
53, likely TLE. Which of these waves is abnormal?
May 20, 2025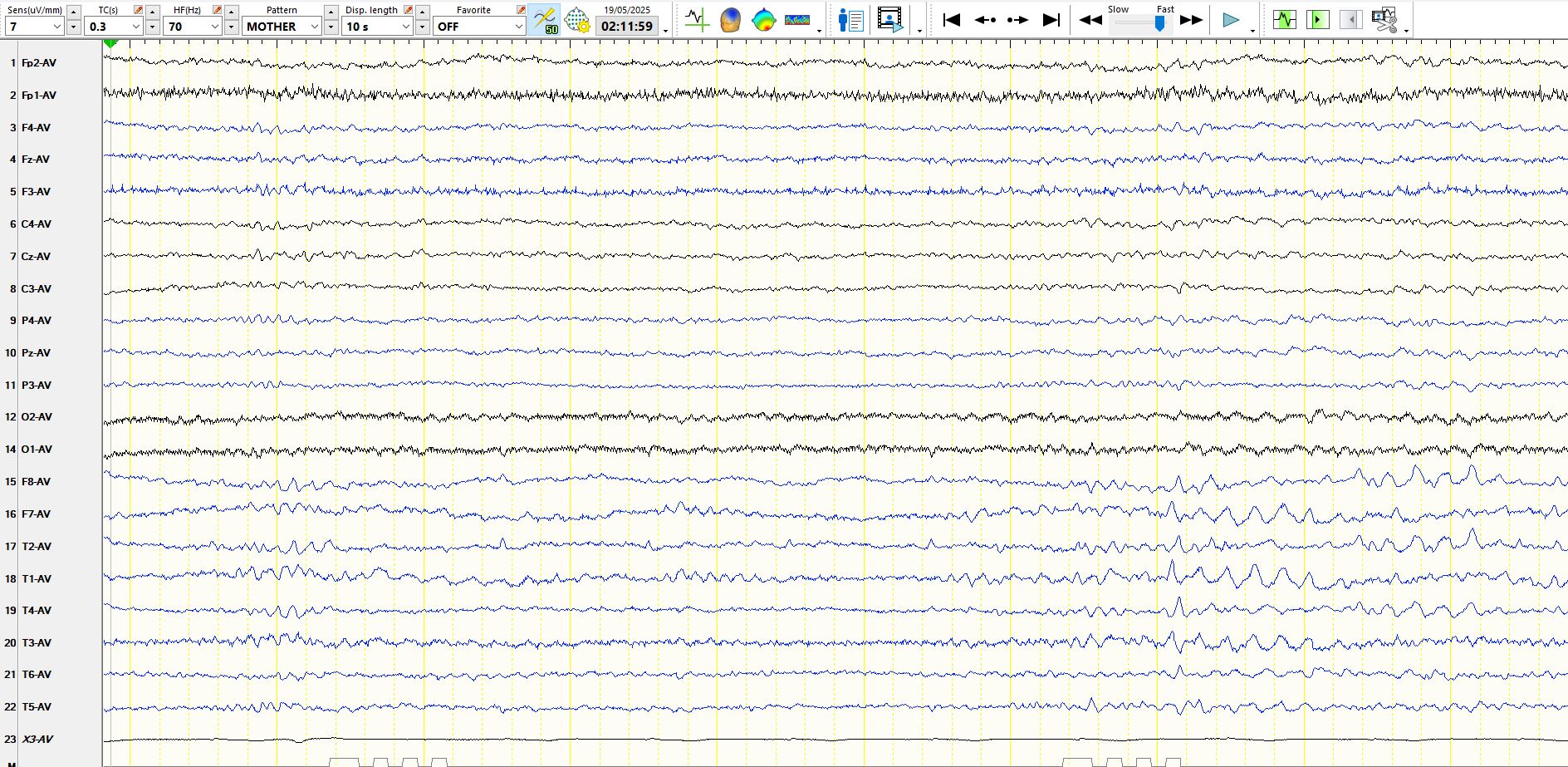
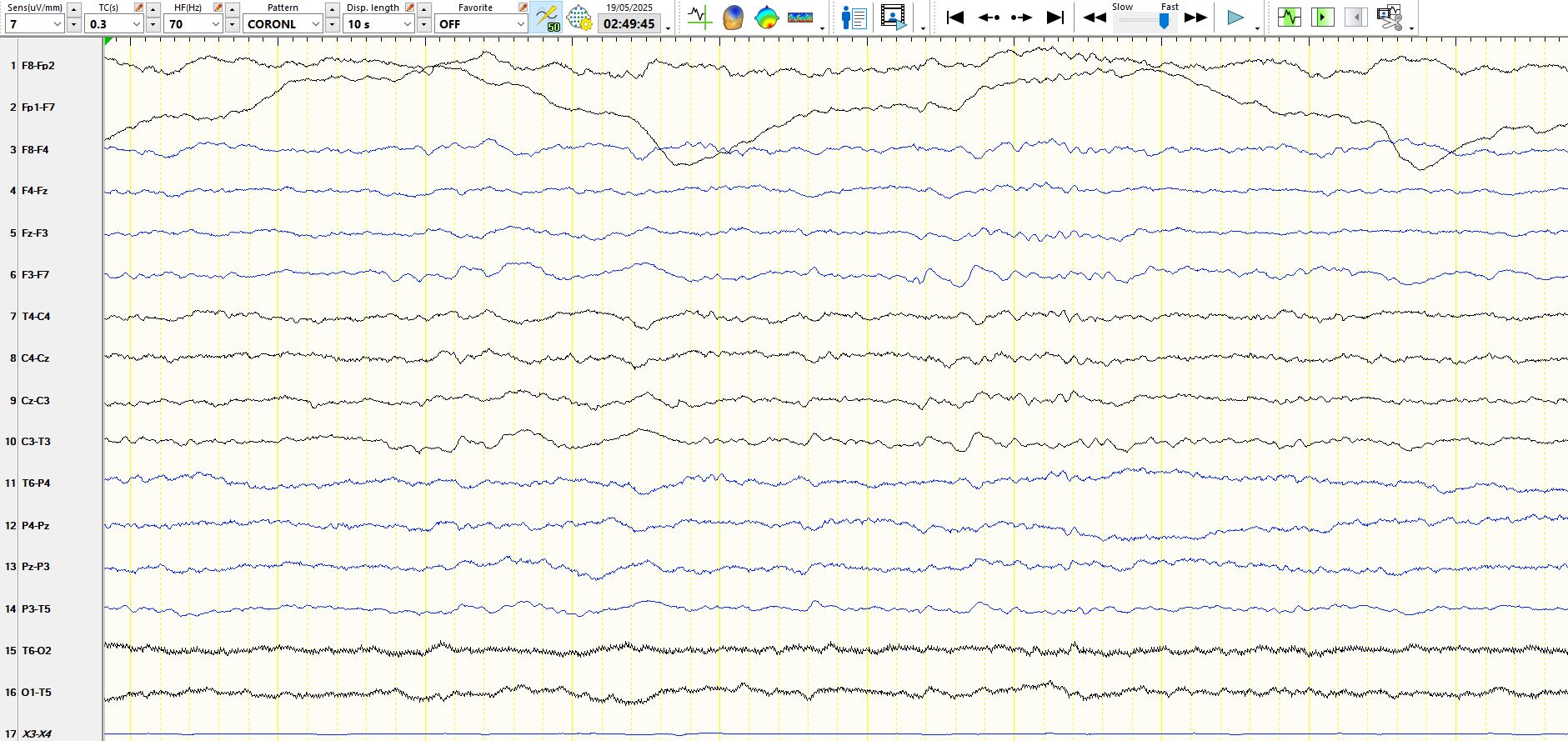
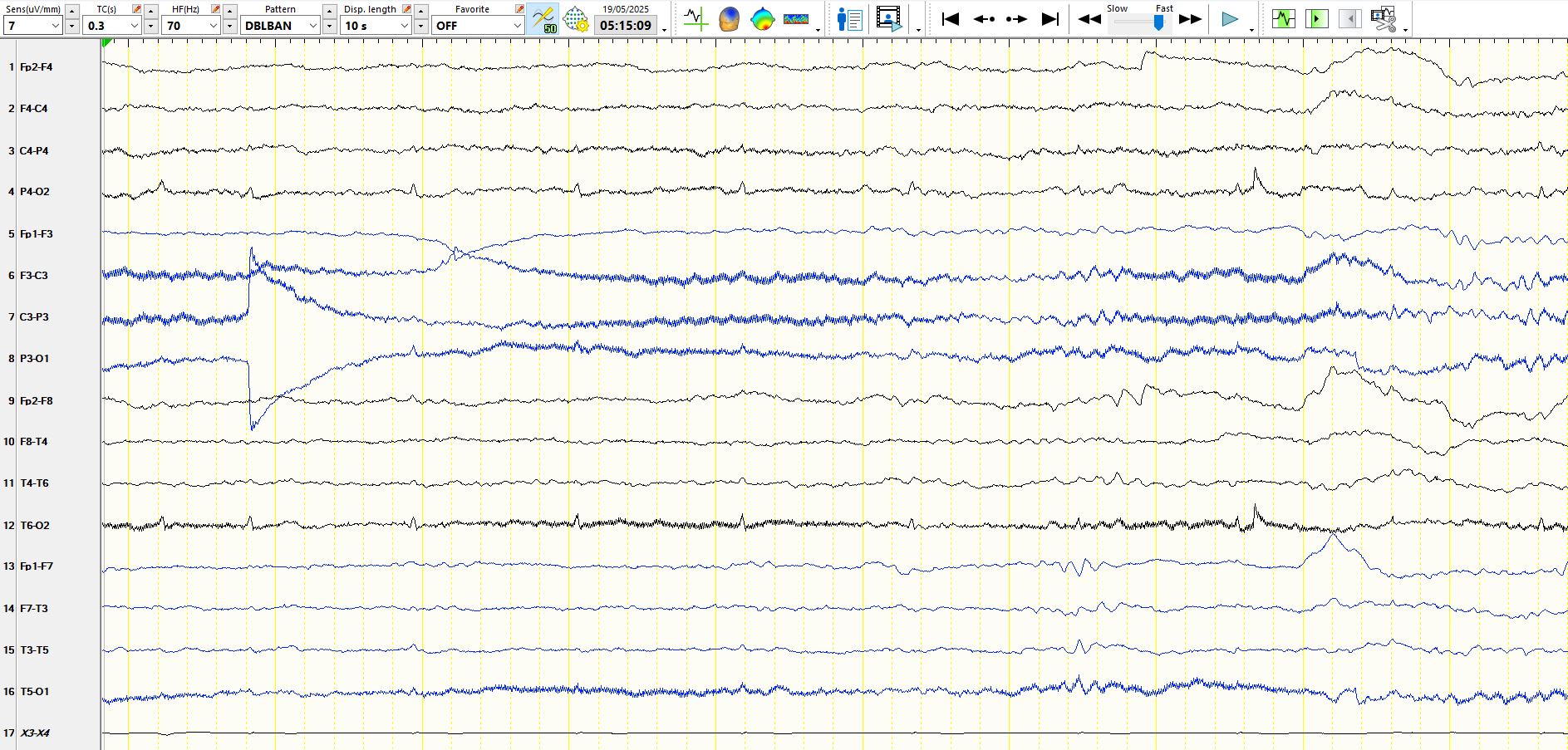
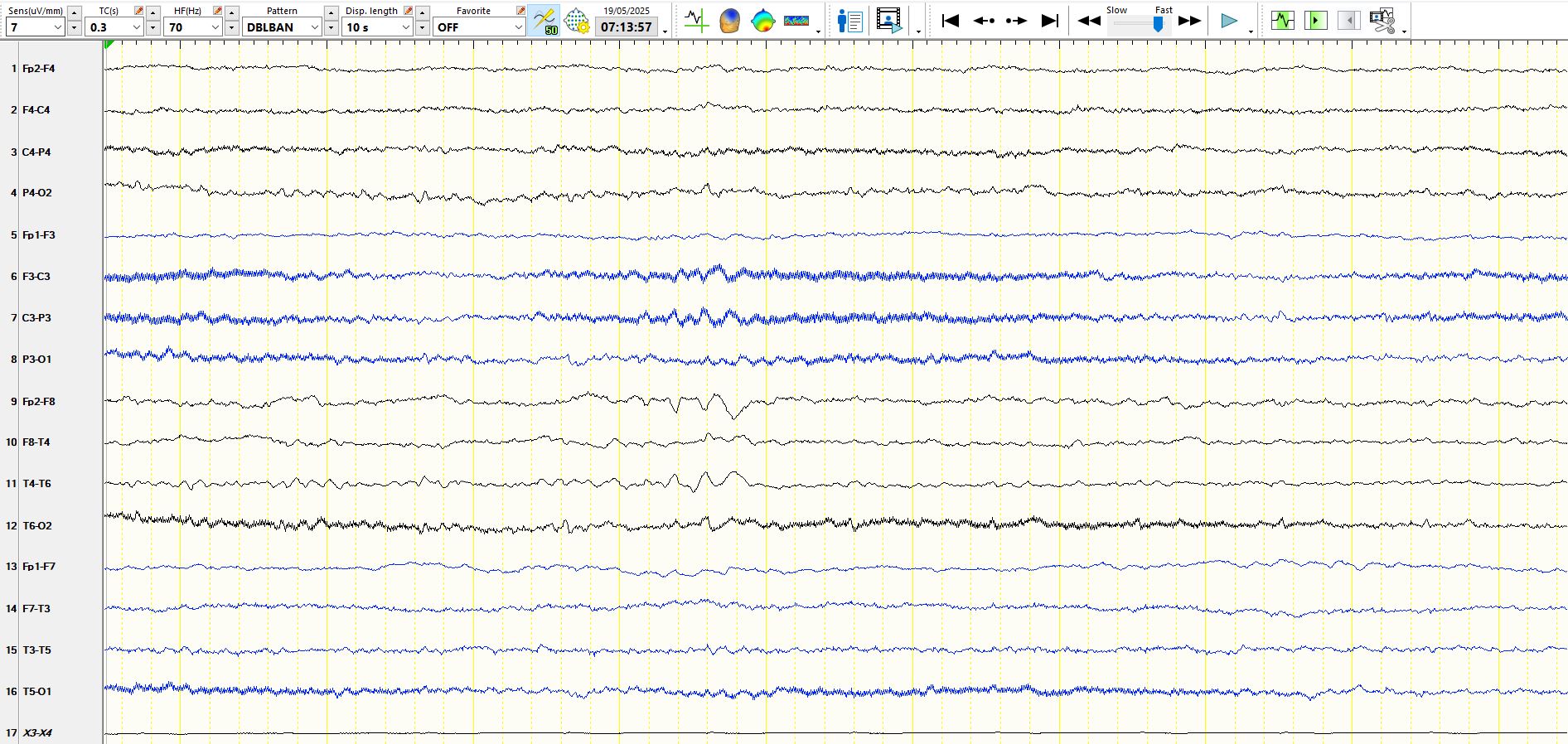
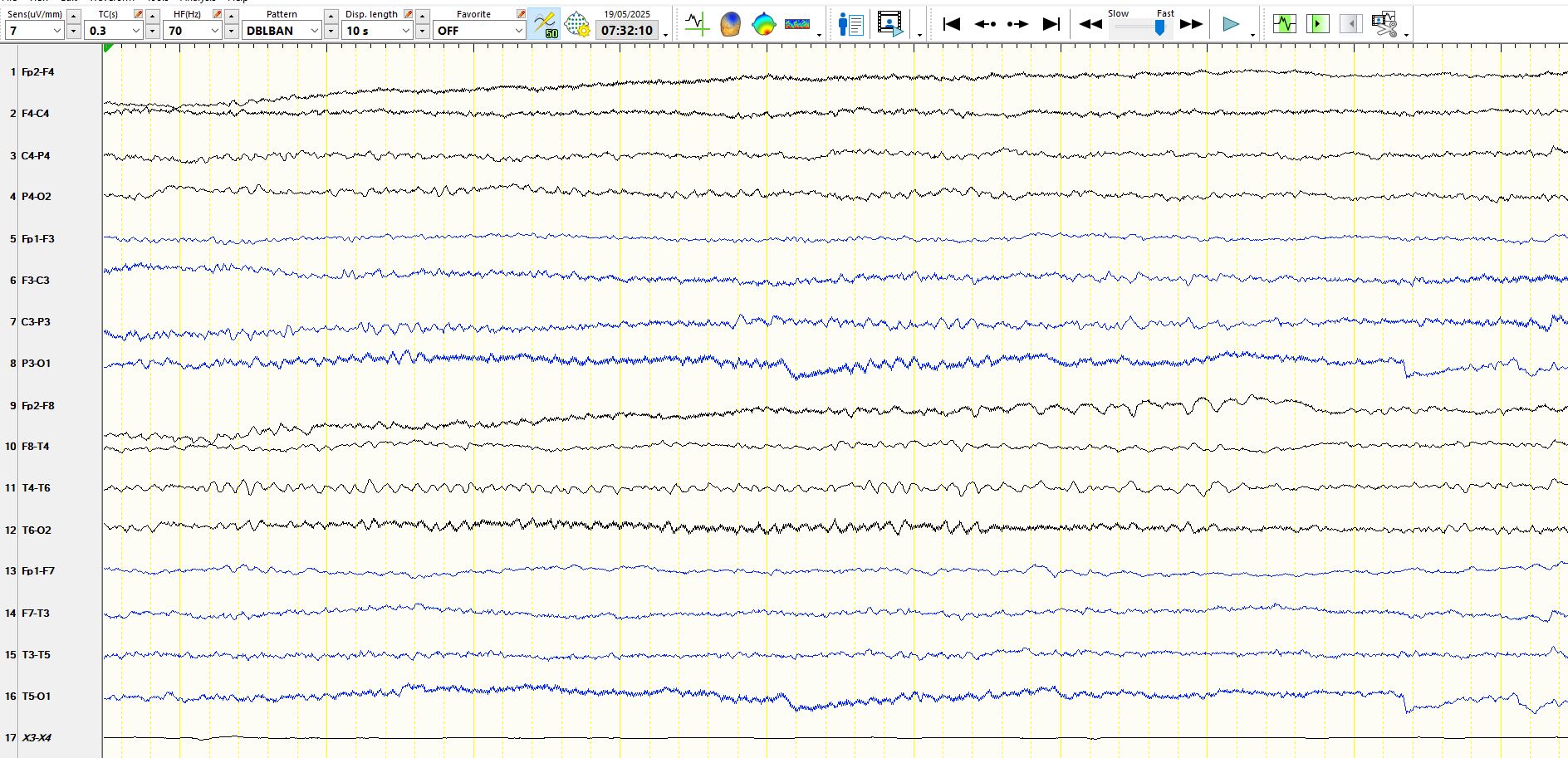
Notice that there are slow eye movements at F8 and F7 In the first few seconds, the background rhythms slow after one second and rhythmic theta waves appear alternately over both temporal regions. One might call this rhythmic anterior temporal theta of