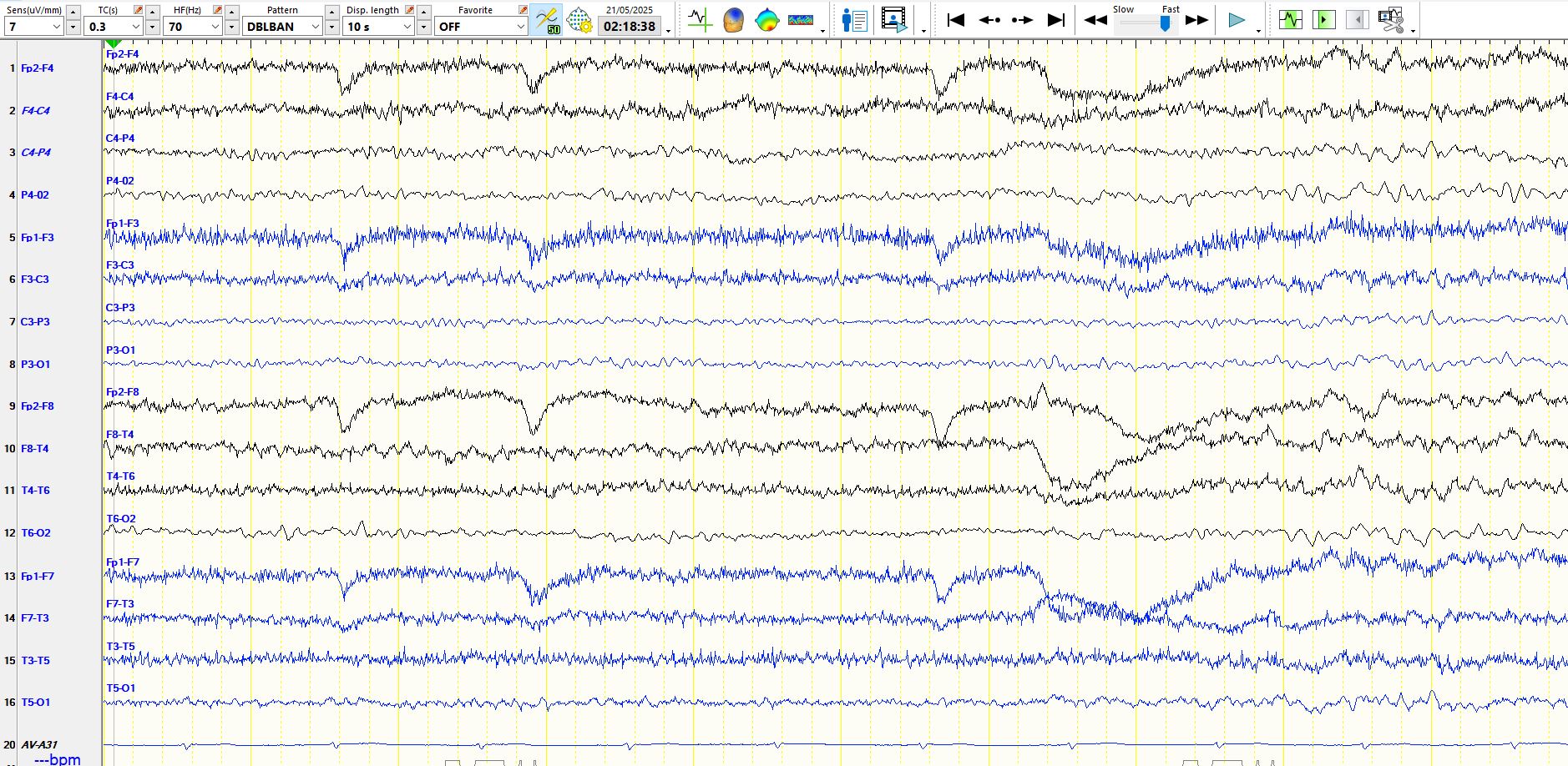
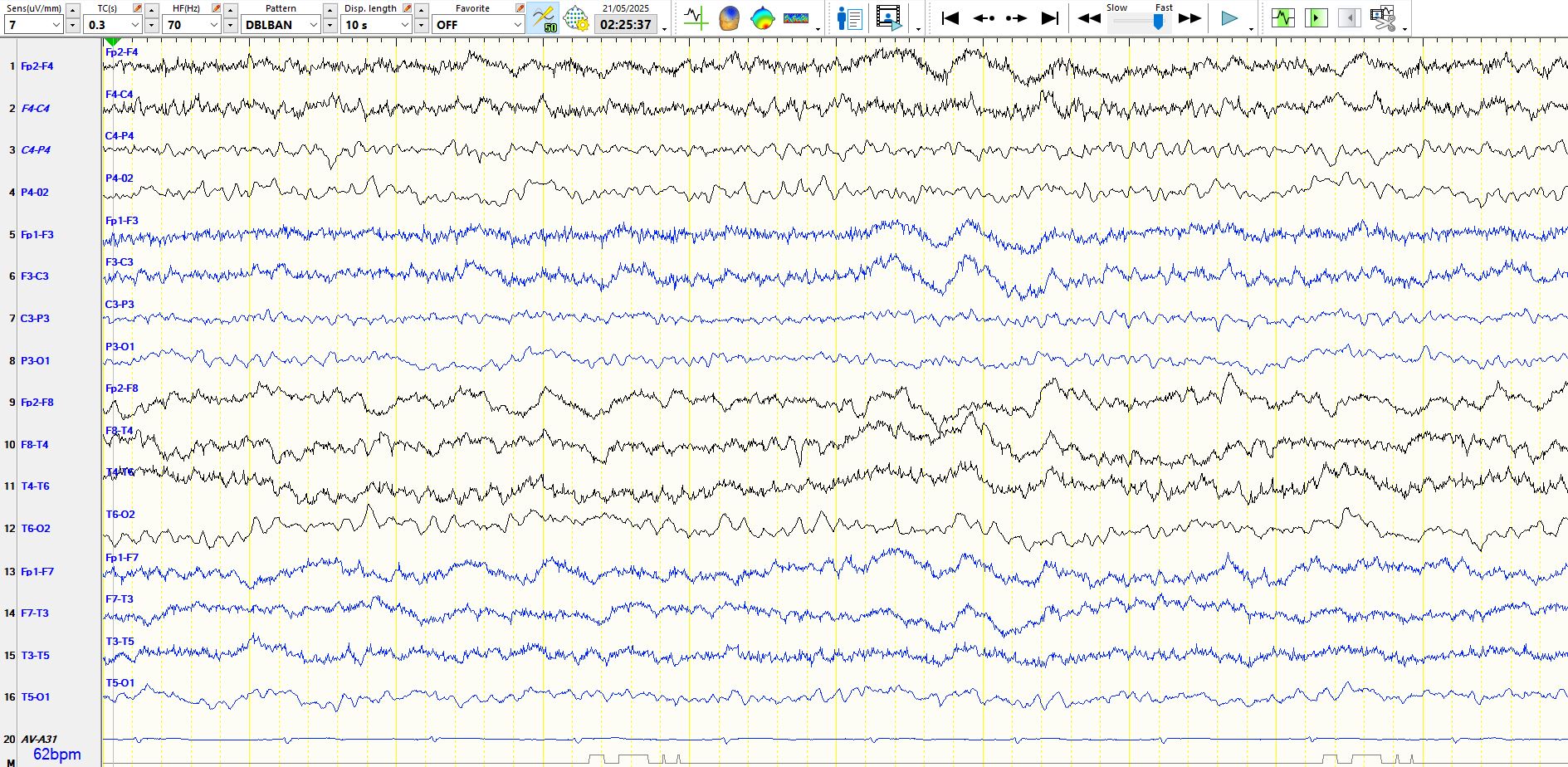
Drowsiness is often a feature of encephalopathies, both clinically and on EEG, see above and below. However, notice the delta waves above.
