
56y, epilepsy, MRI normal, high functioning
Jun 05, 2025What do you make of this apiculate wave in the early hours of the morning (01h26)?
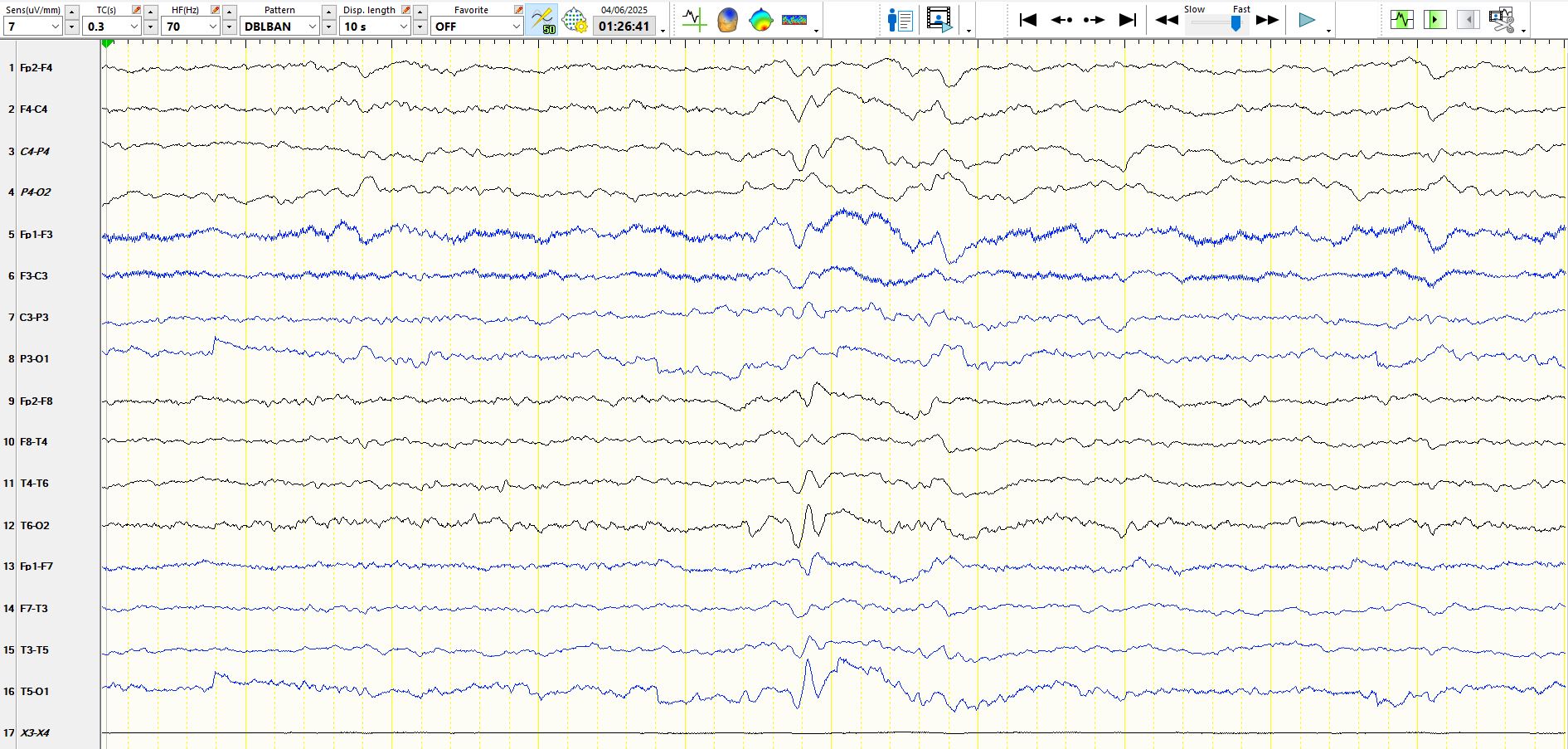
In the above bipolar montage, the large deflection in channels 12 and 16 can only be explained by a discharge that is either electropositive at 02 and 01 or electro-negative at T6 and T5. The latter is perhaps more likely as the discharge is electro-negative at F8 and F7 (downward deflections in channels 9 and 13. One has to consider the possibility of an electropositive