drowsiness "RATD" (not a textbook term, my term). The morphology is identical to rhythmic mid-temporal theta of drowsiness. This is a normal phenomenon
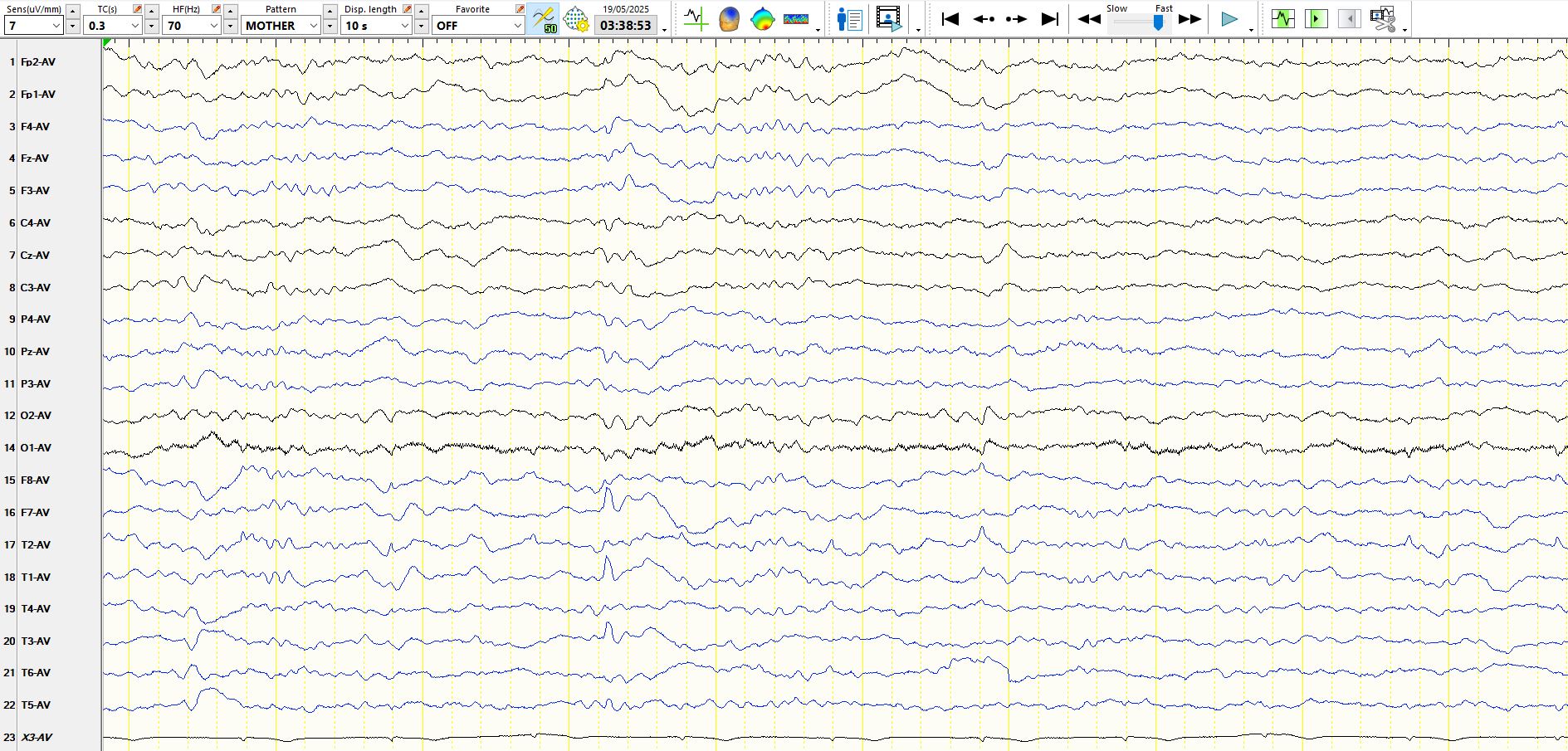
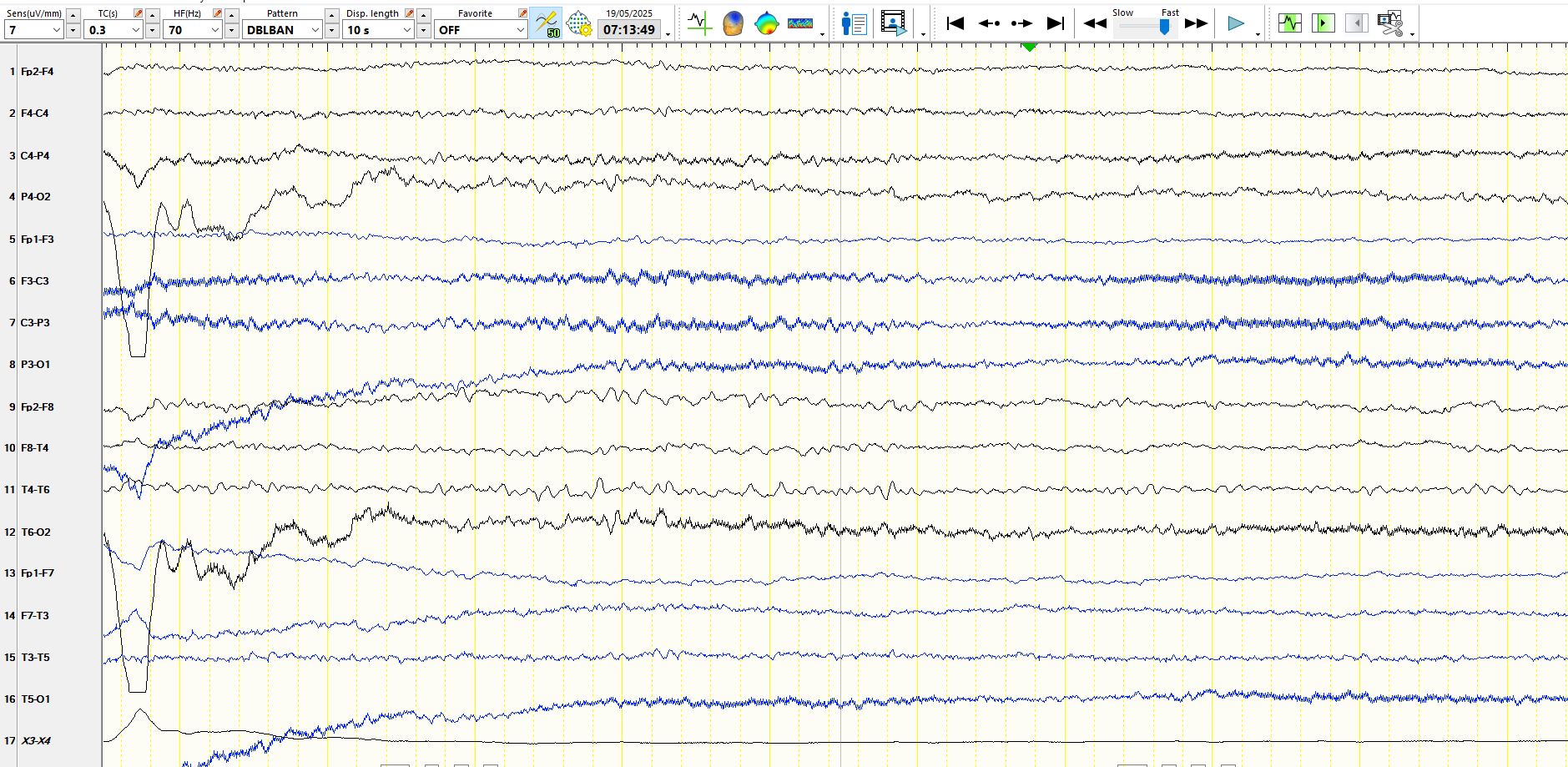
This is another example of "rhythmic anterior temporal theta of drowsiness"
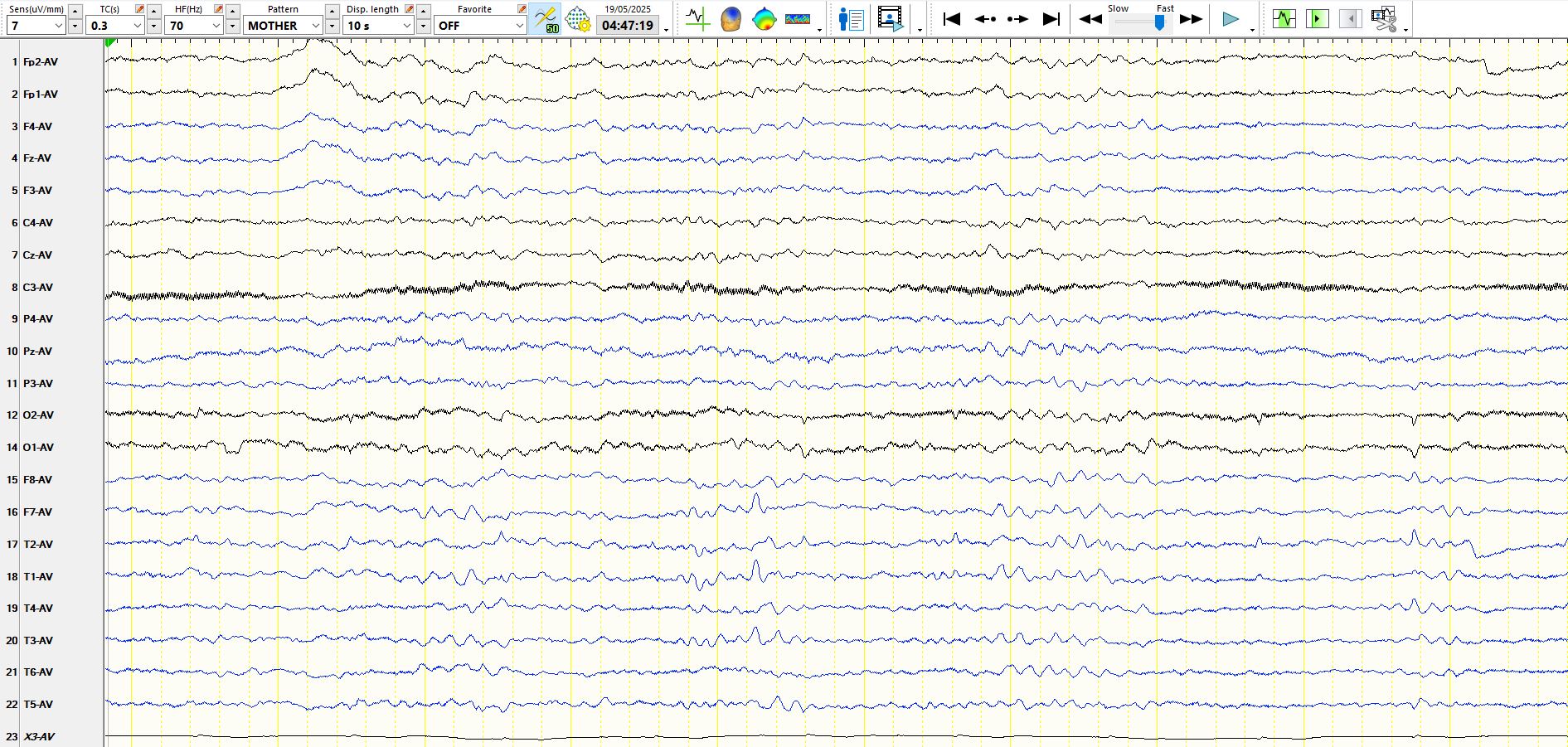
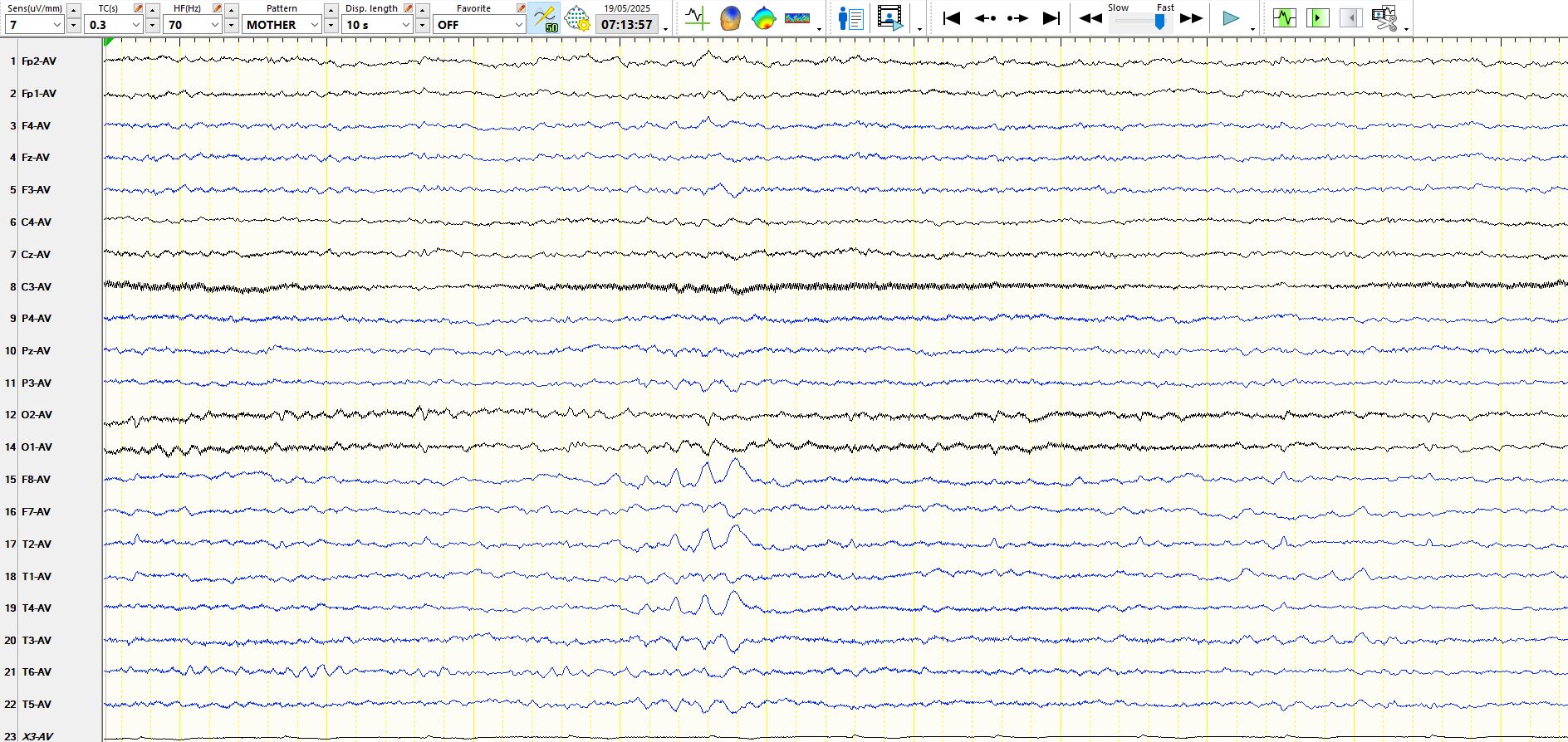
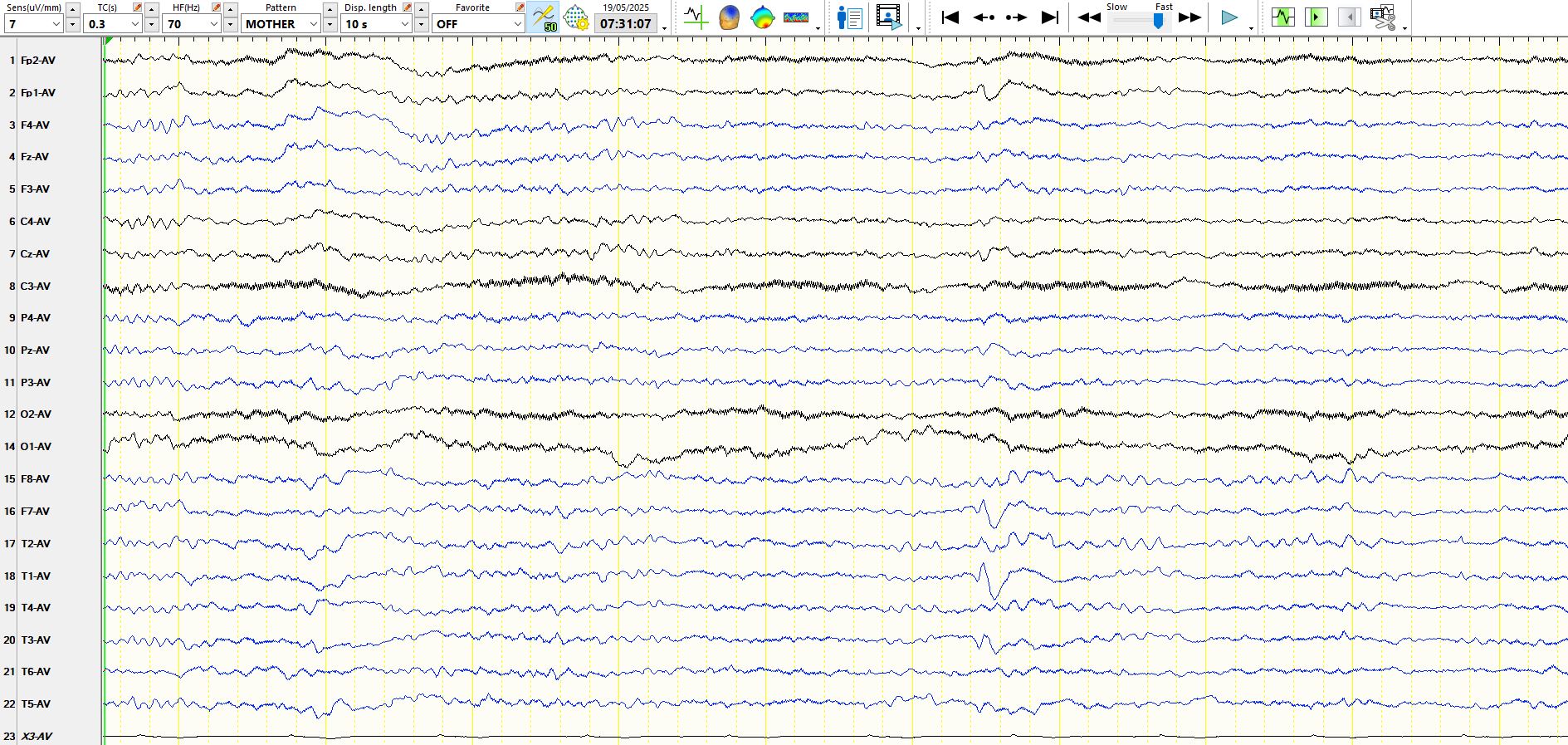
 This is a low amplitude widely-synchonous biphasic sharply contoured waveform with a large