41y, TLE
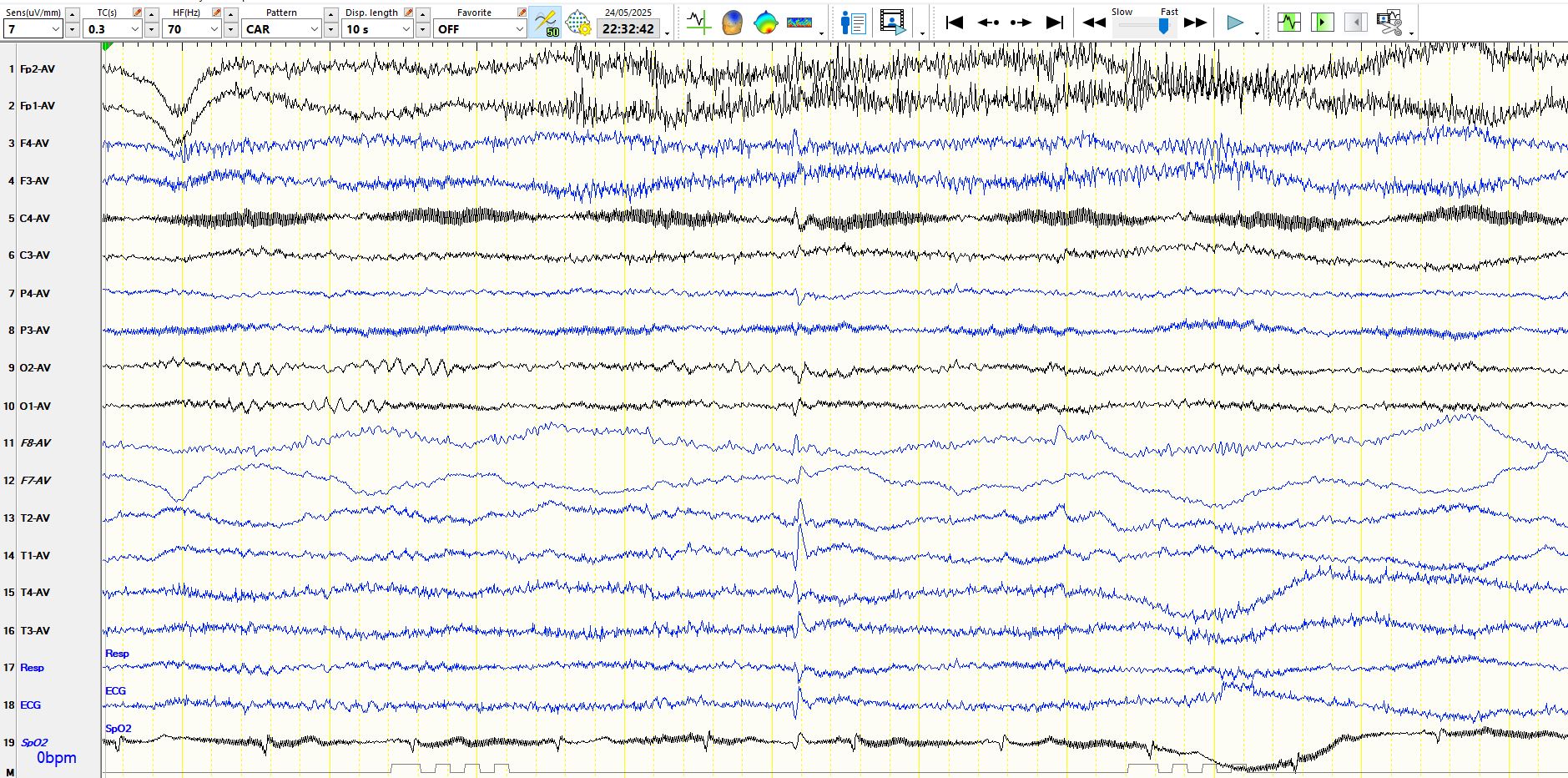
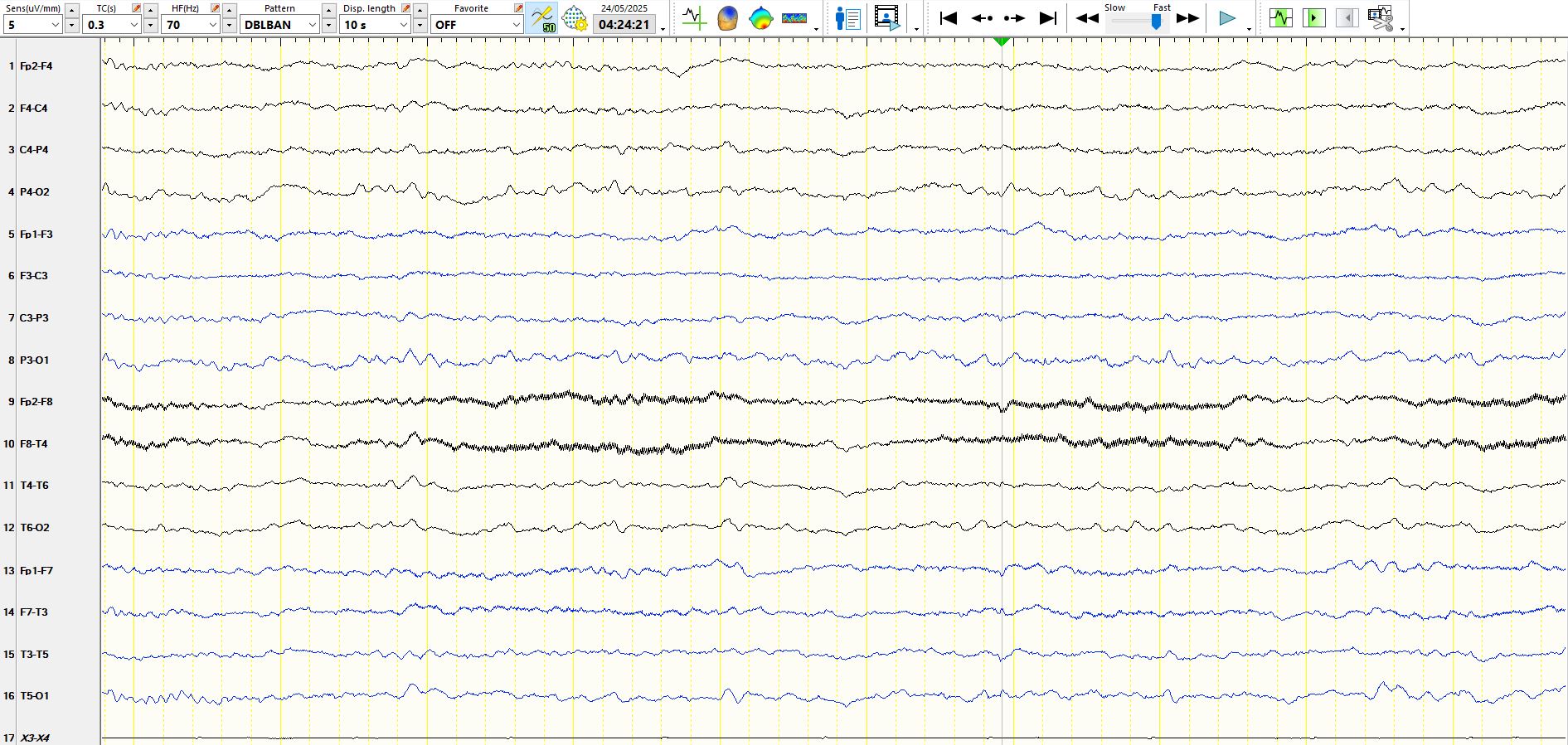
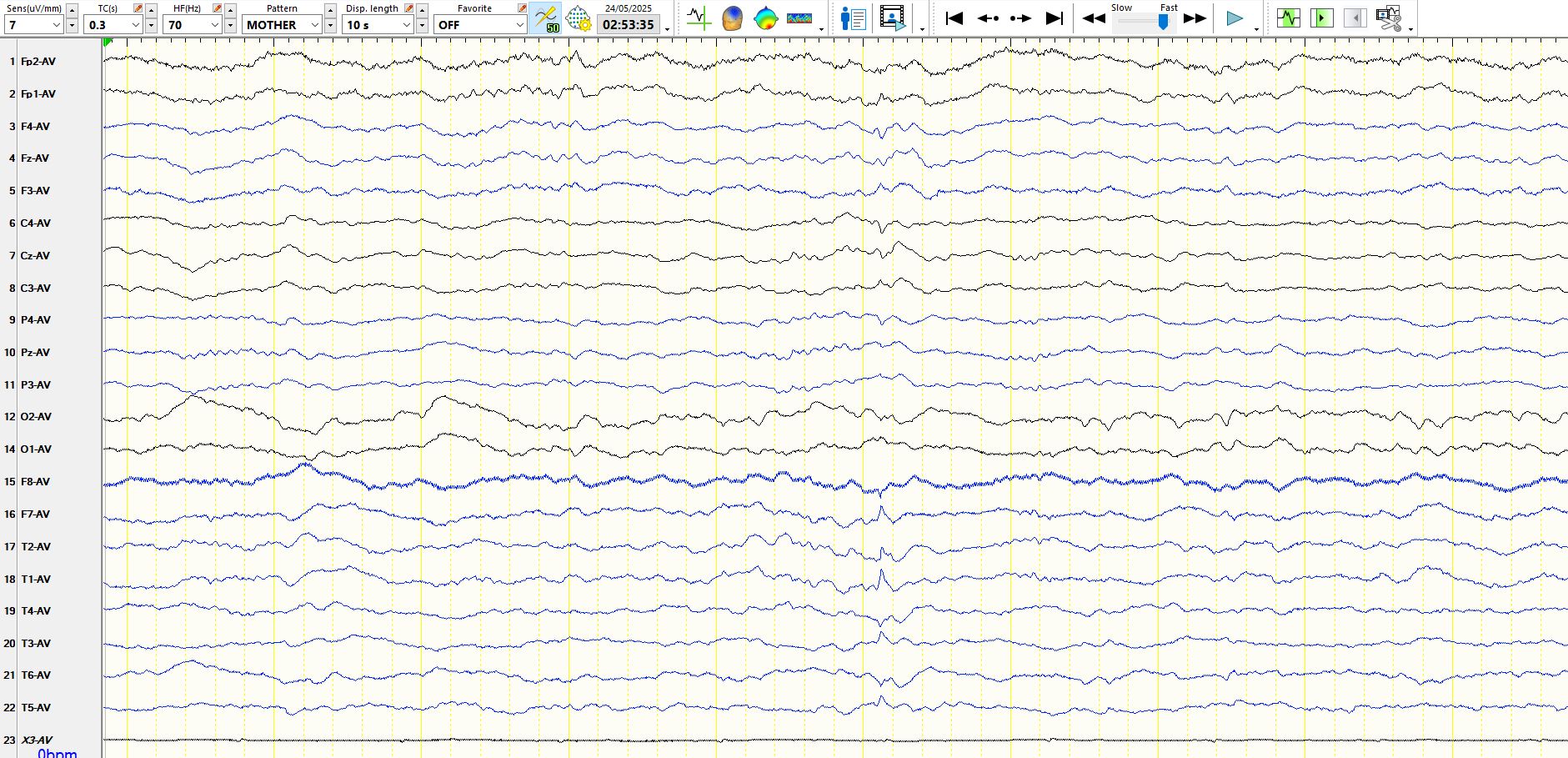
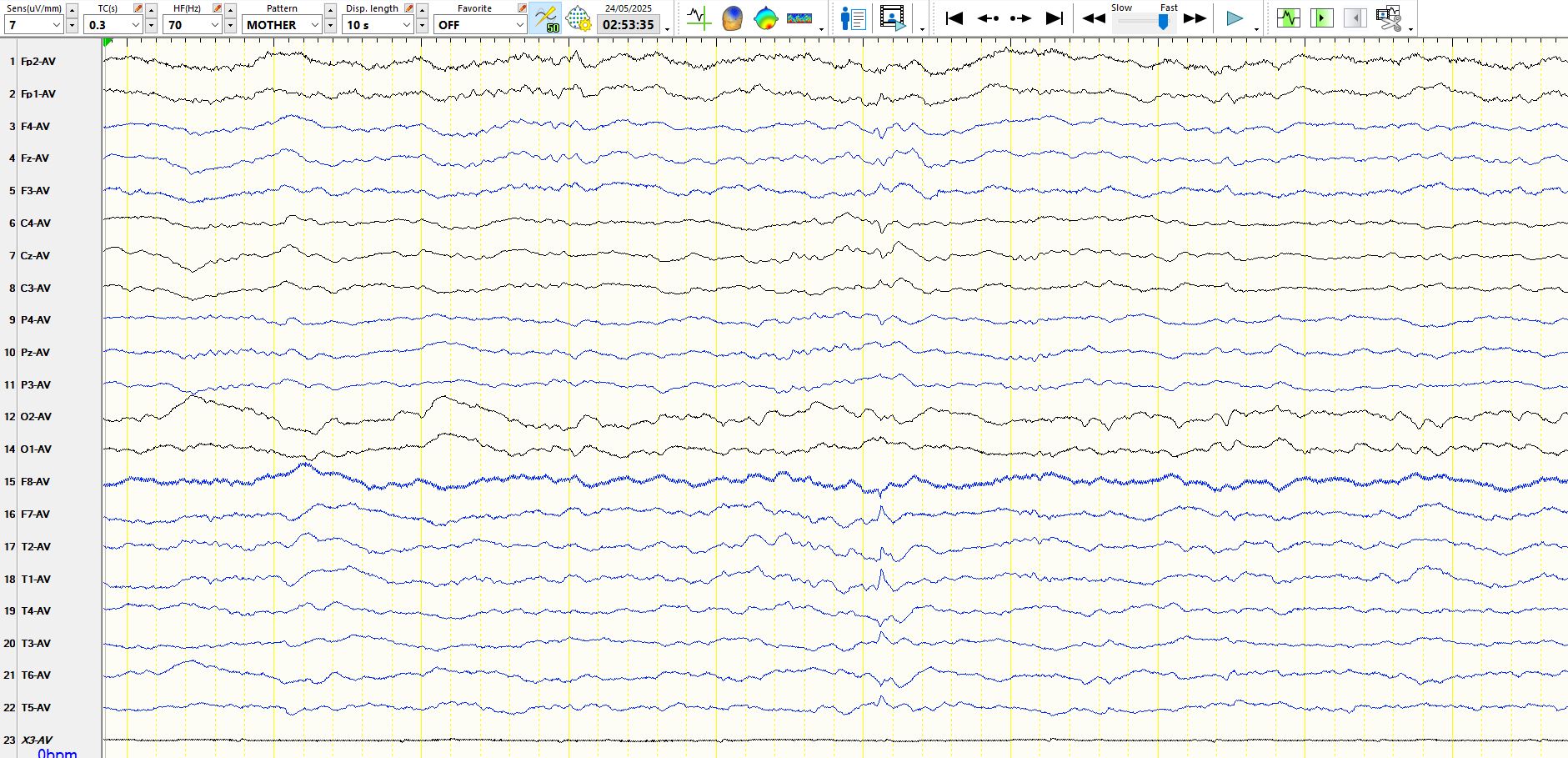
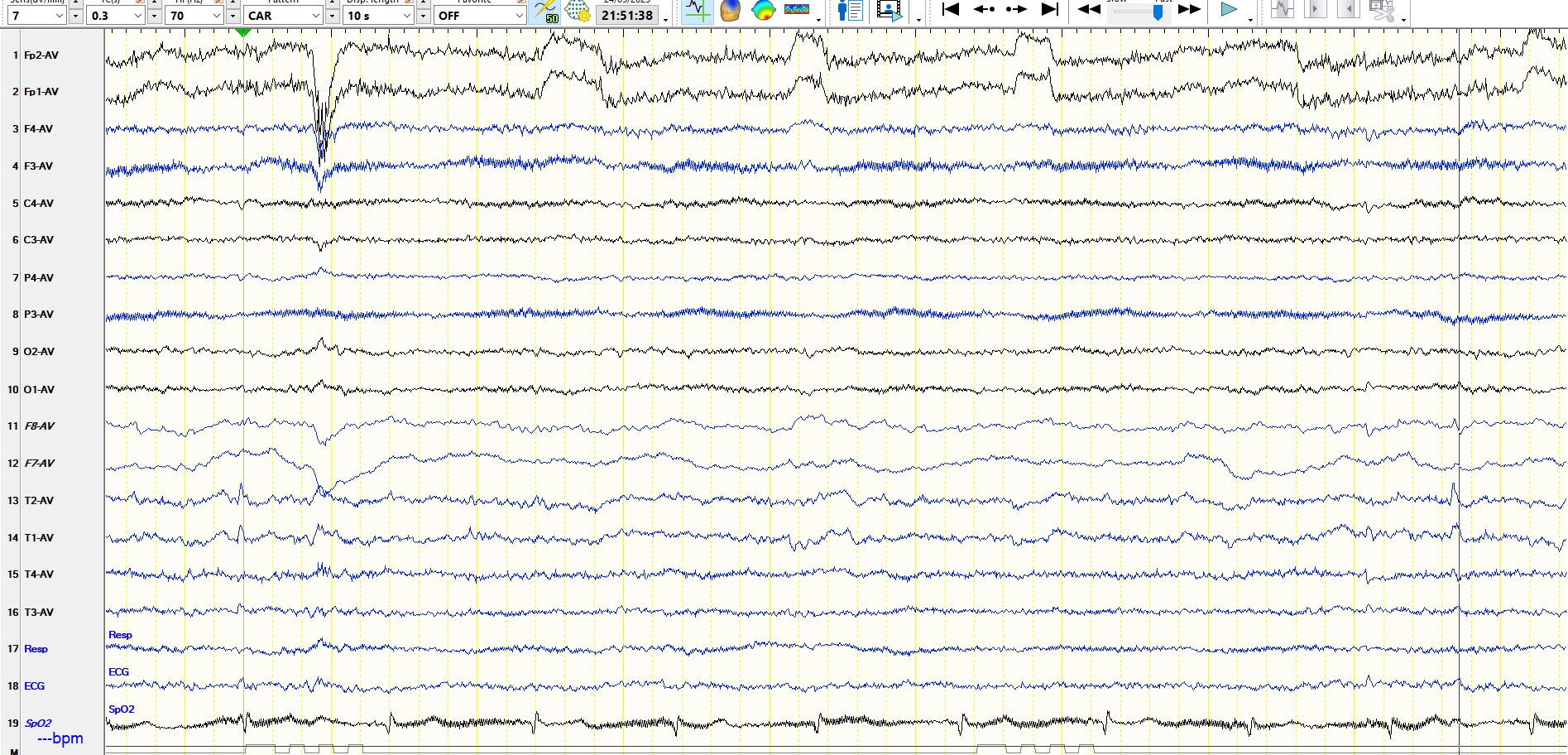
May 25, 2025What is the nature of the following sharply contoured wave? The recording during wakefulness was normal for 3 days of monitoring. The following is from sleep:
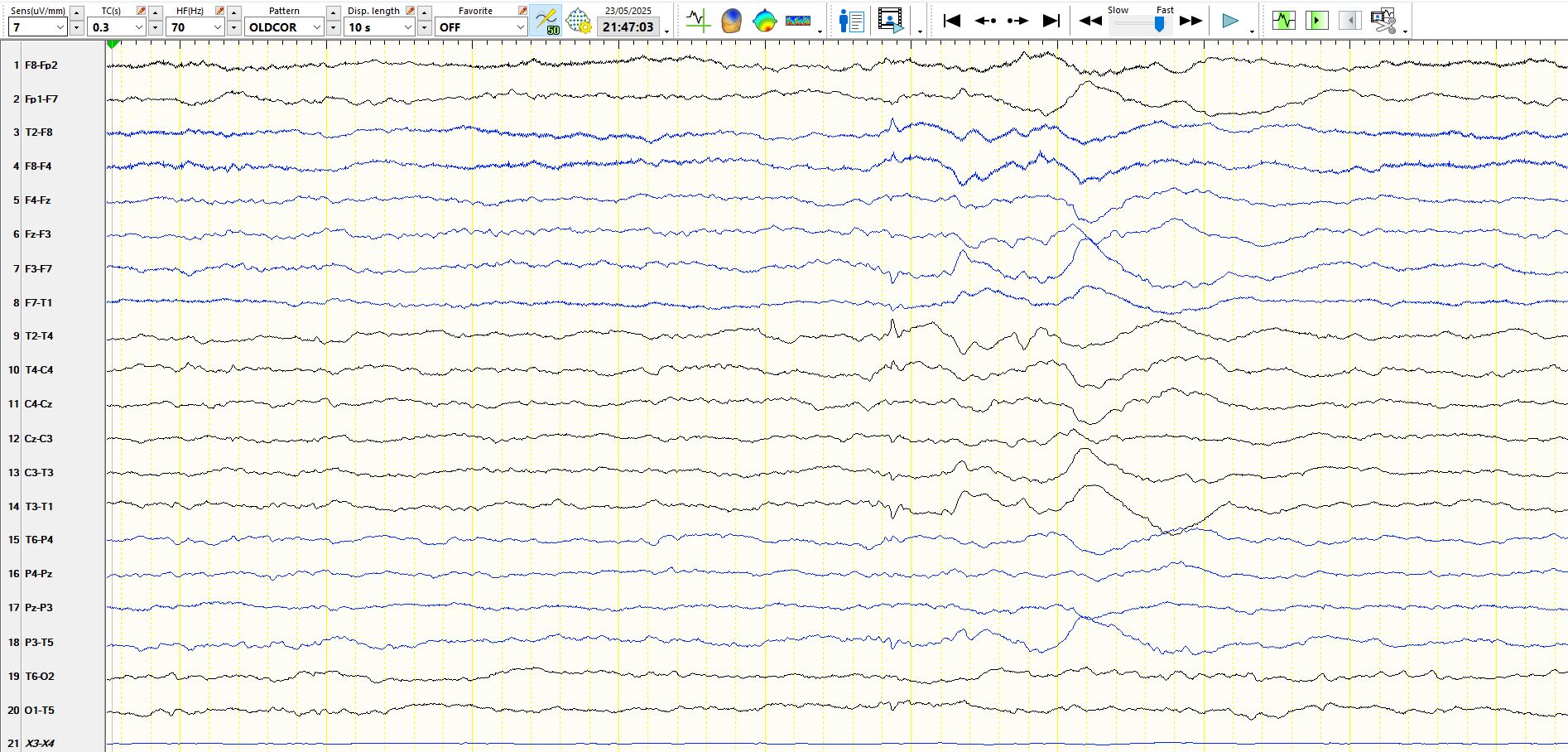
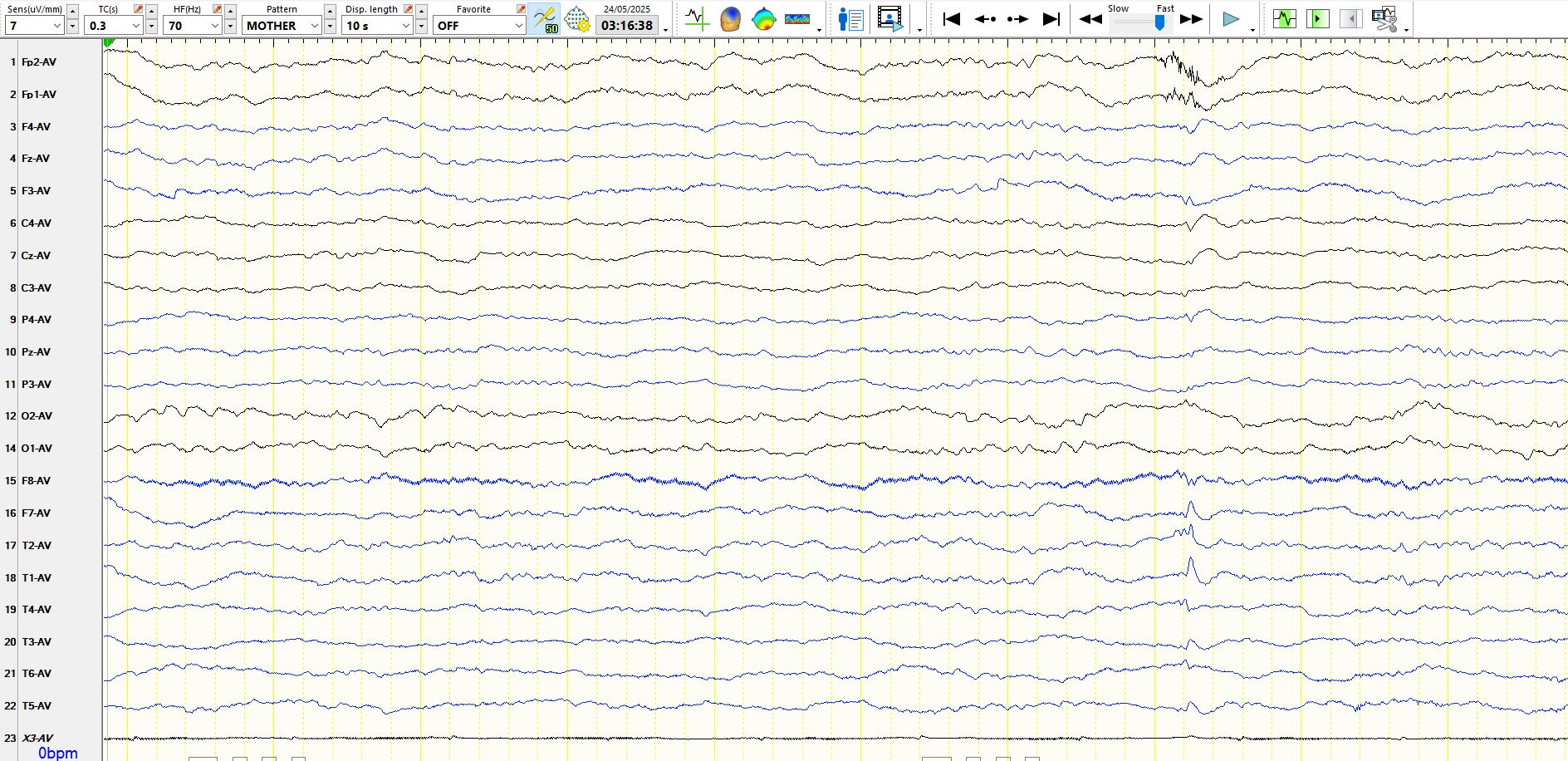
The above discharge appears at M1-F7-M2. It appears during sleep and notice the after