discharge at O2 and 01 in addition to the electronegativity anterior to this, thereby producing a large deflection, especially as there is a subsequent delta wave in channels 12 and 16 and there is little deflection in channels 4 and 8 (the only other possibility is that the discharge is only electro-negative over the temporal regions and substantially equi-potential electronegativity in the parasagittal derivations). Notice that this waveform highlighted by the grey line is preceded by a wave form of opposite polarity in channels 12 and 16, again not in channels 4 and 8, Indicating the discharge is either primarily electropositive posteriorly or electro-negative over the anterior head regions. This is resolved by looking at other montages
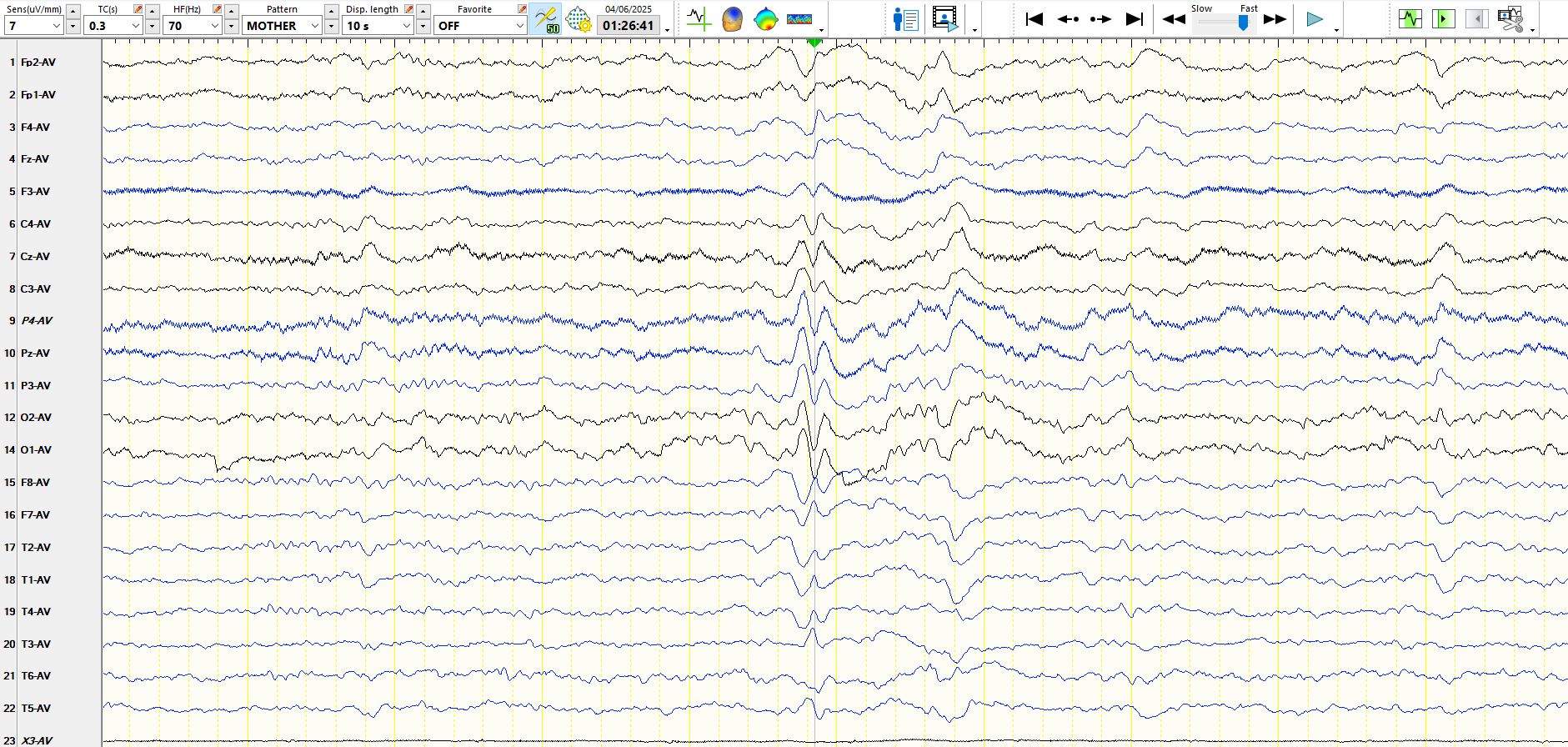
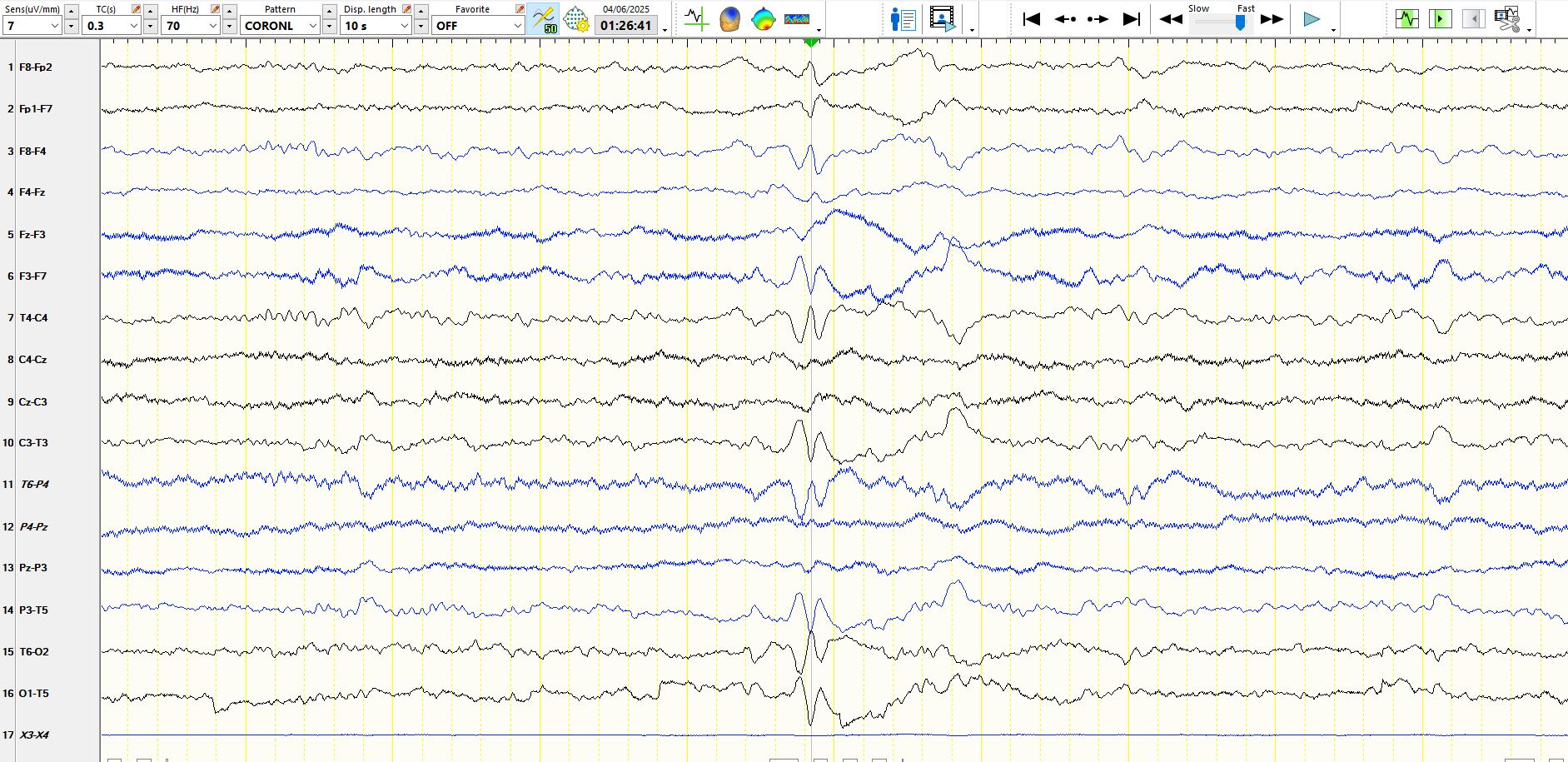
One has to be careful of the common average referential montage (above) in this situation, as the possibilities all include waveforms with a large field, which has the potential to substantially involve the referential and result in "false localisation", depending