On the page above, Diffuse theta waves appear in the last few seconds as part of the drowsy pattern, preceded by slow eye movements and therefore difficult to distinguish from physiological drowsiness
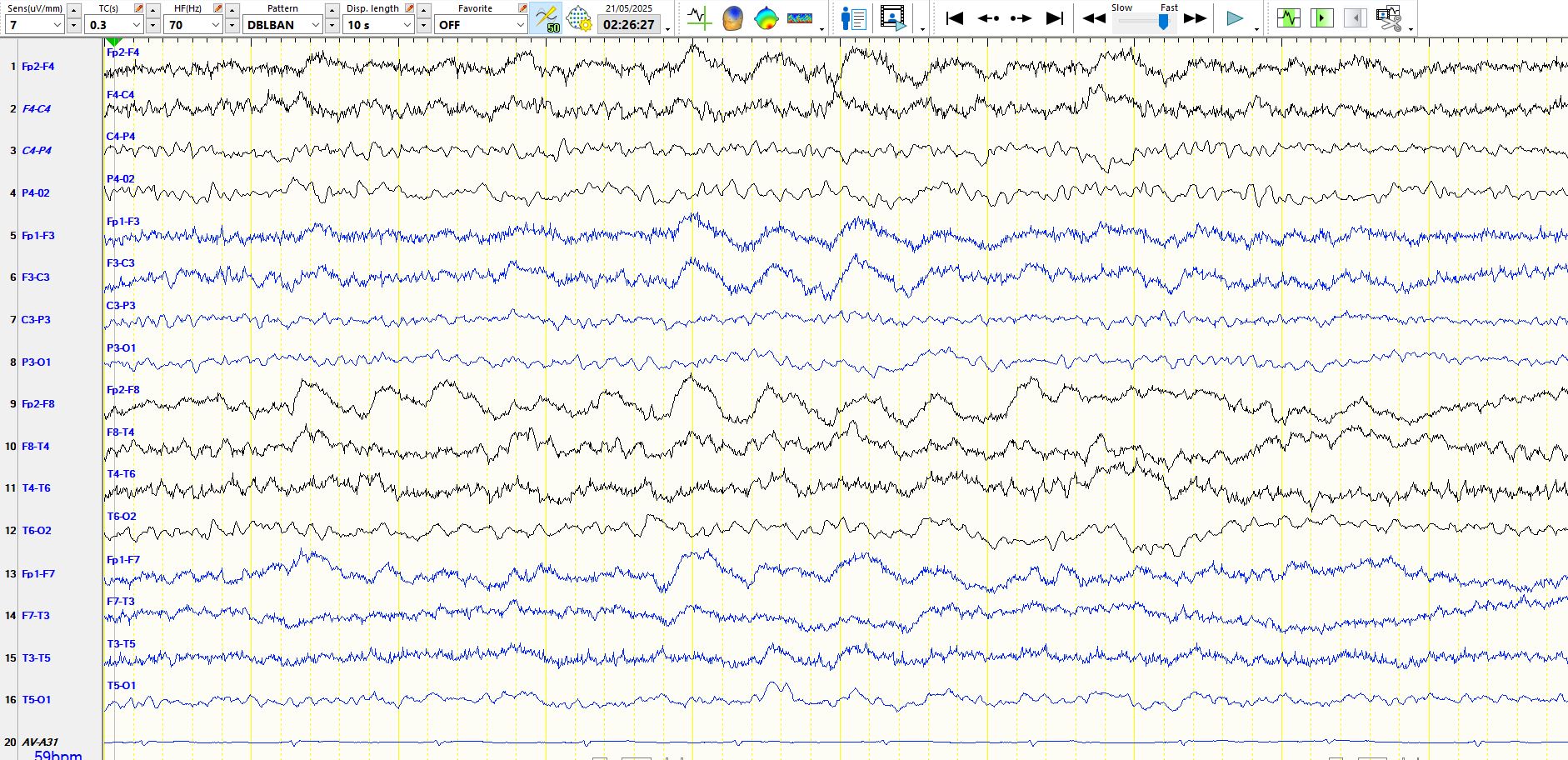
In contradistinction to "physiological drowsiness", note the early appearance of rhythmic, frontally-predominant delta waves during the last few seconds of the page below, preceded by a relatively normal recording, albeit minimally drowsy, but not abnormal, prior to the appearance of the delta waves
Below is another page that is normal despite a very obvious encephalopathy on history taking.
A mixture of alpha and delta frequencies highlights the encephalopathy (See below). The frontal intermittent delta waves become apparent
The page above and below start to raise the possibility of frontal intermittent rhythmic delta activity
As the patient falls asleep, K-complexes appear. Note the duration of this K complex below. These waves, resembling K-complexes, appeared abundantly during the early stages of sleep and I wondered whether these were possibly "pathological K-complexes" as there were no associated spindles and V-waves. They were also consistently of long duration. K-complexes may be as long as 1.5 seconds, but these waveforms dominated the recording at times during the early stages of sleep; hence, one might say that the architecture of early sleep was abnormal.