coming slow wave in the same derivations as the apiculate wave. It is not coincident with the ECG trace at the bottom and hence not ECG artefact. It does not have the typical field of a small sharp spike, although it is "small". If you are uncertain, and that is certainly a sensible approach to low amplitude apiculate waves in sleep, there is nothing wrong with drawing attention to its presence in the body of your report, without calling it an inter-ictal epileptiform discharges/spike/sharp wave. In these examples, M1, F7 and M2 are excluded from the common average montage, as are the sagittal derivations.
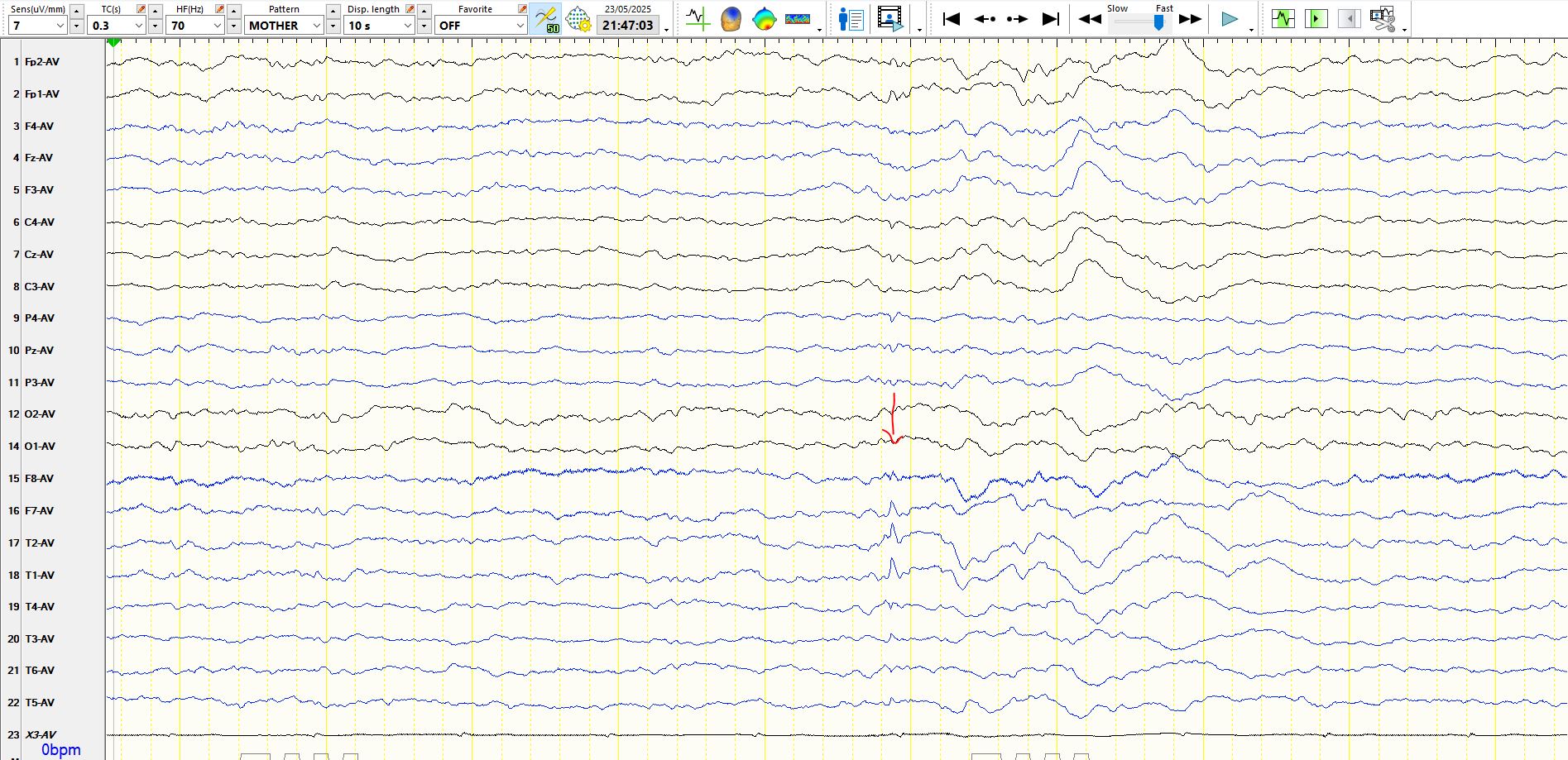
In the above coronal montage, specifically designed to look at the temporal lobes in the coronal plane, it is apparent that the wave cancels at M2-M1. This supports the hypothesis that the spike is generated from the inferior/medial temporal regions, but cannot be reliably lateralized, especially as the medial temporal regions (hippocampus and amygdala) are near the midline, adjacent to the brainstem, and both are relatively remote from M1 and M2.