upon which references you choose to include in the common average. Hence, the coronal montage (below) should be reviewed; the grey line results in only one of 2 explanations, namely that the discharge is primarily electropositive over the sagittal and parasagittal regions or the less likely possibility that the discharge is electro-negative over the temporal regions. Notice the diminishing electro positivity as one moves anteriorly along the parasagittal derivations in the coronal montage below. This also suggests that the discharge is primarily electropositive posteriorly
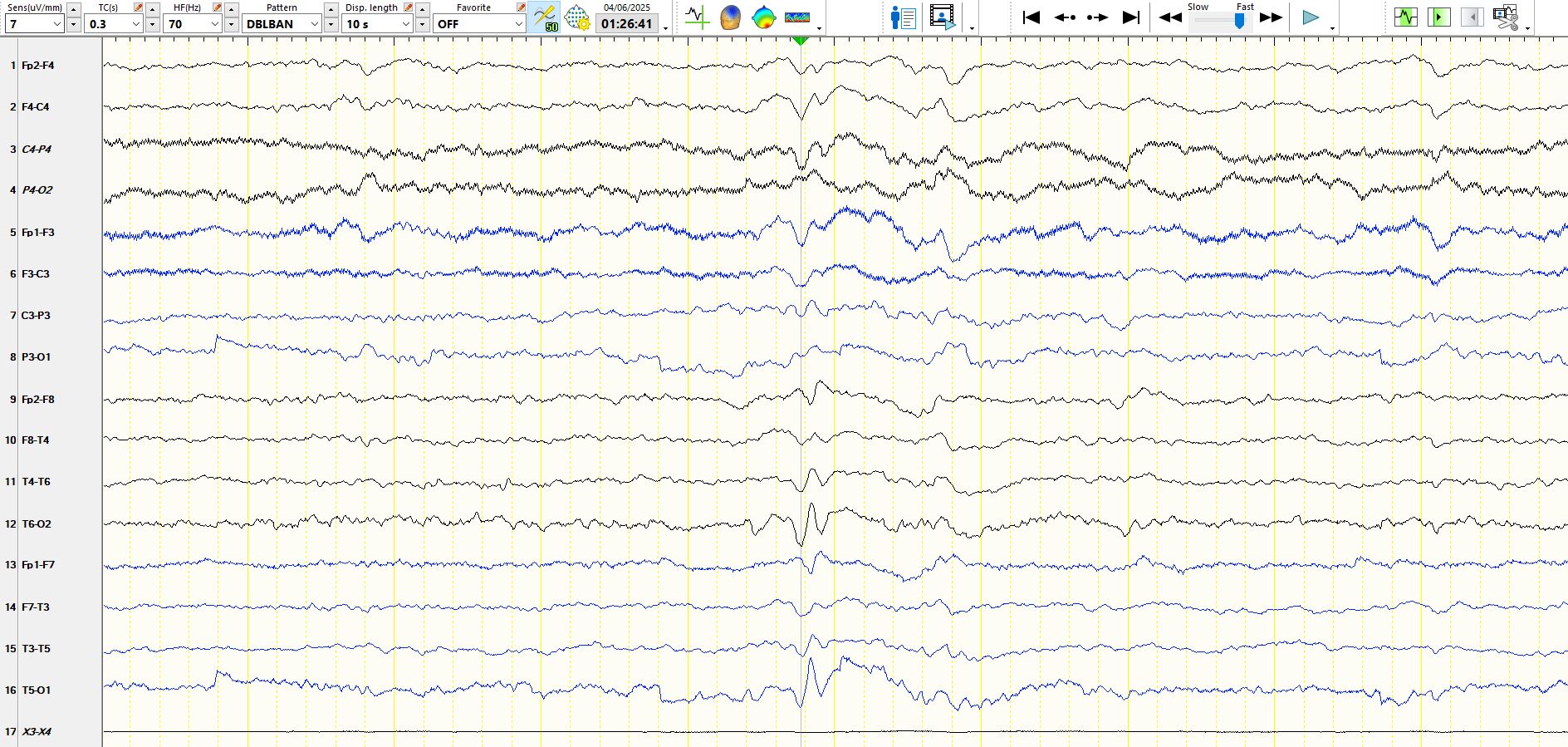
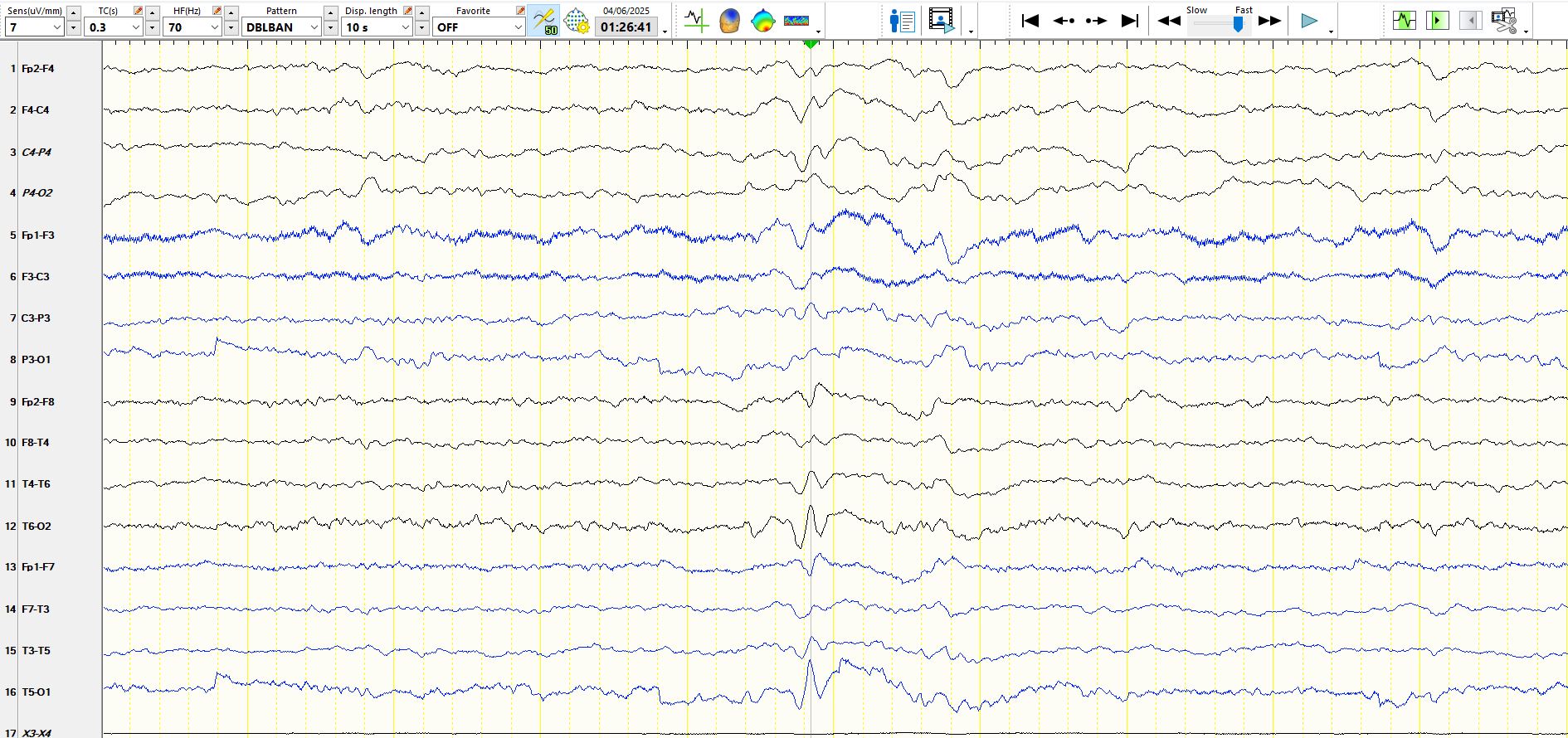
The answer becomes truly apparent when one looks at the first of these waves in the "double banana" montage above. The first possibility is that the discharge is primarily electro-negative over the posterior head regions and this possibility is further increased by the fact that the discharge is equi-potential in channels 4 and 8 (in other words equi-potential at P4 and O2 and at P3-01). Alternatively it is electropositive anteriorly. The referential montage below settles the issue