Unlike physiological drowsiness, page below demonstrates the evolution from wakefulness to drowsiness, with the early appearance of frontally-predominant delta waves, here seen right frontally (patient previously had a stroke in the right frontal region).
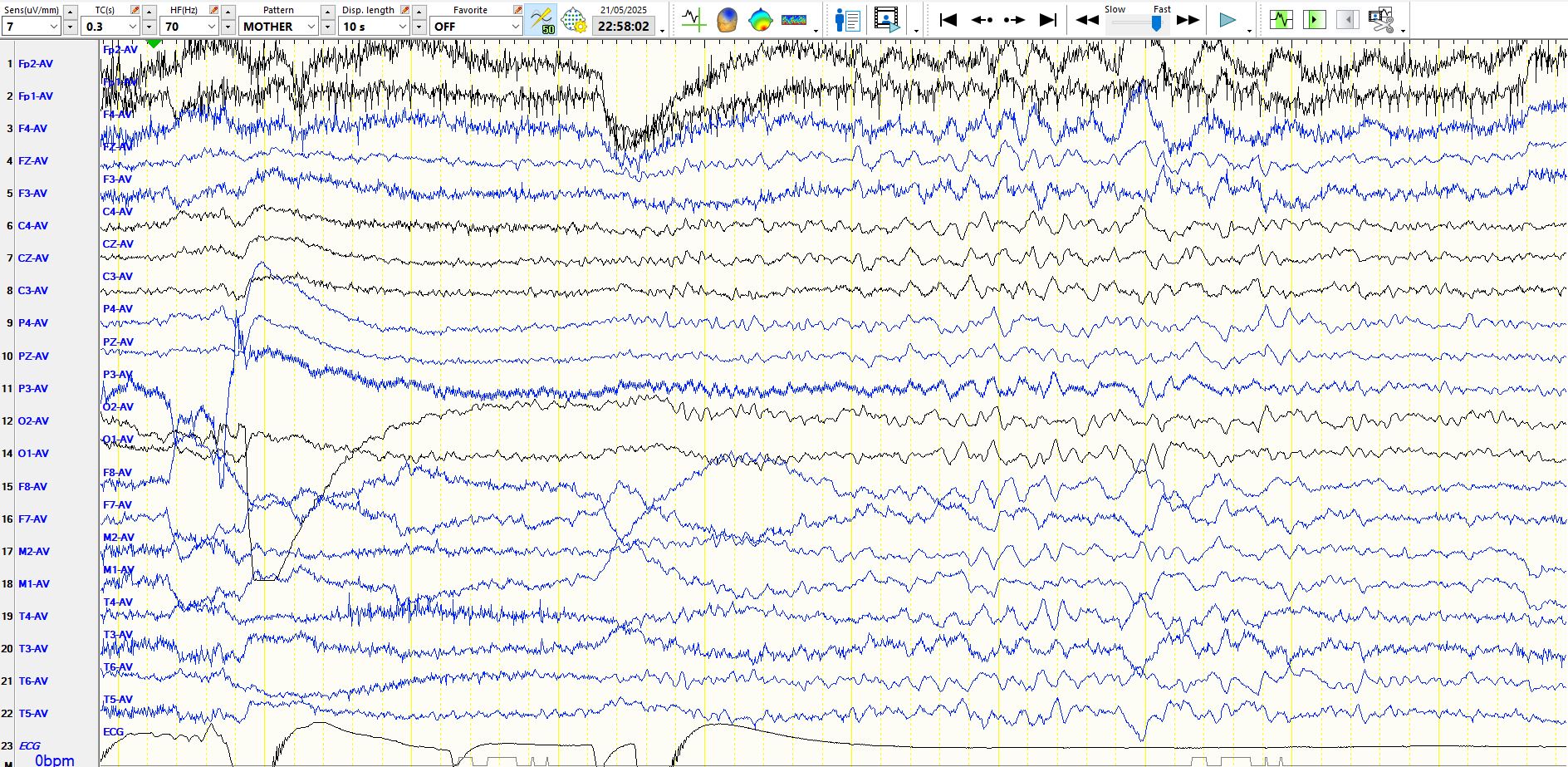
What do you make of the following 3 pages, which follow one another?