field. The slower wave that follows it is simply part of the background and hence the association is spurious. The morphology, amplitude and distribution of these waveforms in sleep mandates that they should be called small sharp spikes of sleep, a normal phenomenon.
This is a low amplitude widely-synchonous biphasic sharply contoured waveform with a large field. The slower wave that follows it is simply part of the background and hence the association is spurious. The morphology, amplitude and distribution of these waveforms in sleep mandates that they should be called small sharp spikes of sleep, a normal phenomenon.
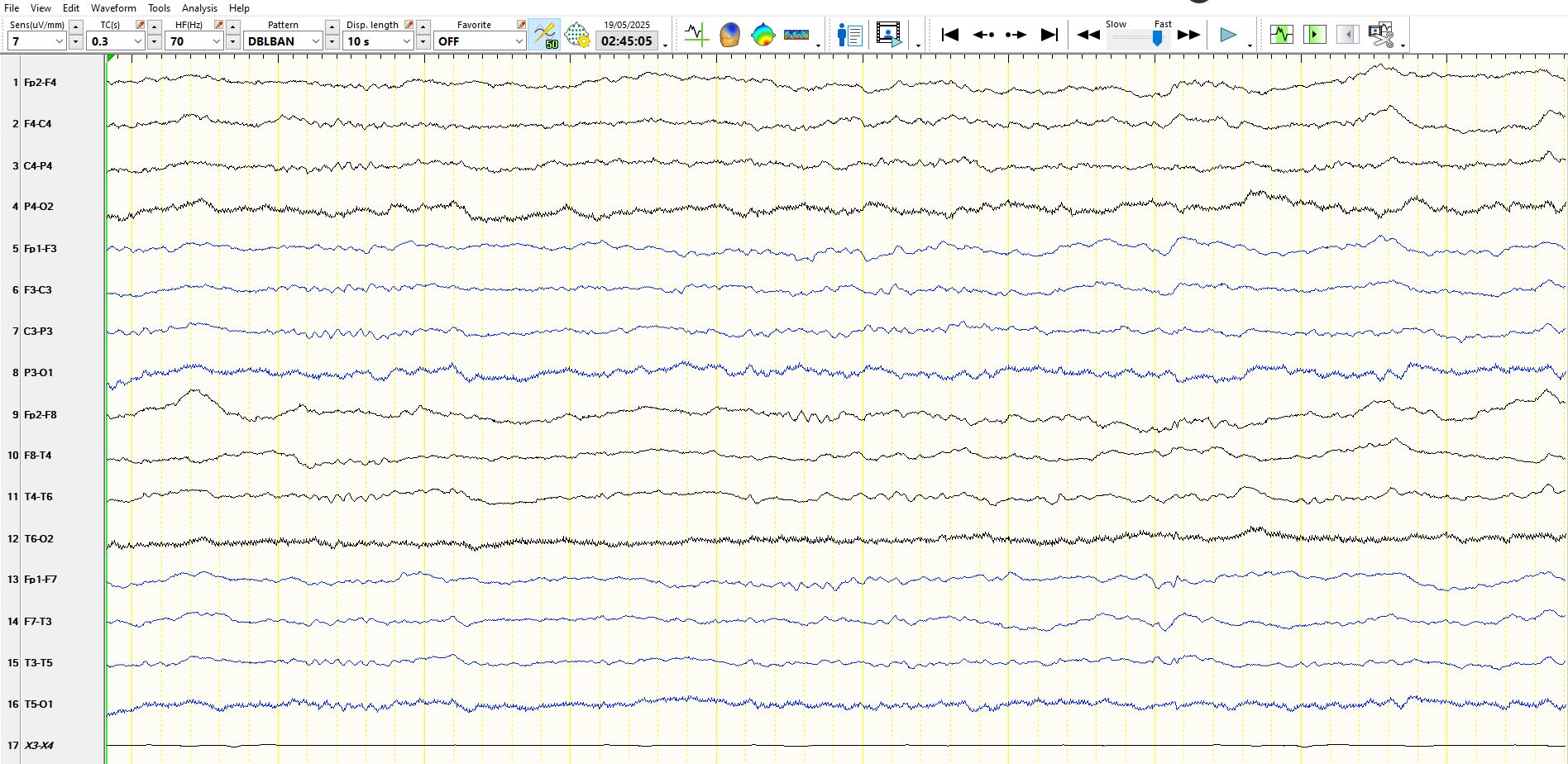
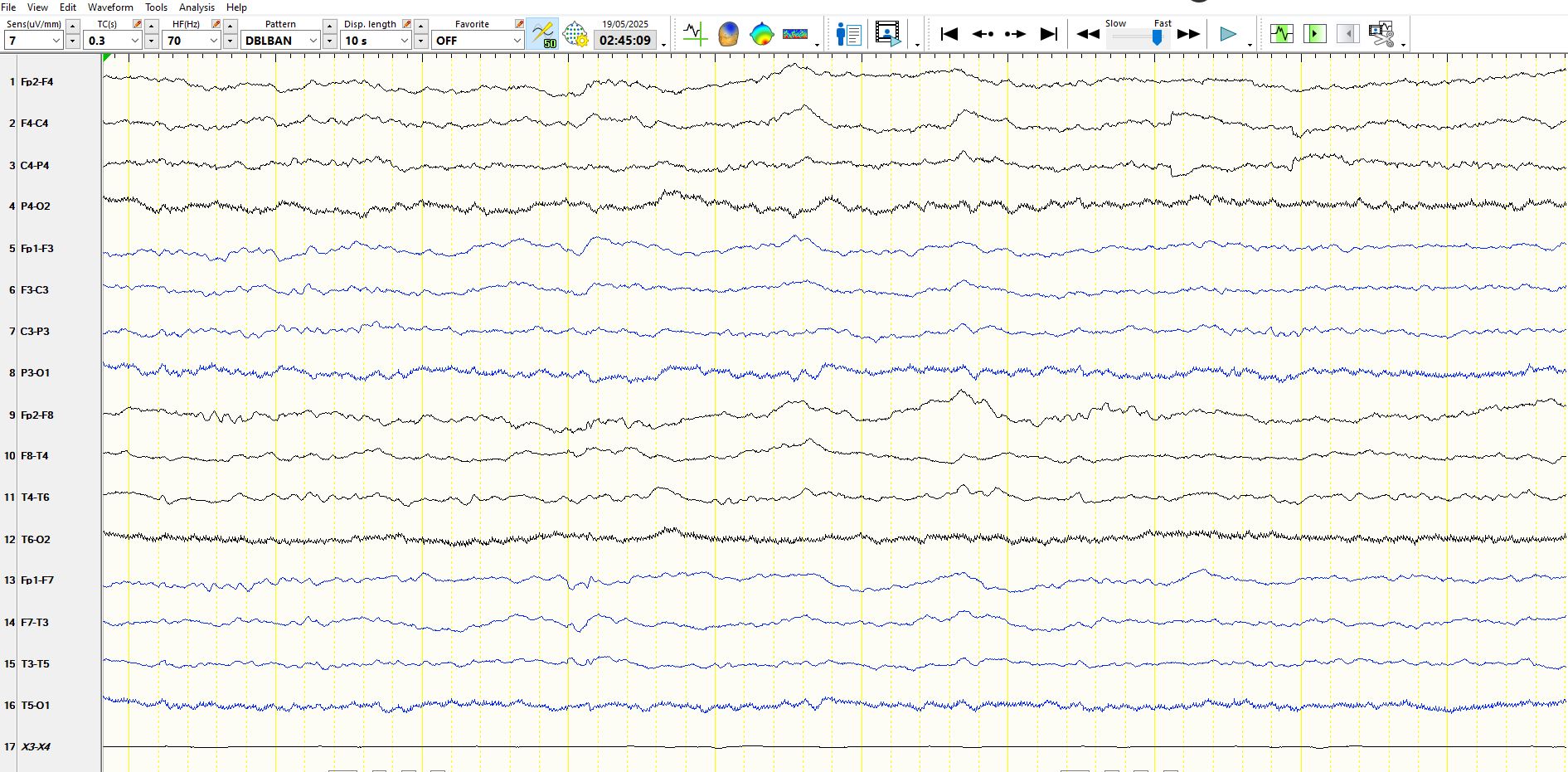
This is the same page as above, but in a bipolar montage. As is typical of small sharp spikes of sleep, the low amplitude of the apiculate wave virtually causes it to disappear on bipolar montage. Notice the "pseudo-spike-and-wave" like morphology. The lesson is to be careful of chance association and low amplitude spike-and-wave.