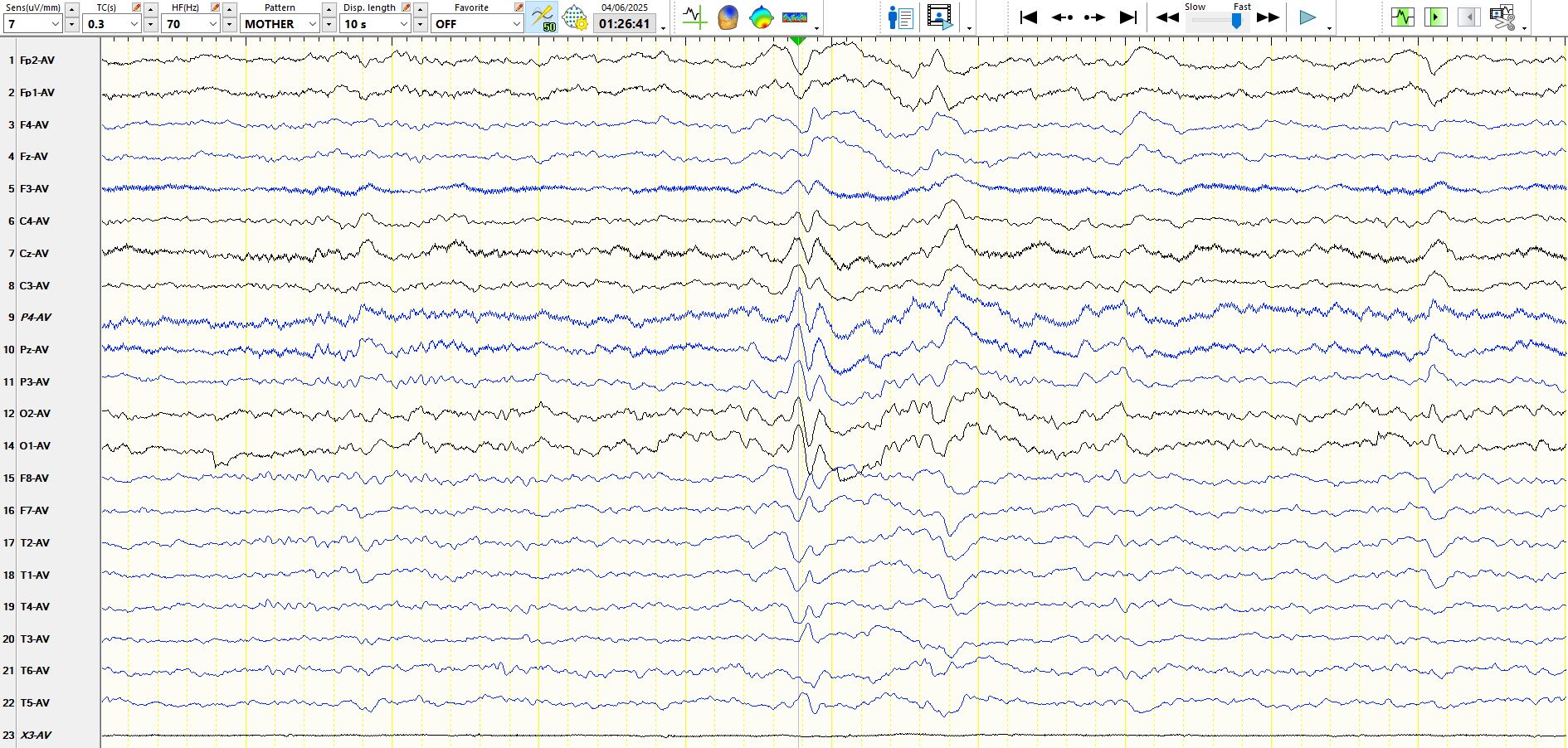
Looking at the first of these waveforms on the referential montage and fiddling with the inputs to the reference, the discharge is likely to be primarily electro-negative at PZ-P4-P3-02-01-CZ-C4-C3. In the context of sleep, this cannot be anything other than a posteriorly located V-wave. There is no such term as P-wave in the brain (to my knowledge), but if you remember it in this manner, you will know what it is next time you encounter it.