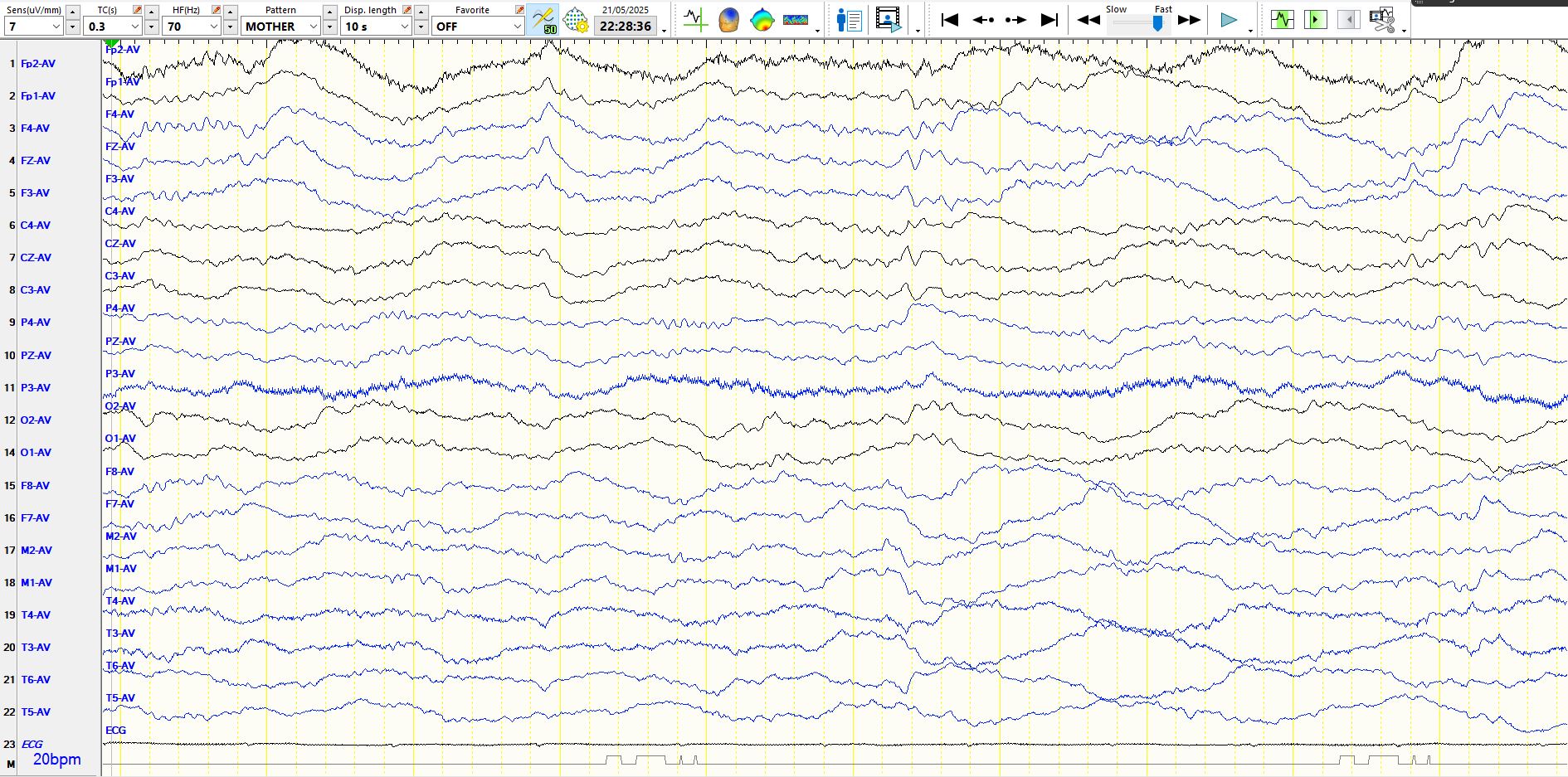
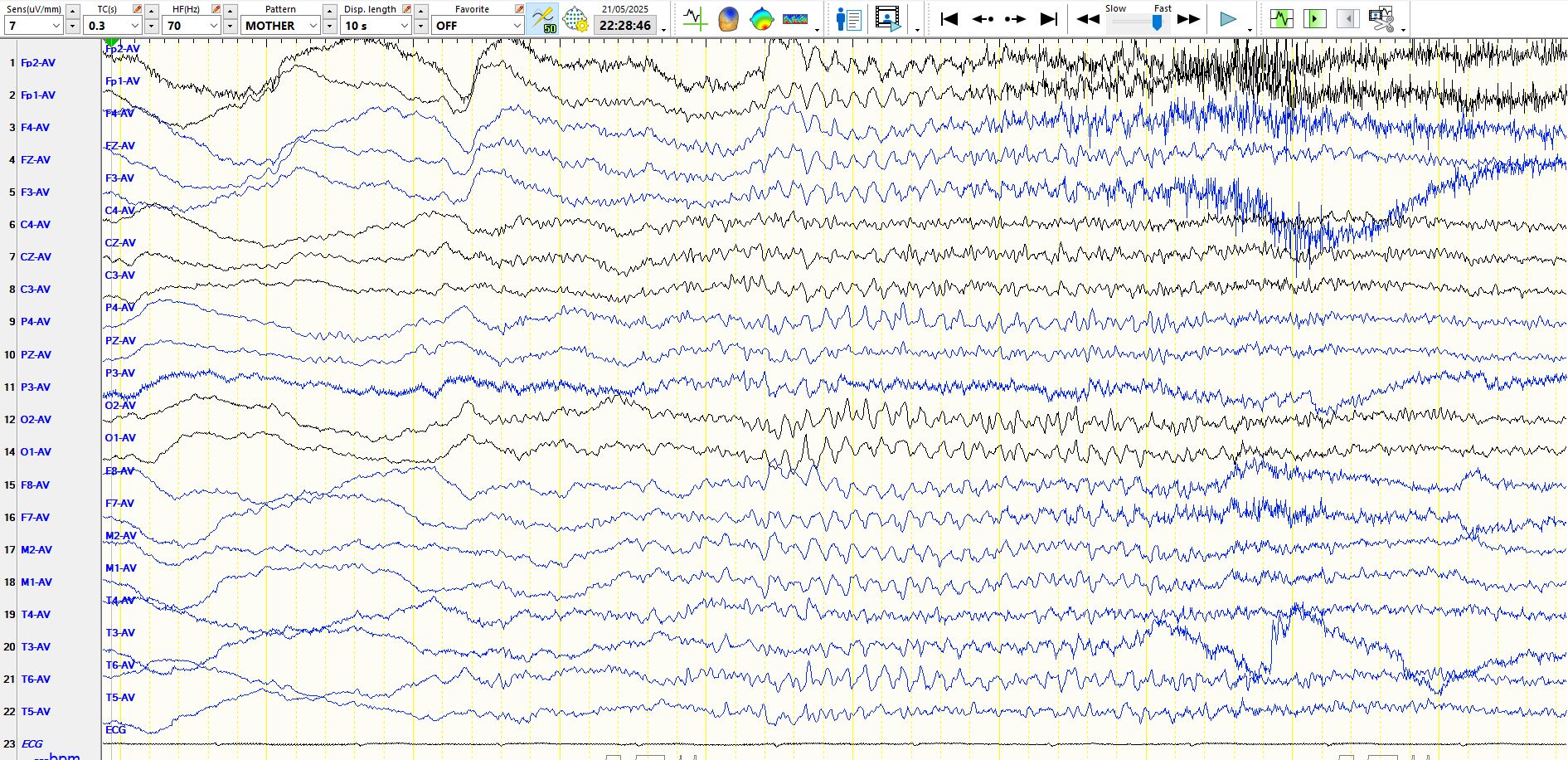
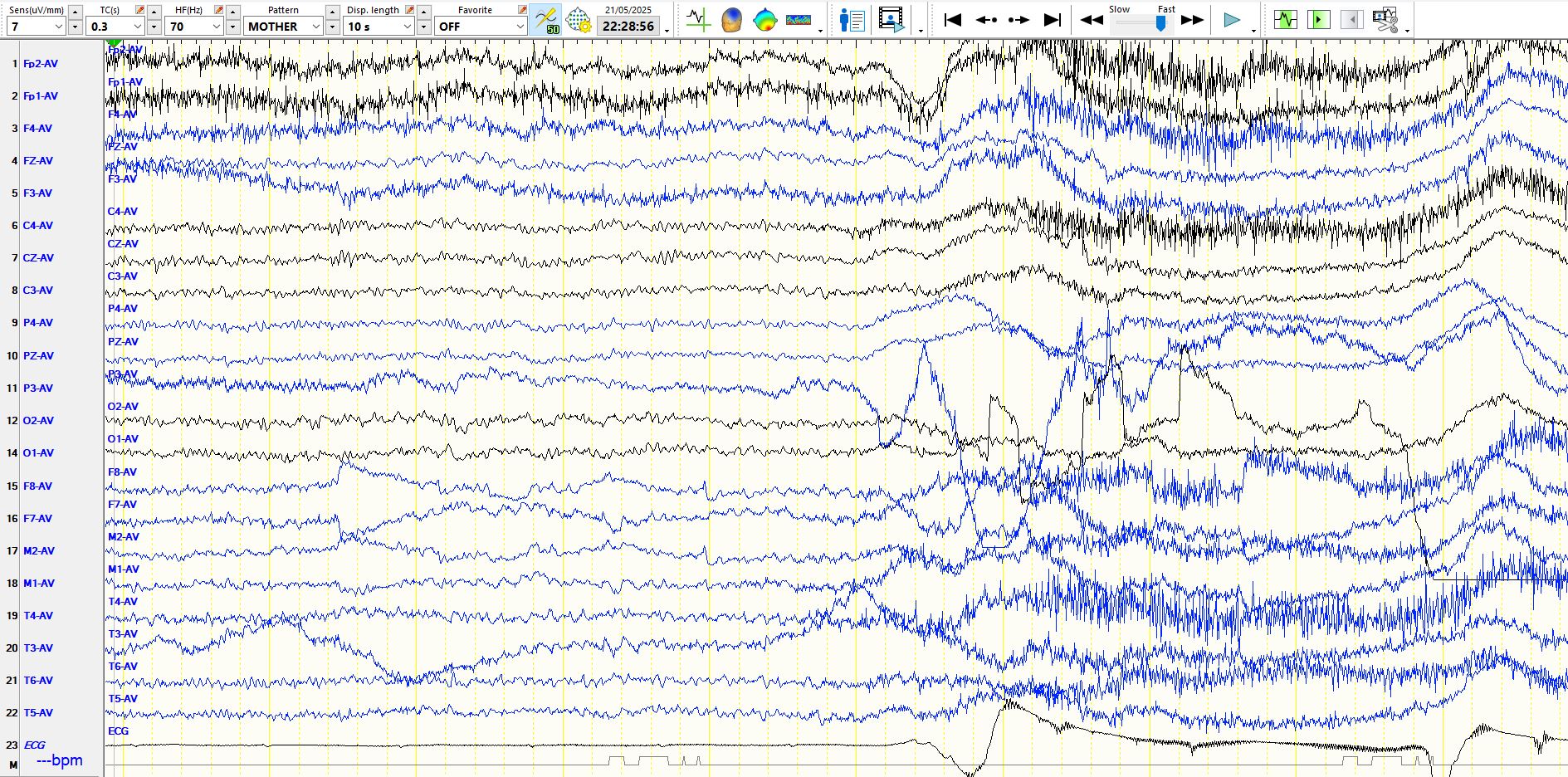
The first page demonstrates that the patient is asleep, but these very slow delta waves are indicative of an encephalopathy. The 2nd page above demonstrates arousal, with a progressive increase in frequencies as arousal occurs, superficially resembling a seizure. Seizures may rouse patients and one has to be especially careful of evolving frequencies at the time of arousal; arousal has a fascinating array of EEG manifestations. The 3rd page above demonstrates that the patient is awake, albeit encephalopathic on clinical examination, while the EEG during this 10 second period is normal.
The EEG of this patient highlights the range of EEG manifestations seen over time in someone with an encephalopathy, ranging from brief periods of normality to an obviously abnormal EEG. The 2nd point is that one should always look for focal dysfunction in the setting of an encephalopathy, including frontal intermittent rhythmic delta activity. This patient was in post-ictal state; Frontal intermittent rhythmic delta activity is sometimes seen as the only manifestation of encephalopathy, interrupting normal background rhythms during the postictal state.