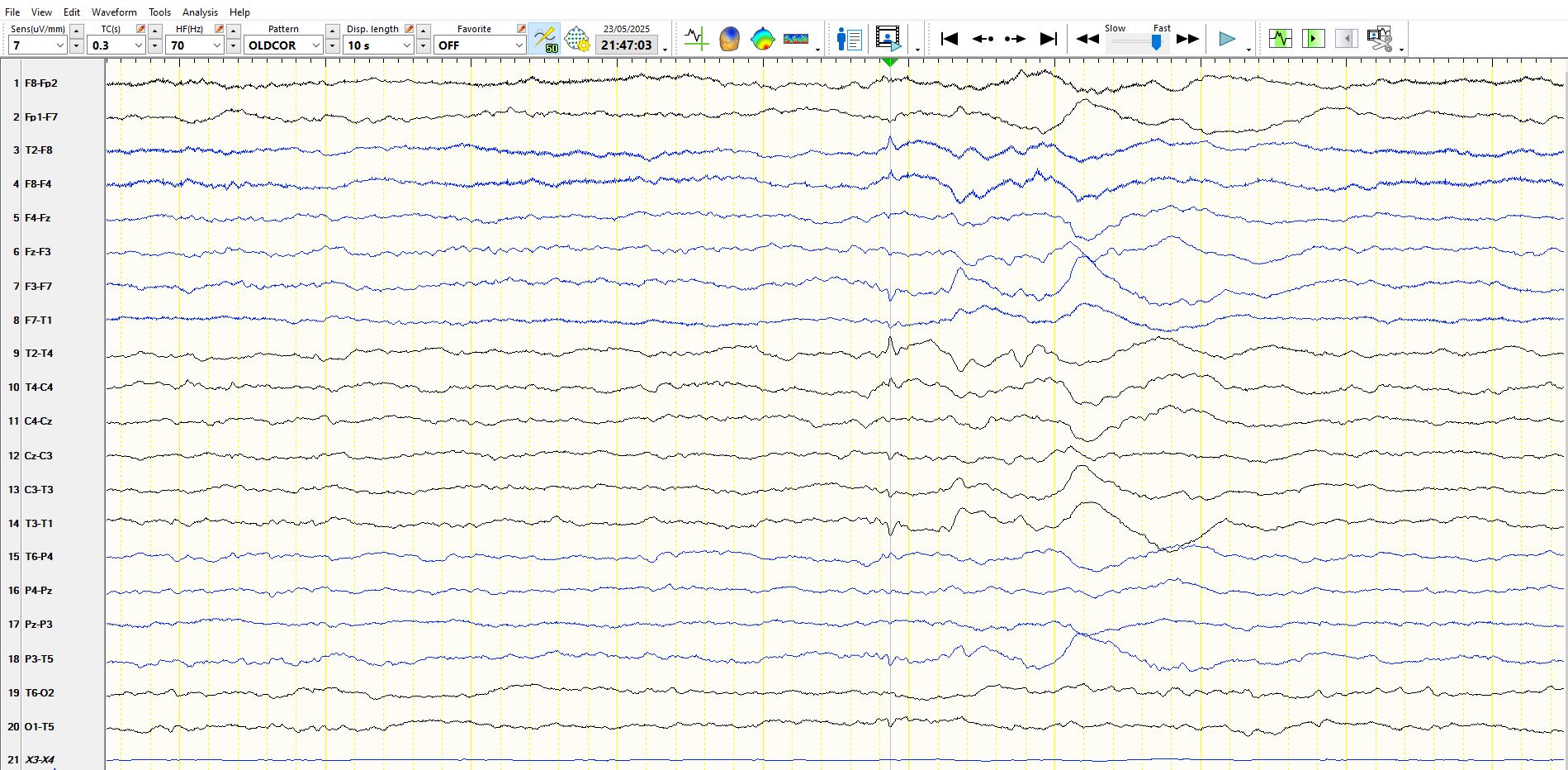
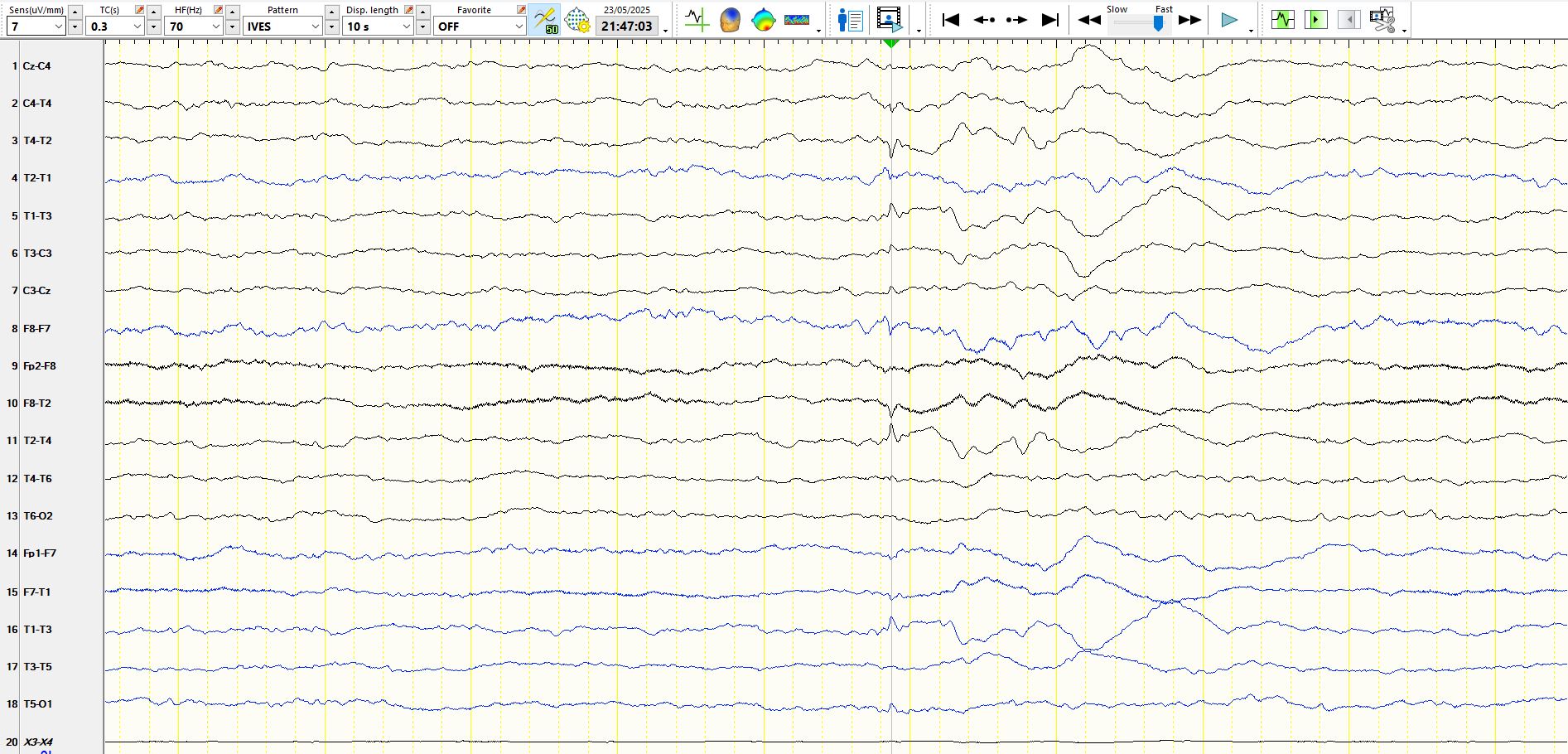
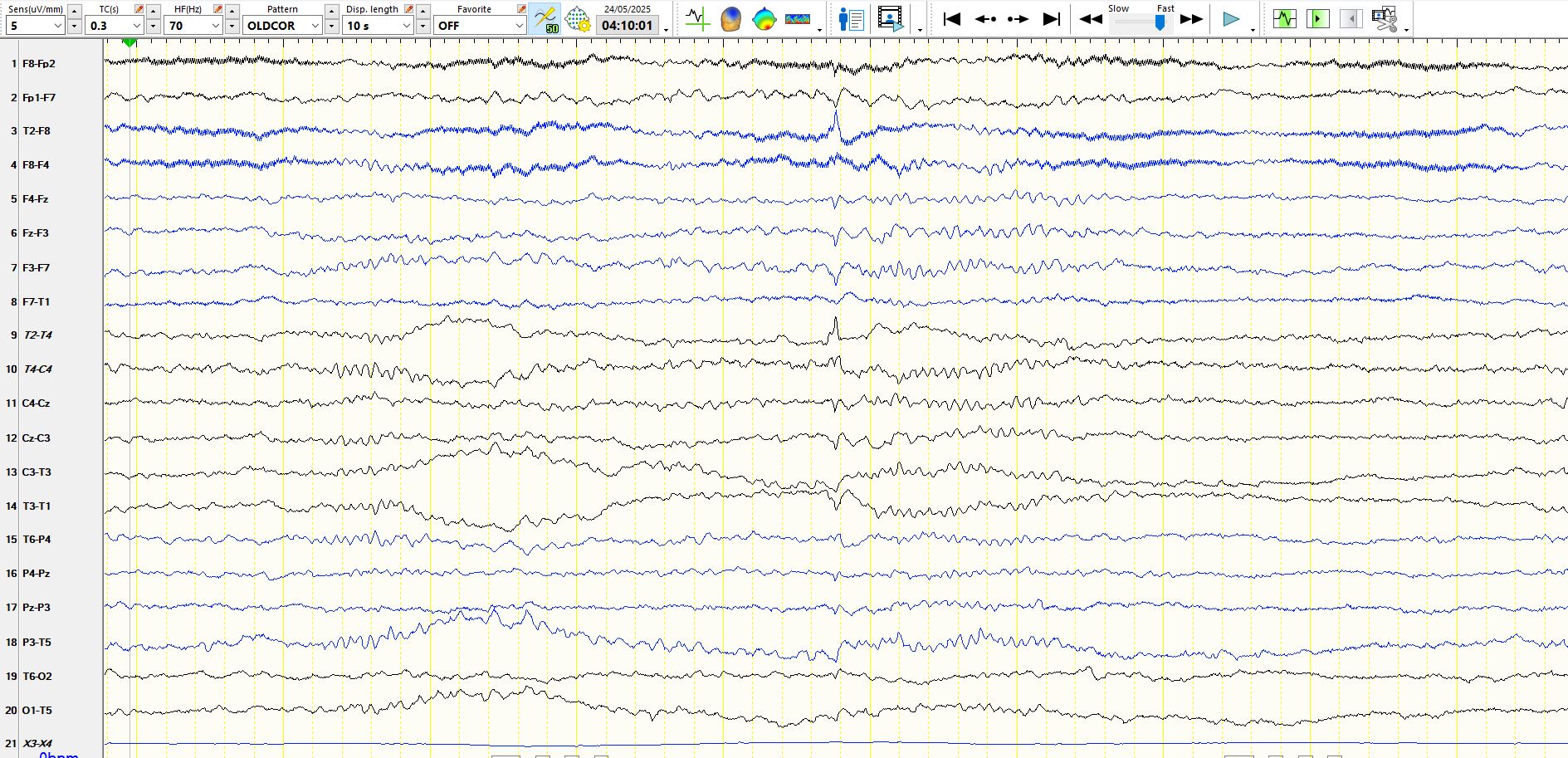
In the above 2 images, where the wave is represented in the coronal montage, there are 3 possible explanations for the waveform. Either it is electro-negative over both inferior temporal regions, or it is simply electropositive at the vertex (and hence a vertex wave) or it is both. However, the electropositive deflection at FZ-CZ is very low in amplitude, when compared to the electro-negative deviation at M2 and M1 (have a look at the referential montage again). This is atypical of a V-wave. You might question the field of this discharge. The discharge is primarily electro-negative over the inferior aspects of both temporal lobes and such a discharge may originate from either inferior temporal region and exhibit volume conduction so that it is seen bilaterally over the mandibular notches (in the same way that a discharge that originates in either frontal-polar region will be seen in the contralateral frontal-polar region). Believe it or not, but this is the nature of the above waveform. You would be correct to be conservative and not call this a spike, but in this instance there were a number of waveforms that had the same characteristics (these are represented after the following image, which is a bipolar representation of the above waveforms). To reiterate, being conservative in calling spikes is the correct philosophy, as you simply don't want to send innocent men to jail for many years. I see way too much of this.