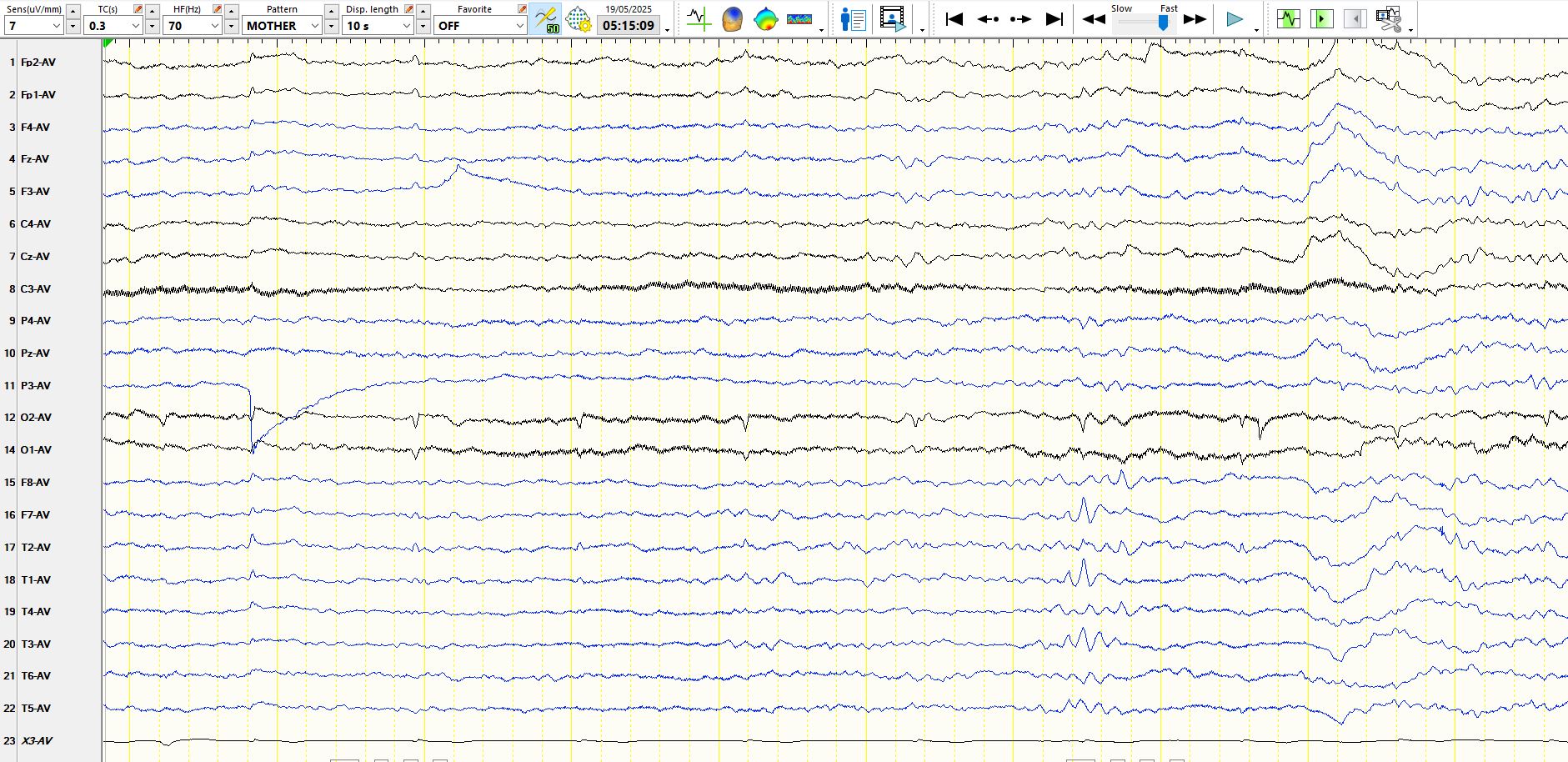
The apiculate waveforms at 2 and 6 seconds represent ECG artefact, which can wax and wane and mimic right temporal spikes. The usefulness of ECG trace is self evident.
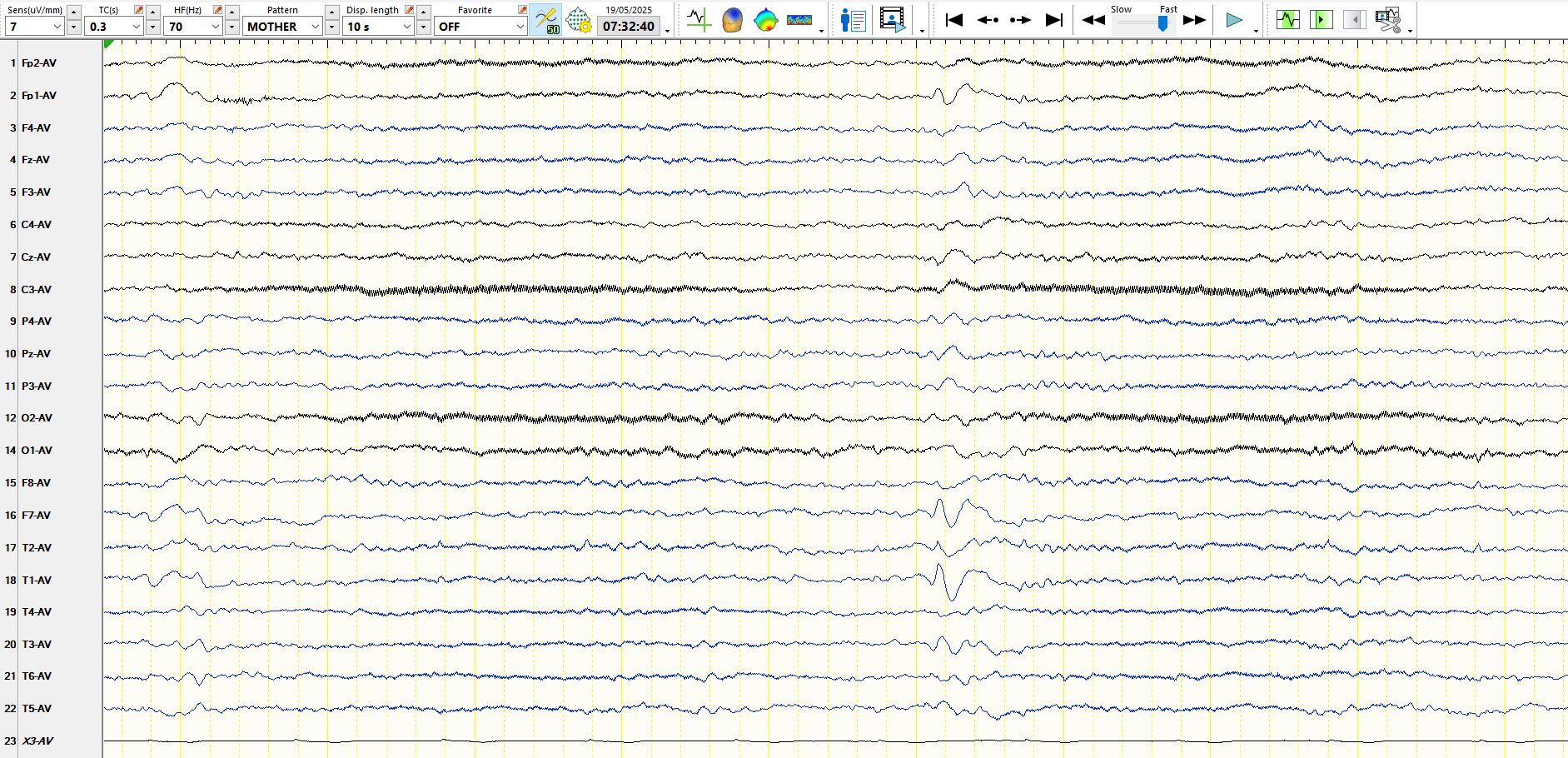
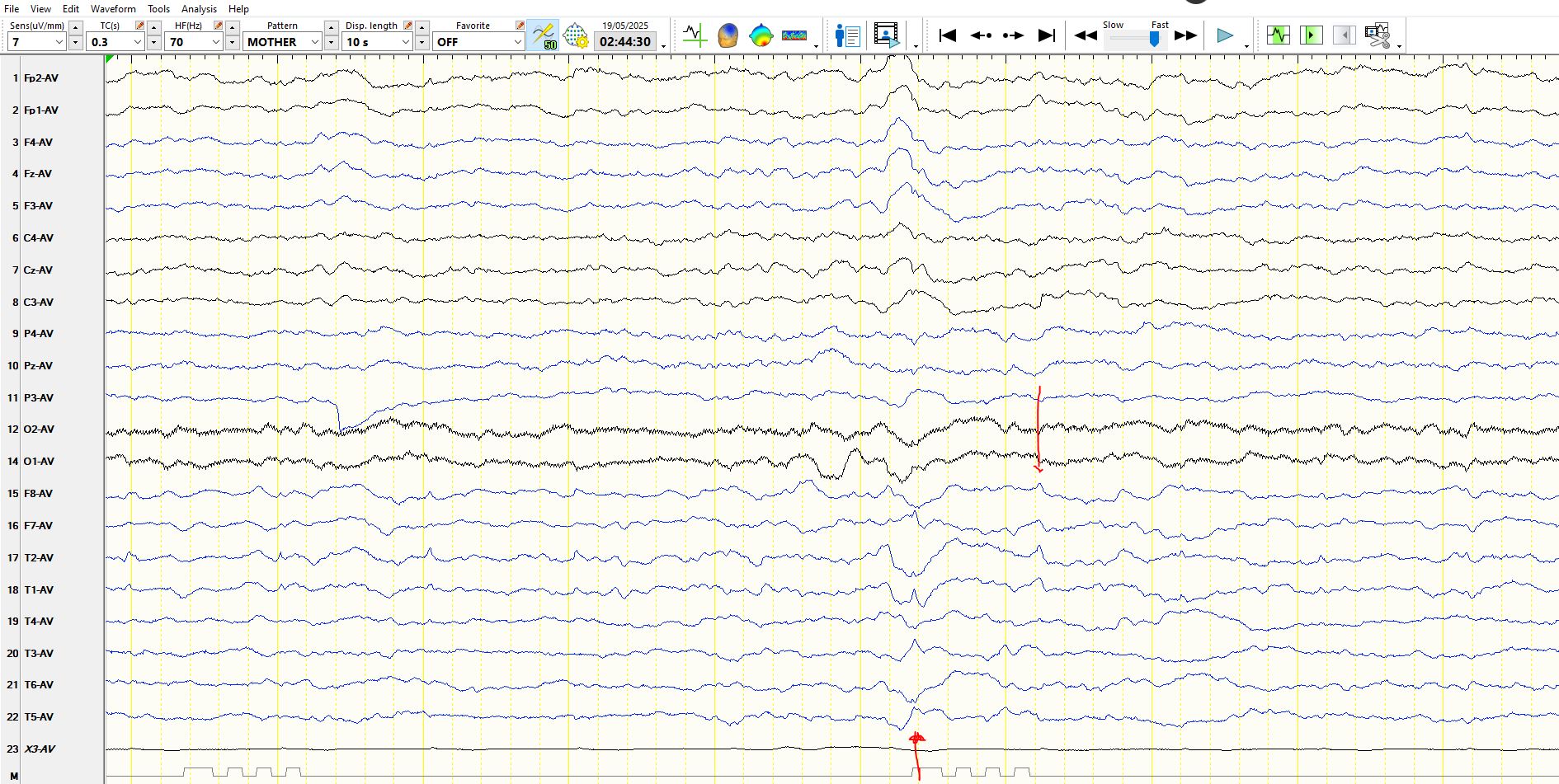 The arrowed wave on the right is once again ECG, while the arrowed wave on the left is questionably abnormal. However, since the left and right temporal derivations are "doing opposite things" and the apiculate wave is low in amplitude, do no more than note this, without calling it abnormal. This wave was barely discernible on bipolar montages.
The arrowed wave on the right is once again ECG, while the arrowed wave on the left is questionably abnormal. However, since the left and right temporal