27, referred for epilepsy vs NES
Jun 27, 2025Have a look at the following few pages:
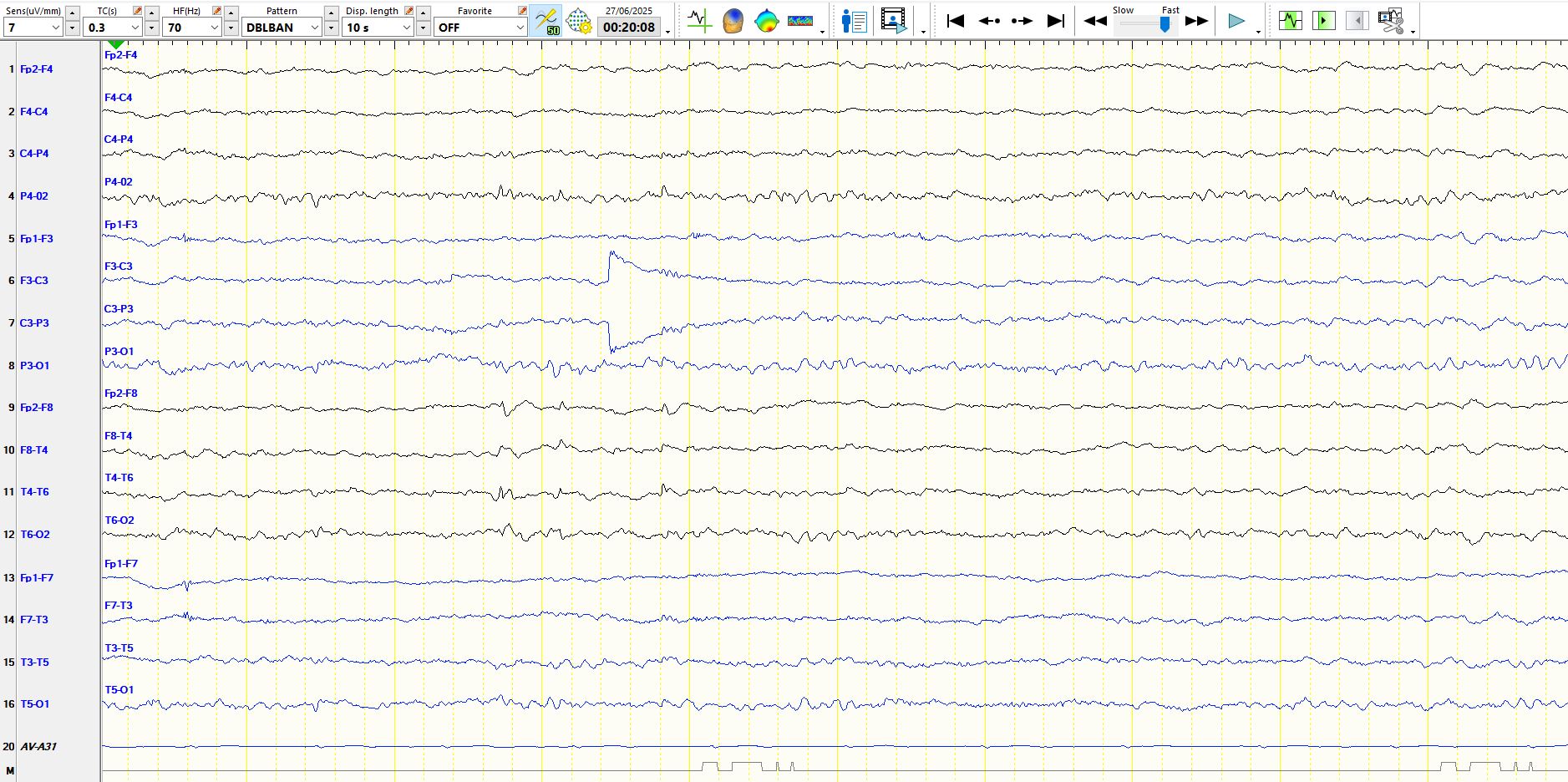
The following page is the bipolar representation of the above page:
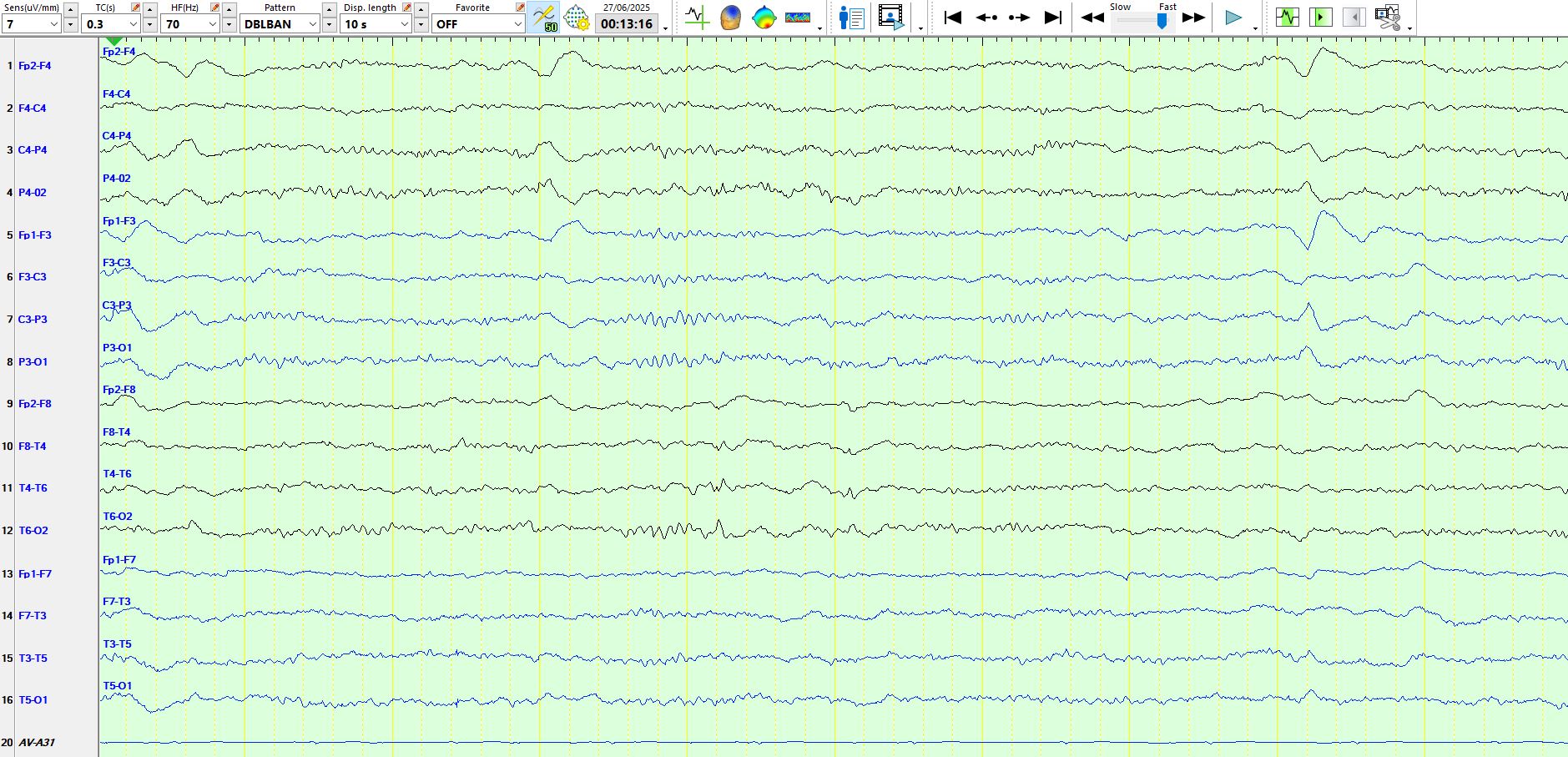
In the above, the wave is seen at T6-T4 and is electro-negative, excluding the possibility of a POST. Moreover, it appears over the posterior temporal region rather than the occipital region. It is low in amplitude, raising the possibility of a small sharp spike, but the above discharge has a restricted field, unlike small sharp spikes and there is a wave approximately 1 second later which is not particularly sharp and therefore does not share a morphology with small sharp spikes. There is no suggestion that it is an artefact.