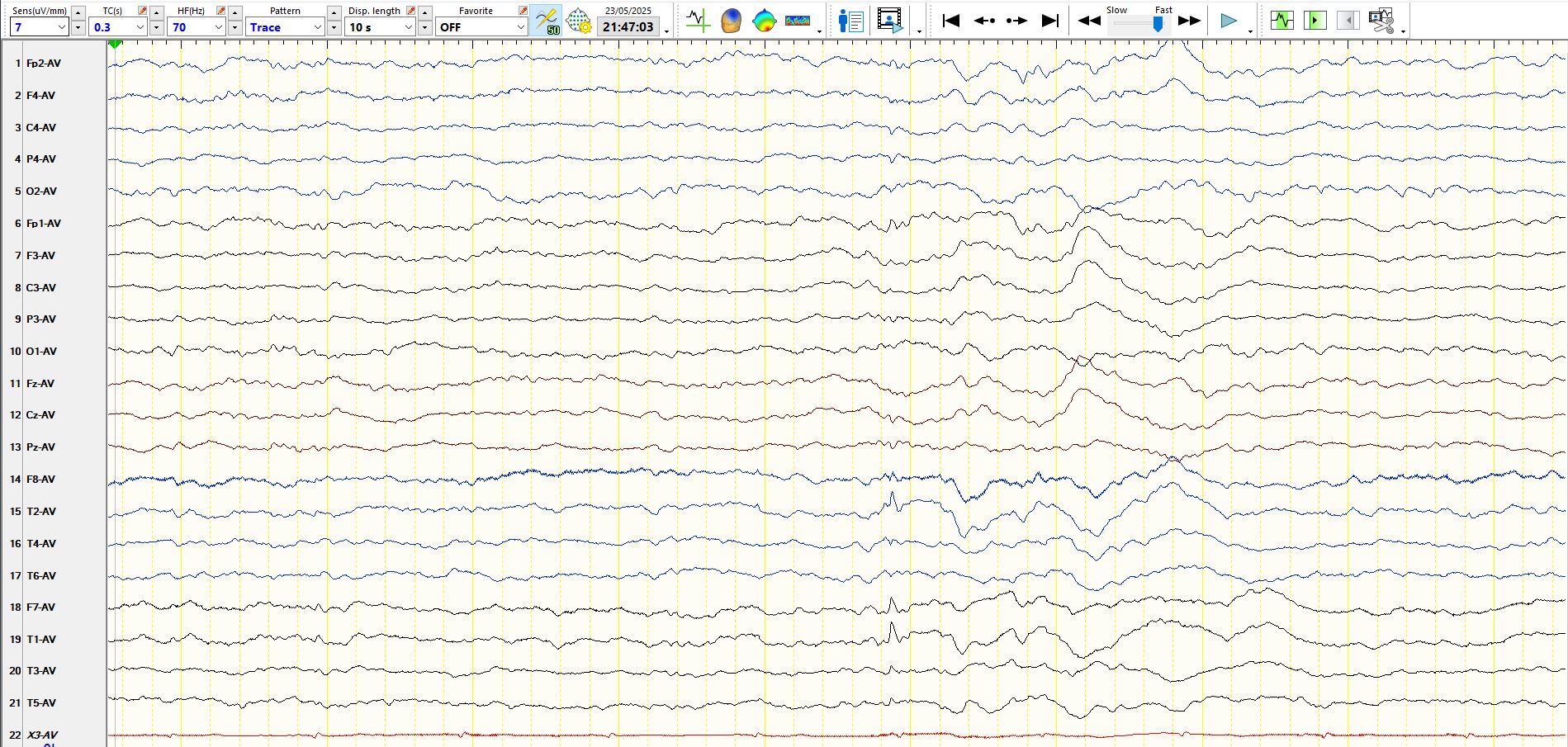
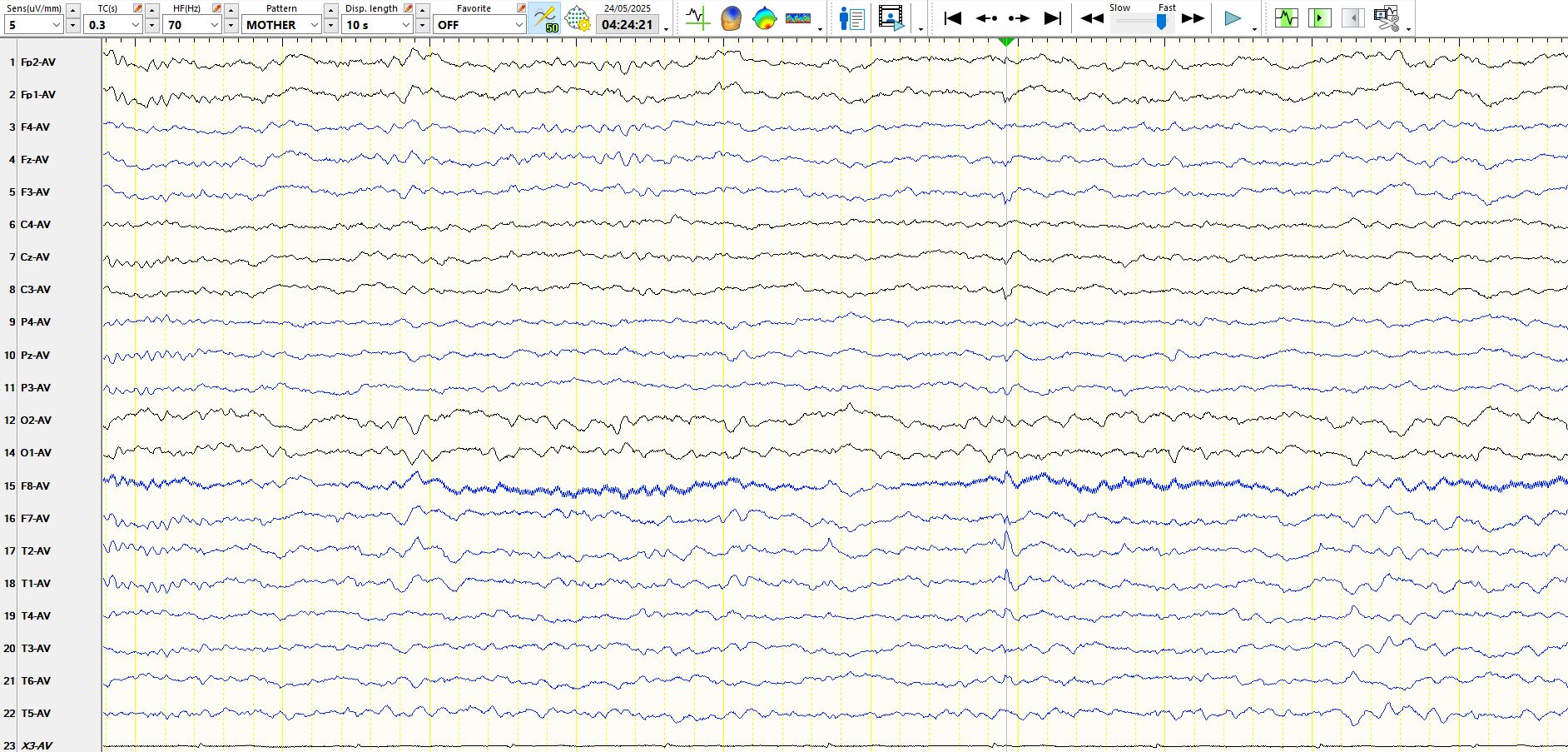
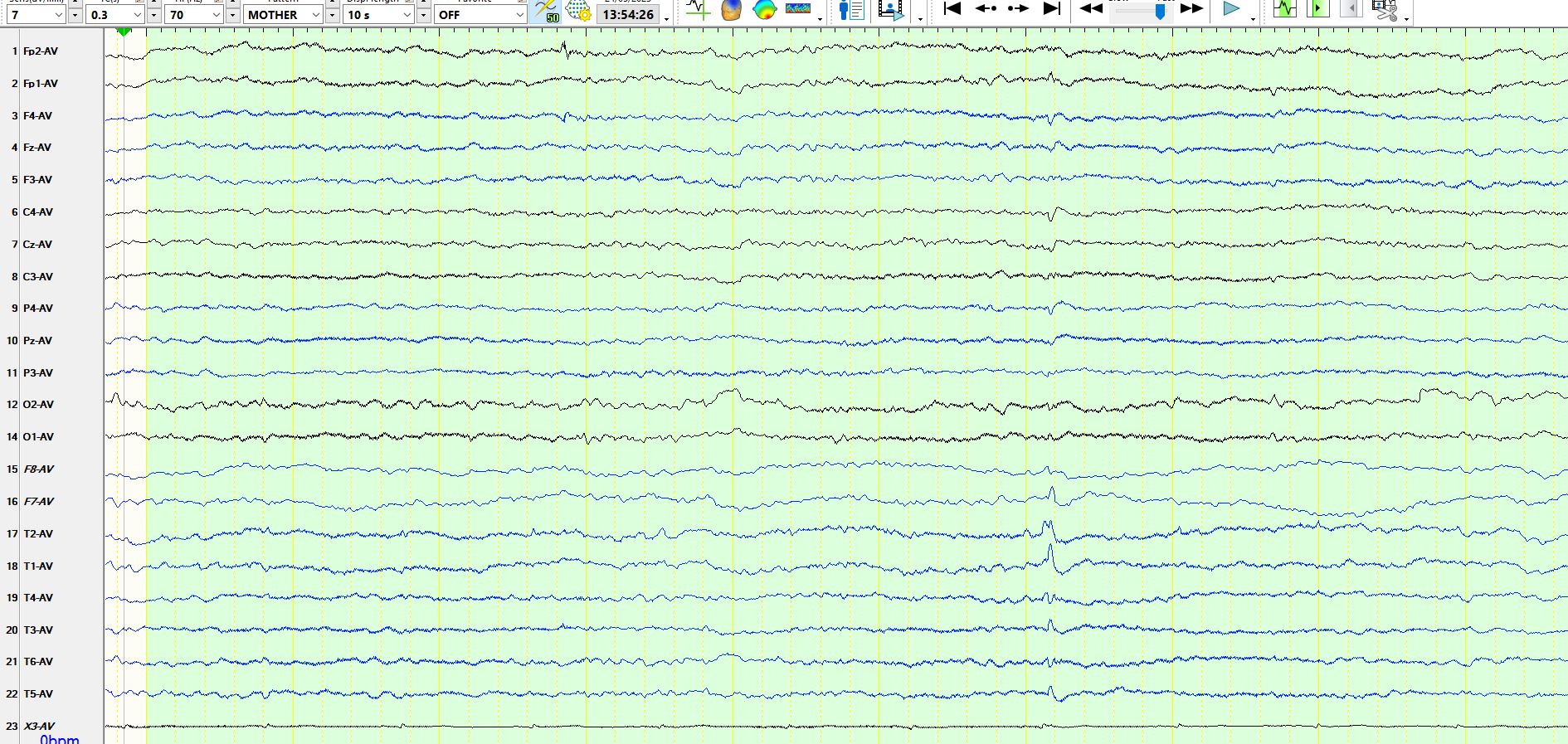
Unsurprisingly, the wave is barely visible on the bipolar anterior-posterior montage, simply because the inferior temporal derivations are not represented in this montage. This neatly illustrates a different point, namely that the conventional anterior-posterior bipolar montage may completely miss inferior temporal discharges, including theta waves, delta waves and spikes. This is an important weakness of this montage, in my view.