derivations are "doing opposite things" and the apiculate wave is low in amplitude, do no more than note this, without calling it abnormal. This wave was barely discernible on bipolar montages.
 Another good example of small sharp spikes of sleep.
Another good example of small sharp spikes of sleep.
The same small sharp spike of sleep represented on bipolar montage
This waveform is more suggestive of a sharp and slow-wave, as the slow-wave interrupts the background, as does the sharp wave and both are distinct from the background. Nevertheless, the waveform is low in amplitude and It may be prudent to report this as a possible or probable sharpen slower wave, to be confirmed by the presence of other waves of a similar nature or ones that are even more certain. Again, do not forego the specificity of EEG easily!
This is the same wave as above in a bipolar montage; The above cautions apply records (my suggested rule of thumb is not to consider any discharge a spike unless it is unambiguous on at least two montages, including a bipolar montage)

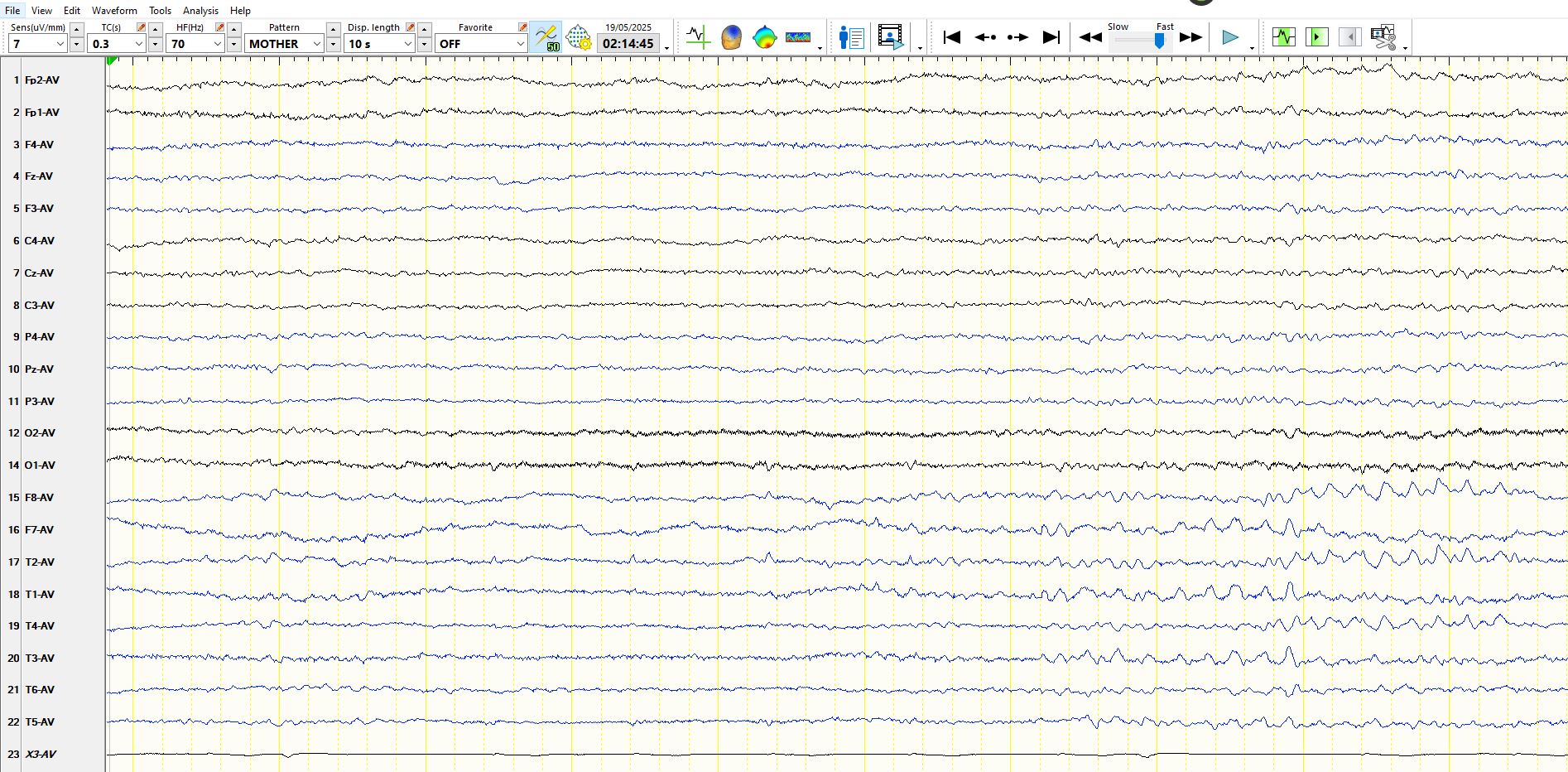
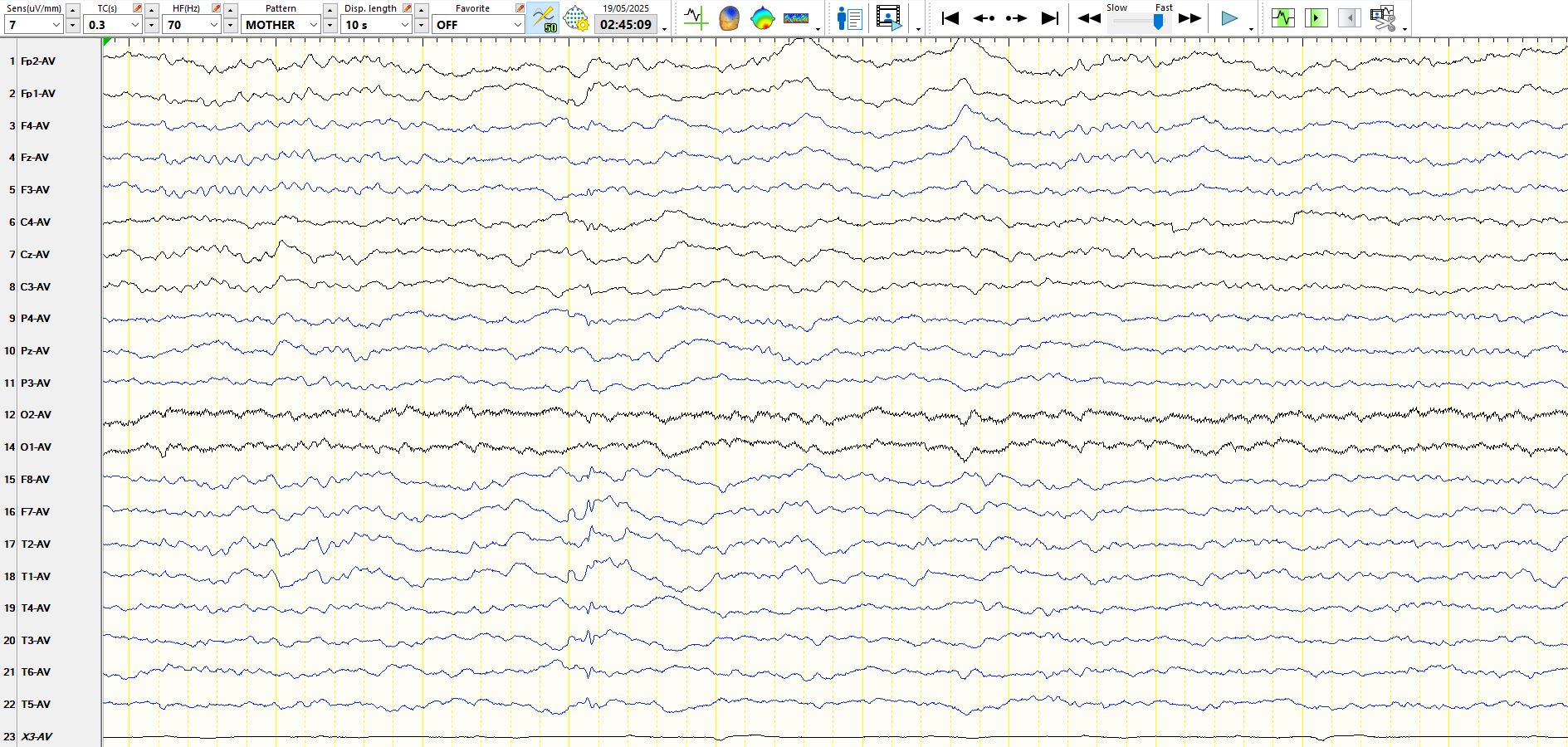
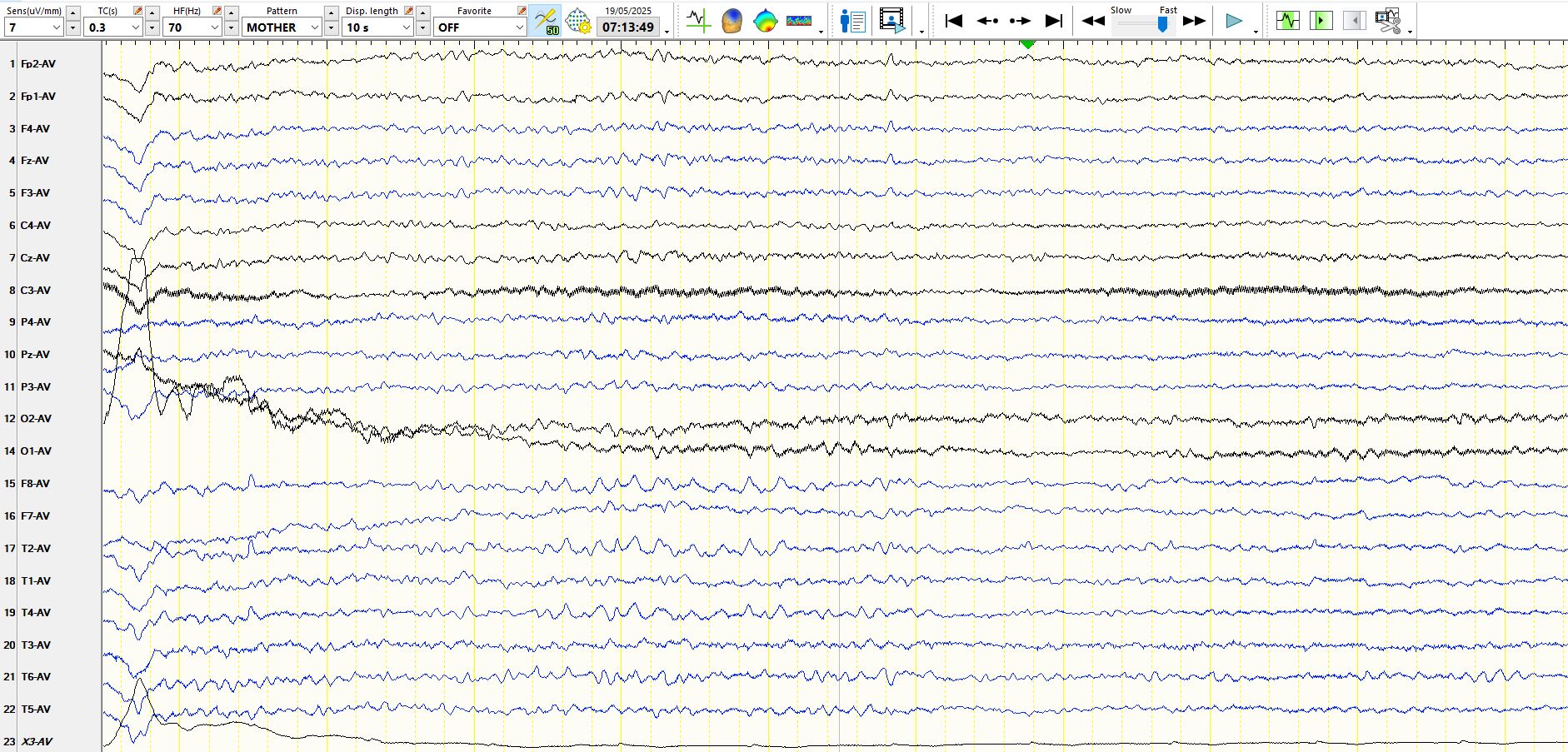
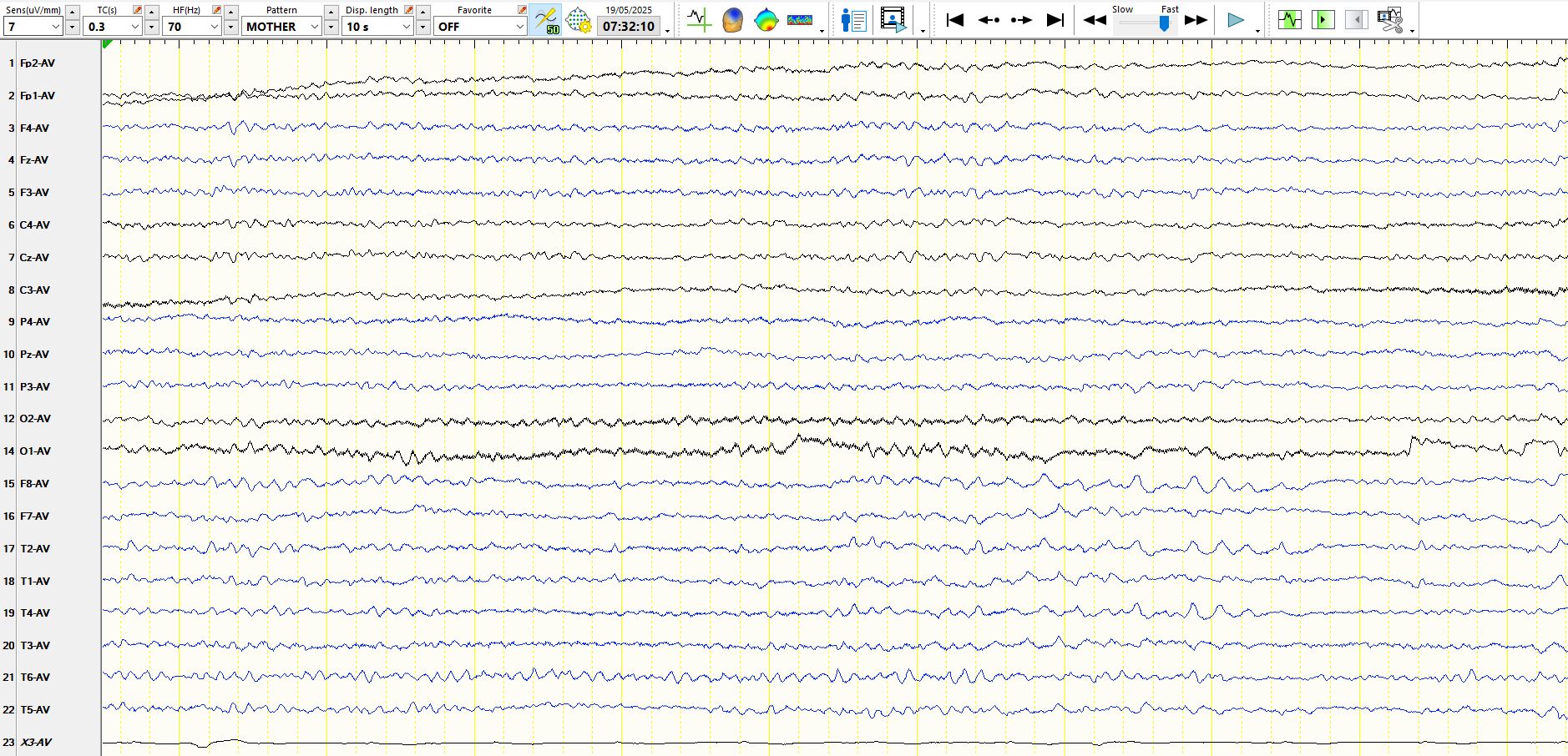
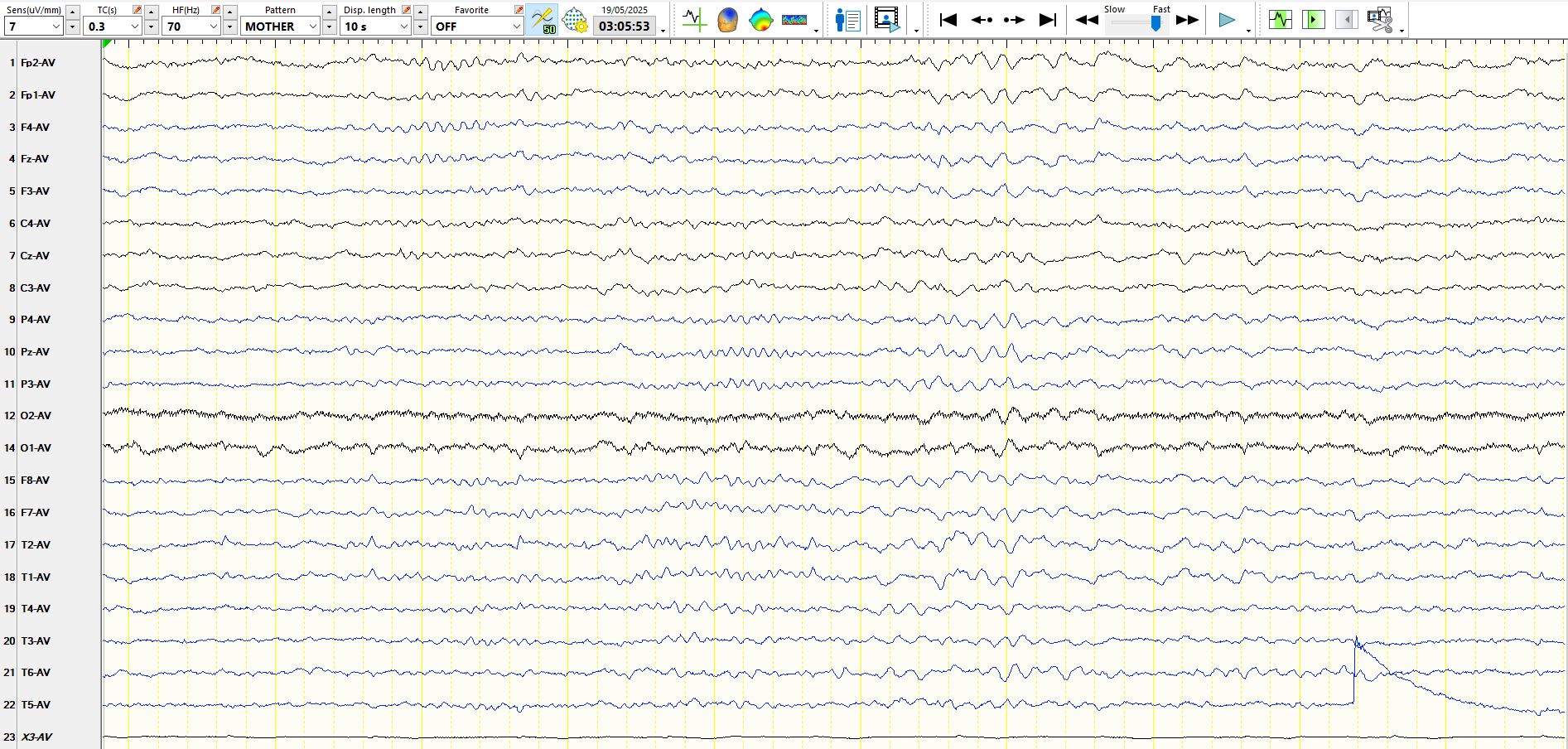
The patient is awake, with EMG artifact and faster frequencies within the first 2nd of the page. This is followed by progressive slowing of the background ribbons, cessation of EMG artifact, the appearance of slow eye movements MF8 and F7 and "rhythmic anterior temporal theta drowsiness" ("RATD"). Normal.
This is not ECG. The sharp wave at one-F7-T3 is distinct from the background and is followed by slower wave. This waveform is undoubtedly "spike-and-wave" and this finding removes doubt about the previous discharge (See above)
This is no more than a wicket wave, as it does not disturb the background, there is no following slow-wave and the waveform is not distinct from background rhythms earlier and later on the same page
This is a good example of wicket waves (normal alpha frequencies) at M1-F7-T3, during drowsiness and these waves are followed by slow waves, indicative of an evolution into stage II sleep (note the K complex on the right)
These are the same waves as above in the bipolar montage
You should recognise these now as representing rhythmic theta waves of drowsiness over the right temporal region
These are the same waveforms as above, represented on the bipolar montage
Notice the same waveforms as above, ascending in amplitude and with slight slowing at the end, Same conclusions as above
The same waveforms as above, represented on a bipolar montage
A spike that is unlike anything else in the background, followed by a slow wave, also unlike waveforms elsewhere at this time and just before and after this.
Notice the similarity of this waveform to previous spike-and-wave discharges at M1-F7. Notice also the wave in the first 2nd at M1-F7, which, on its own, one certainly could not call a definite spike-and-wave.
On this occasion the rhythmic anterior temporal theta of drowsiness appears largely on the right side
And here it is represented on the bipolar montage
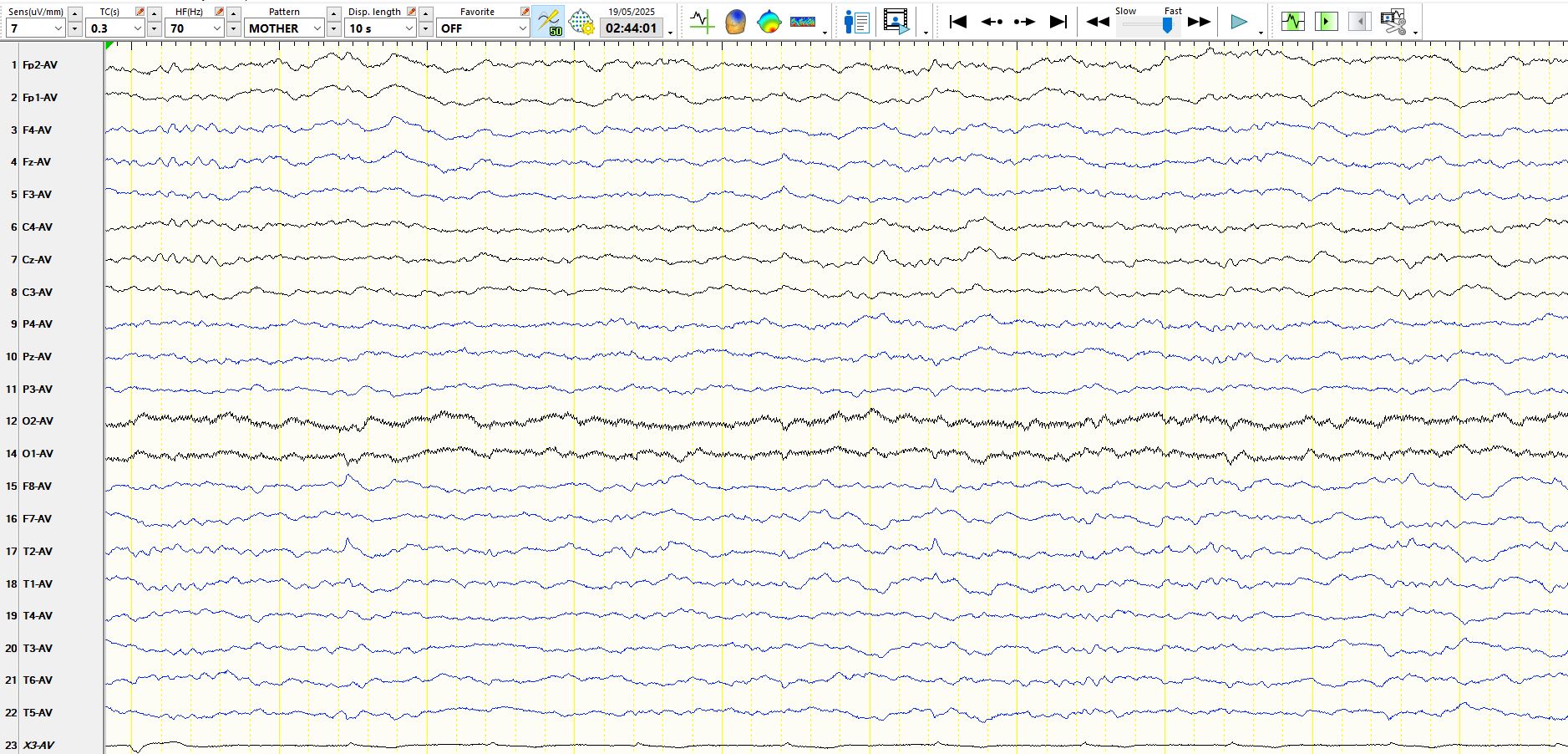
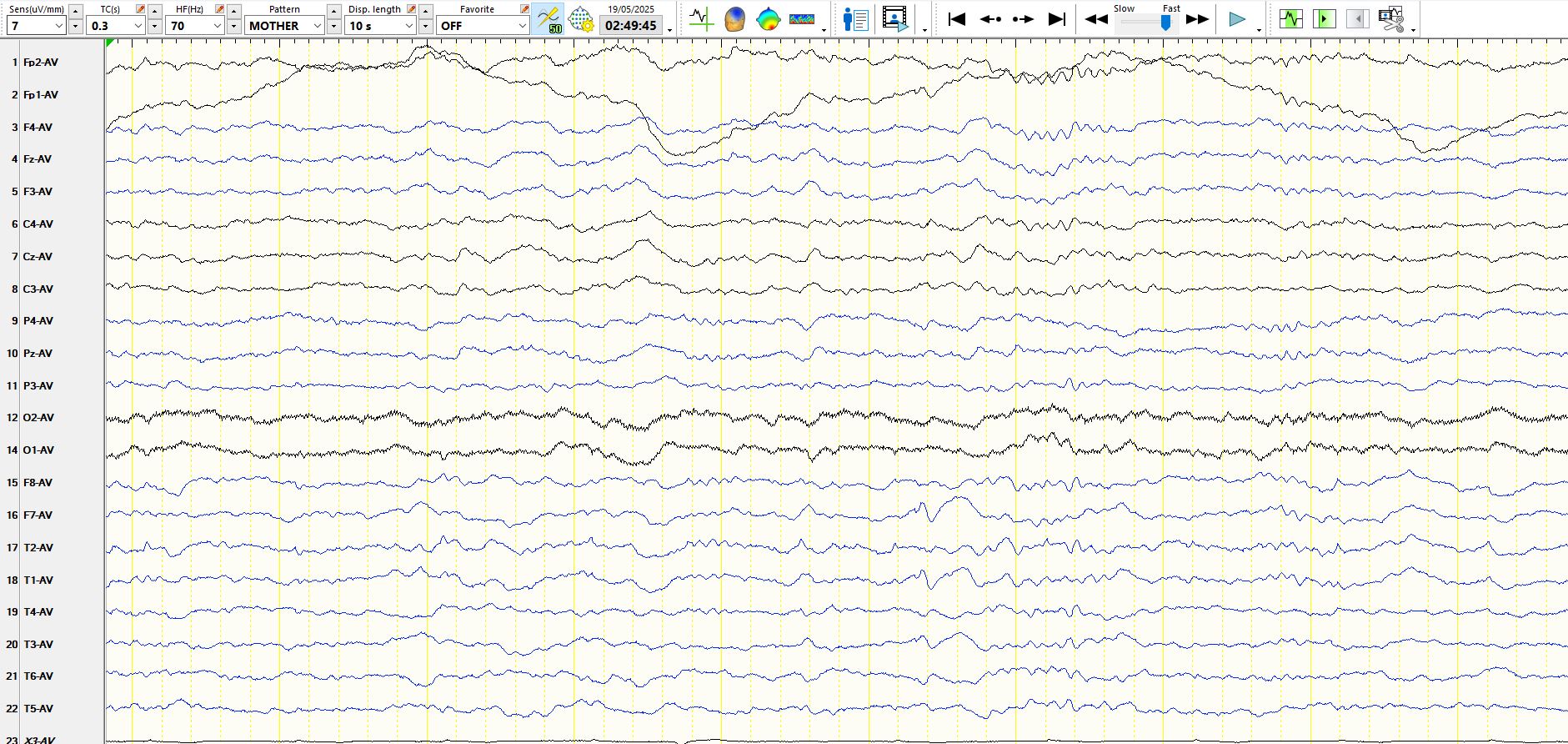
The same patient, with drowsiness manifest as the abrupt appearance off diffuse theta waves, synchronous with the disappearance of faster frequencies over the anterior and posterior head regions, and the anterior temporal regions
Bottom line?
Most sharply contoured waves in the temporal regions are normal, especially in drowsiness and sleep. Moreover, waveforms that resemble the background rhythms are normal. Hence, a single page is no way to scrutinize the background. One has to be very vigilant for the early signs of drowsiness, which is commonly seen on EEG. Don't call something a spike or a sharp wave until it is completely unambiguous; or else you run the risk that your EEG interpretation loses its specificity for the diagnosis of epilepsy, which is the most dreadful outcome of EEG interpretation.