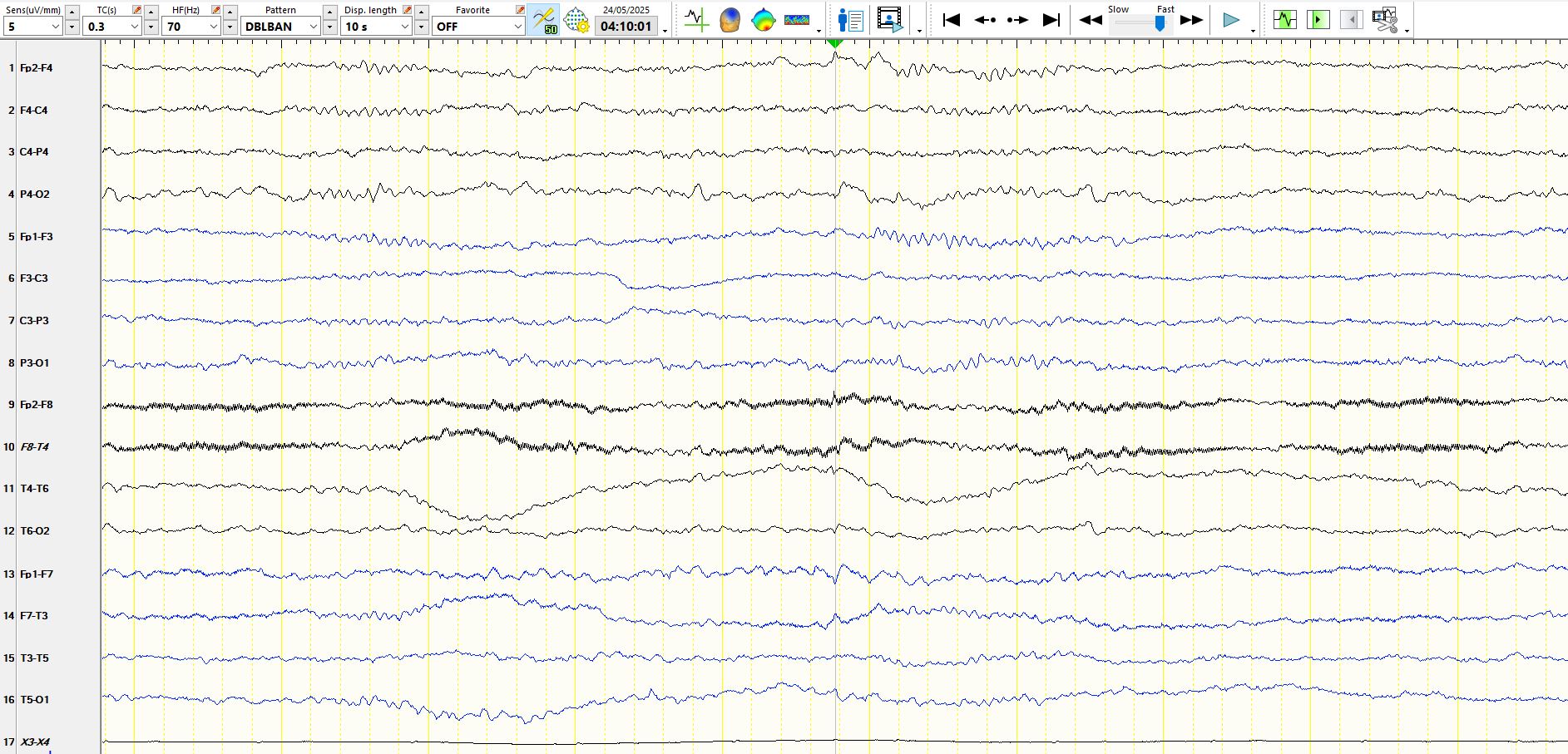
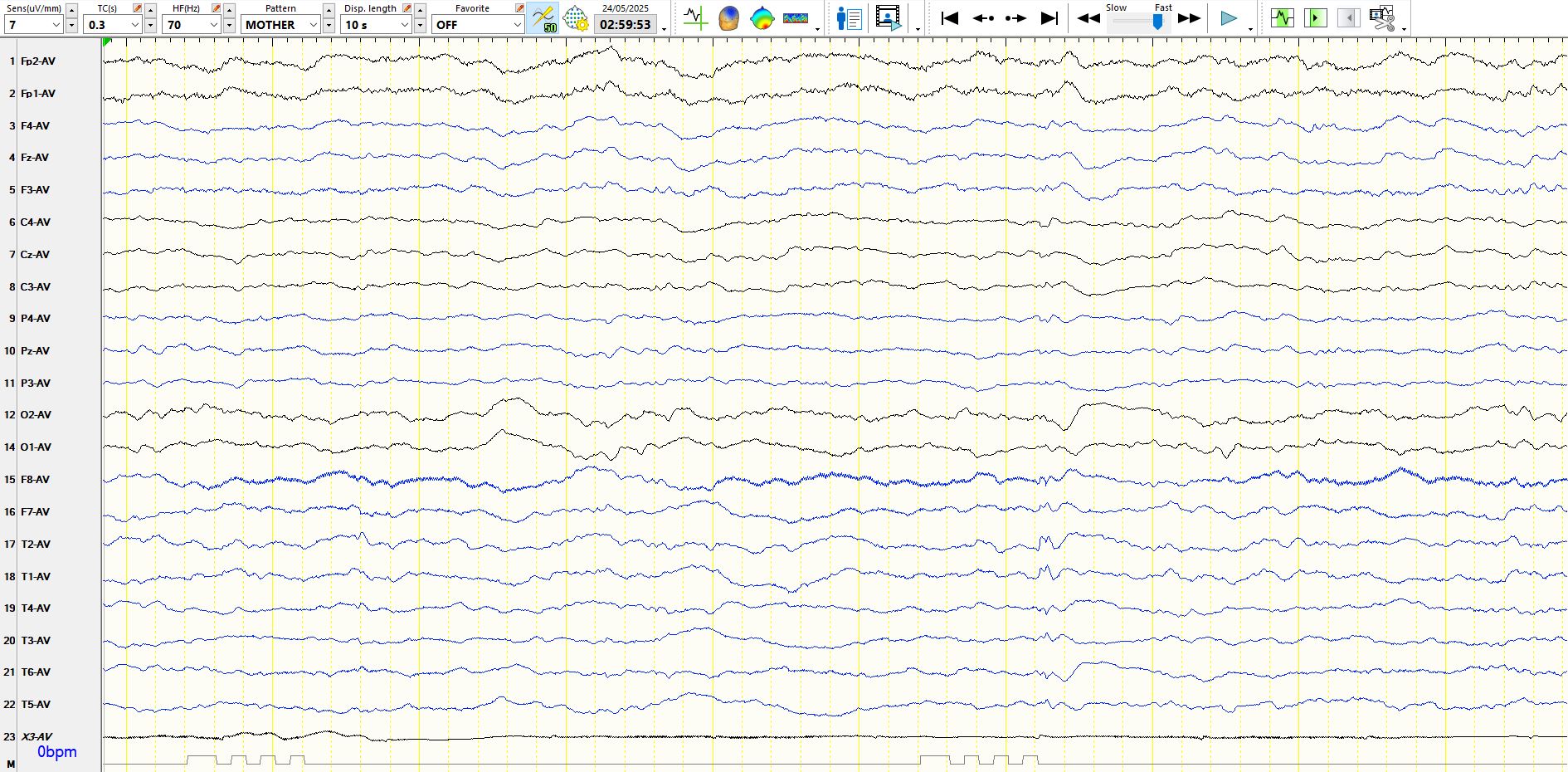
Another example of the same phenomenon:
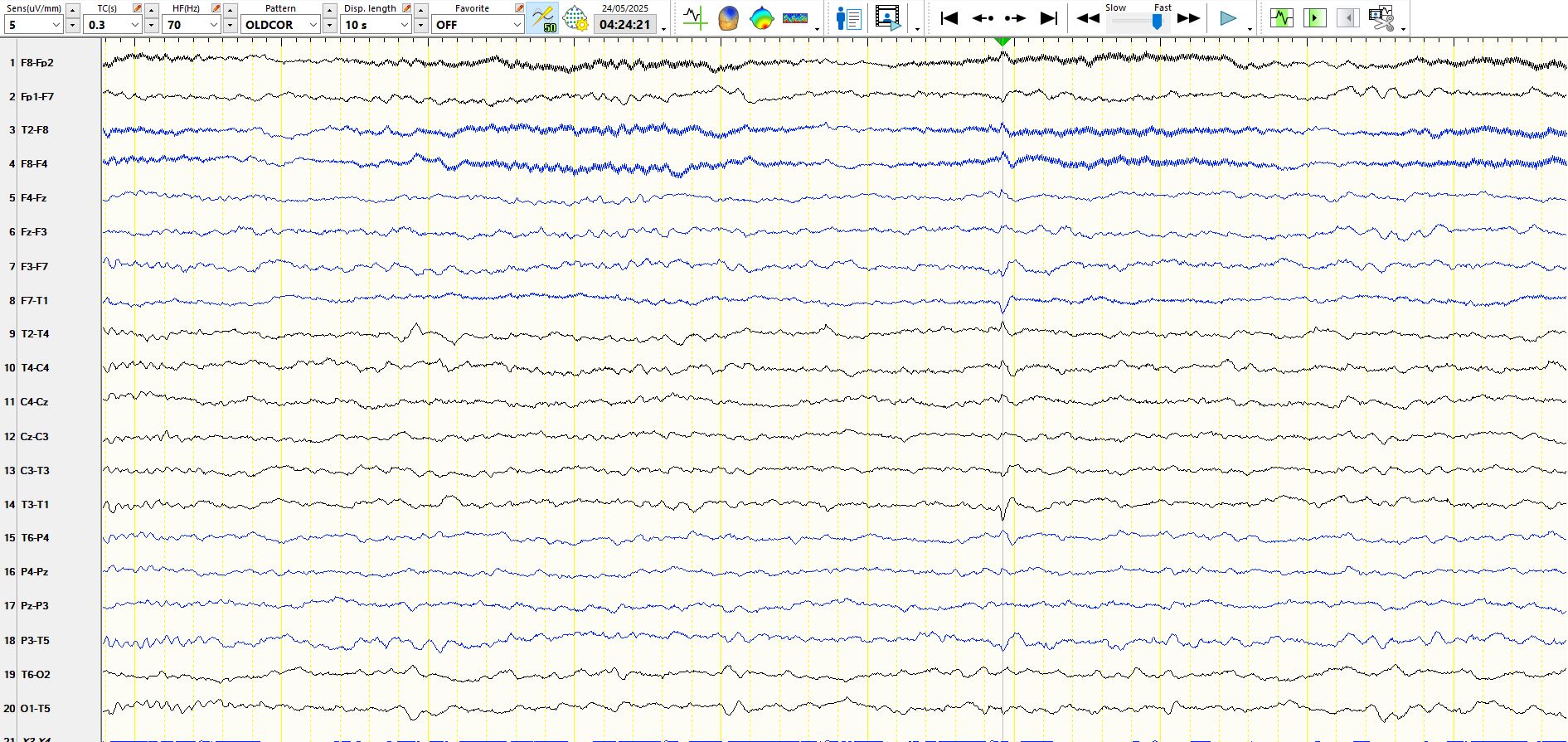
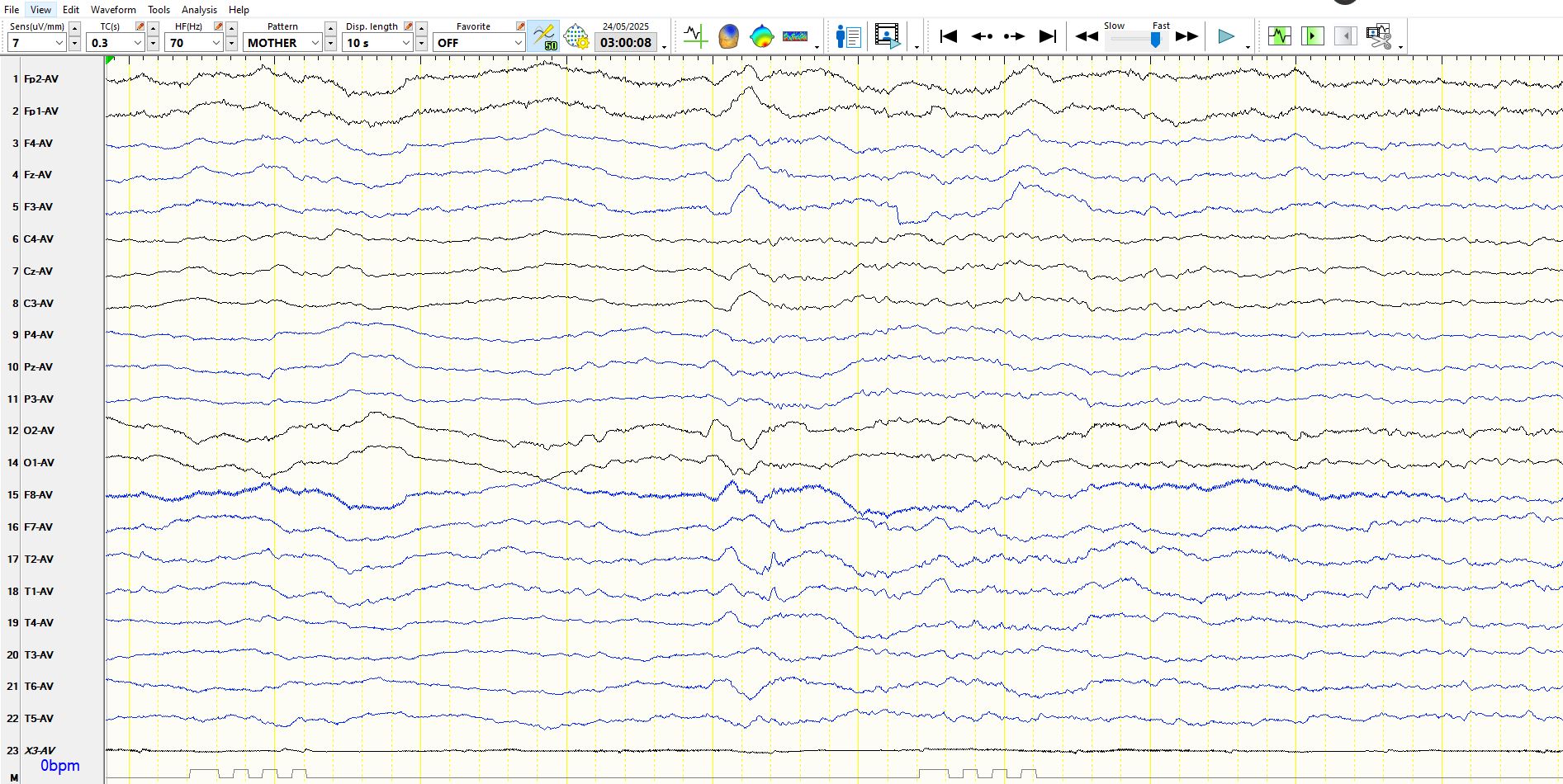
Another example: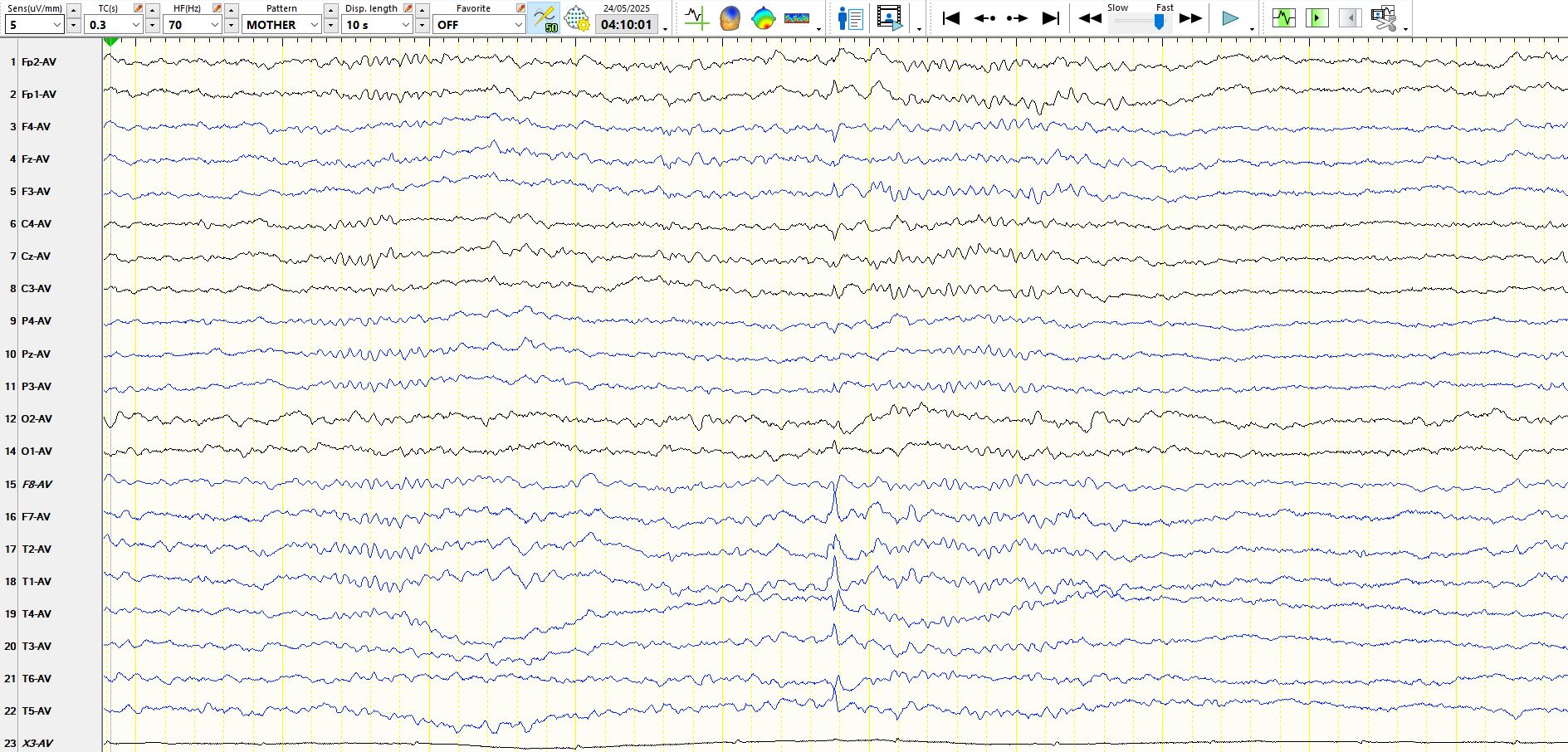
Contrast the morphology and field of the above discharges with a small sharp spike illustrated elsewhere; Click here
11y, seizures
More of the same from the 41y-old:
The following is taken from a subdural recording of a different patient where the electrodes are placed over the inferior temporal regions. Electrodes 1-8 are taken orthogonally from the right anterior temporal region, where number 1 is located most mesially over the amygdala region and 8 is located over the right temporal convexity. Electrodes 9-16 are located posterior to the above 8 electrodes, where 9 is most medial and 16 is over the convexity. 17-24 and 25-32 are located over the left medial temporal region in the same way as the right temporal electrodes, with 17 and 25 located Over the left medial temporal region and 24 and 32 over the left temporal convexity. The point of showing this is to demonstrate the field of the discharges, straddling both inferior temporal regions. Many other such electrodes, implanted elsewhere over the brain, do not demonstrate this discharge; hence it is not a generalised discharge
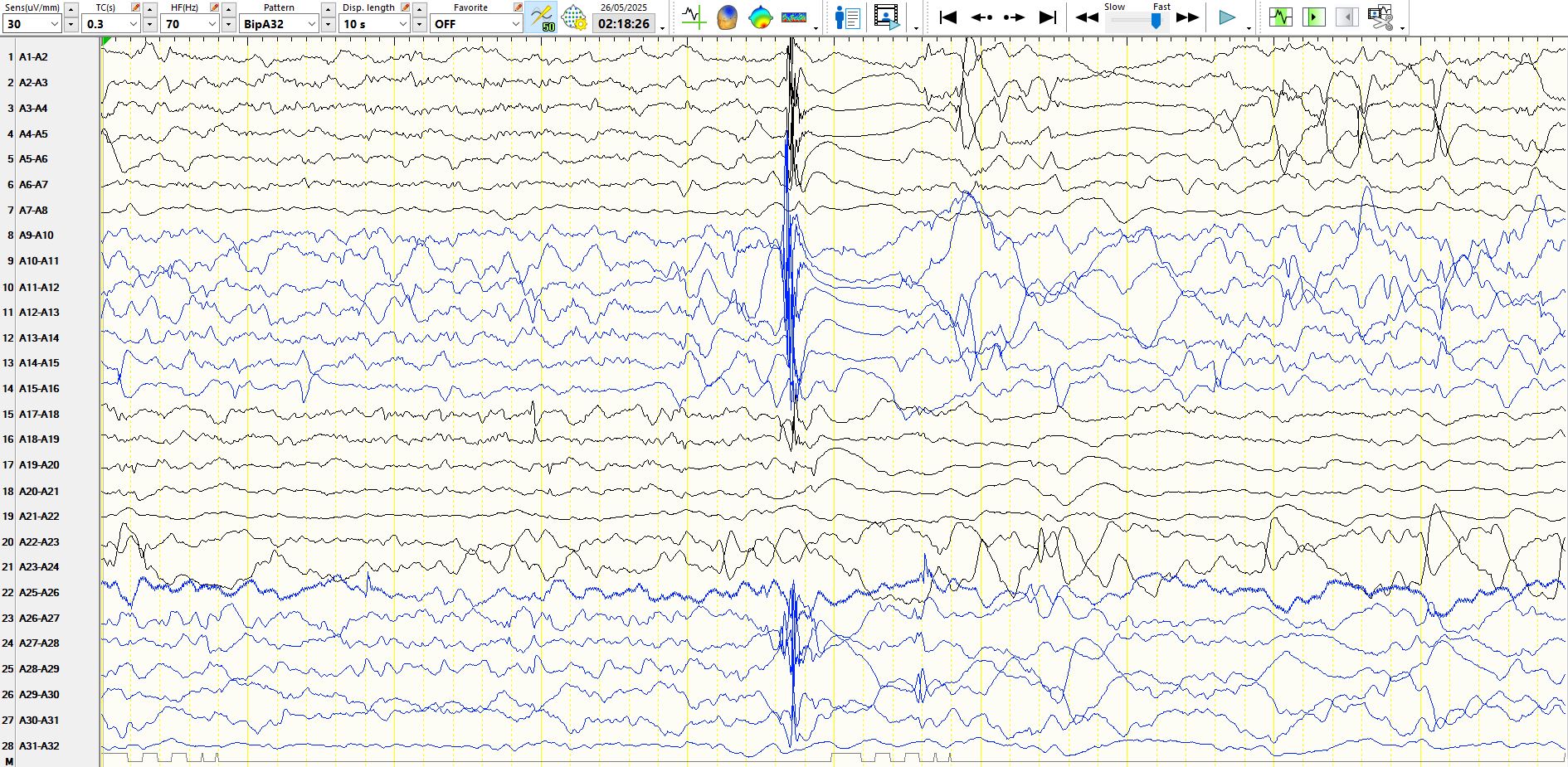
Incidentally, 2 hippocampi are connected by the hippocampal commissure
White-matter commissures: a clinically focused anatomical review - PubMed
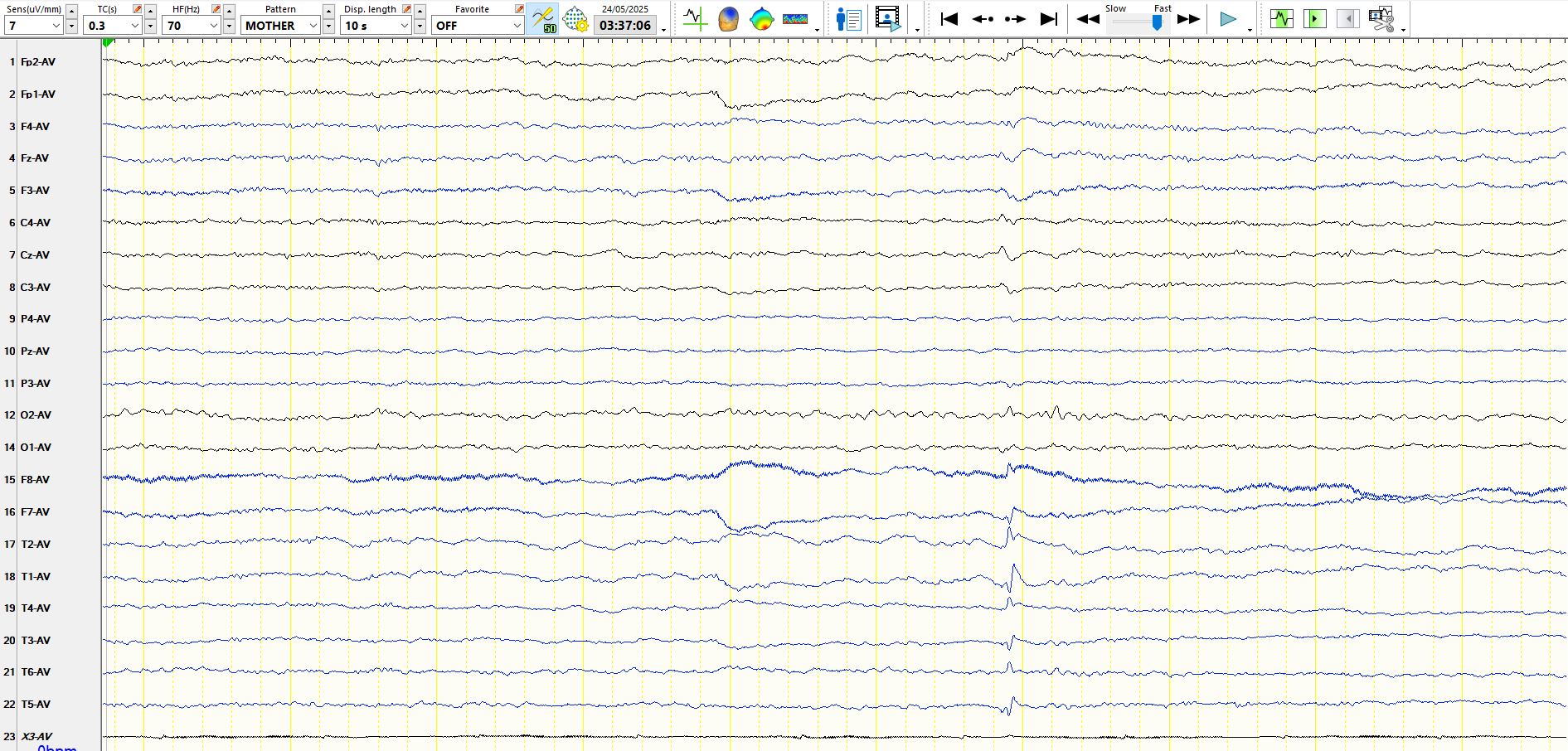
Here is another spike from the 41y in sleep:
and awake (one could easily pass these by):
PS be on the look-out for small sharp spikes in wakefulness. But these are not them!