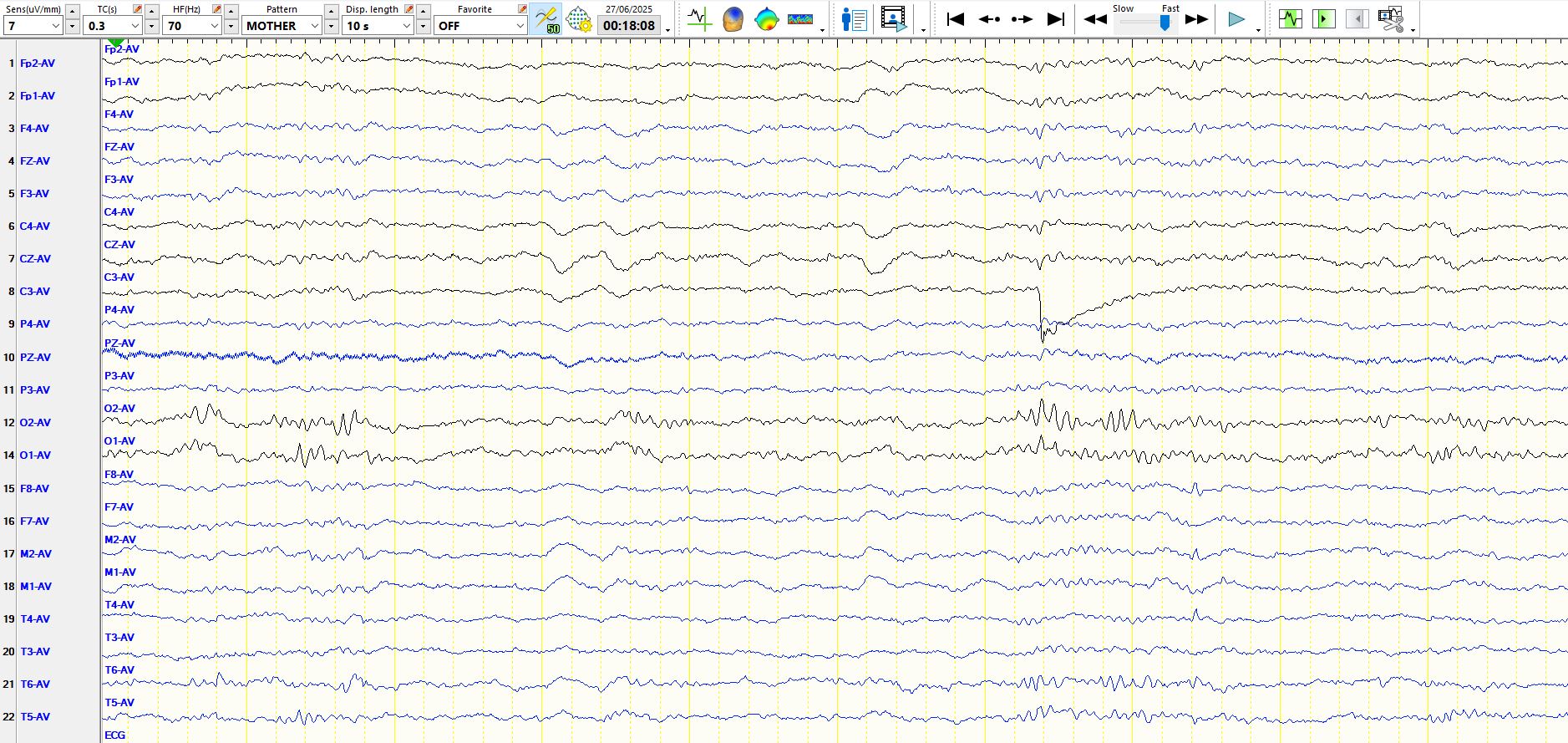
This is a different page:
In the above image, the first wave has the same characteristics as the previous example. The second wave in the occipital regions is physiologically normal in sleep; the sharp wave is part of the background and there is a slower wave in both occipital regions. Hence, the spike-and-wave appearance is misleading, and you should ignore it anyway, given the low amplitude.
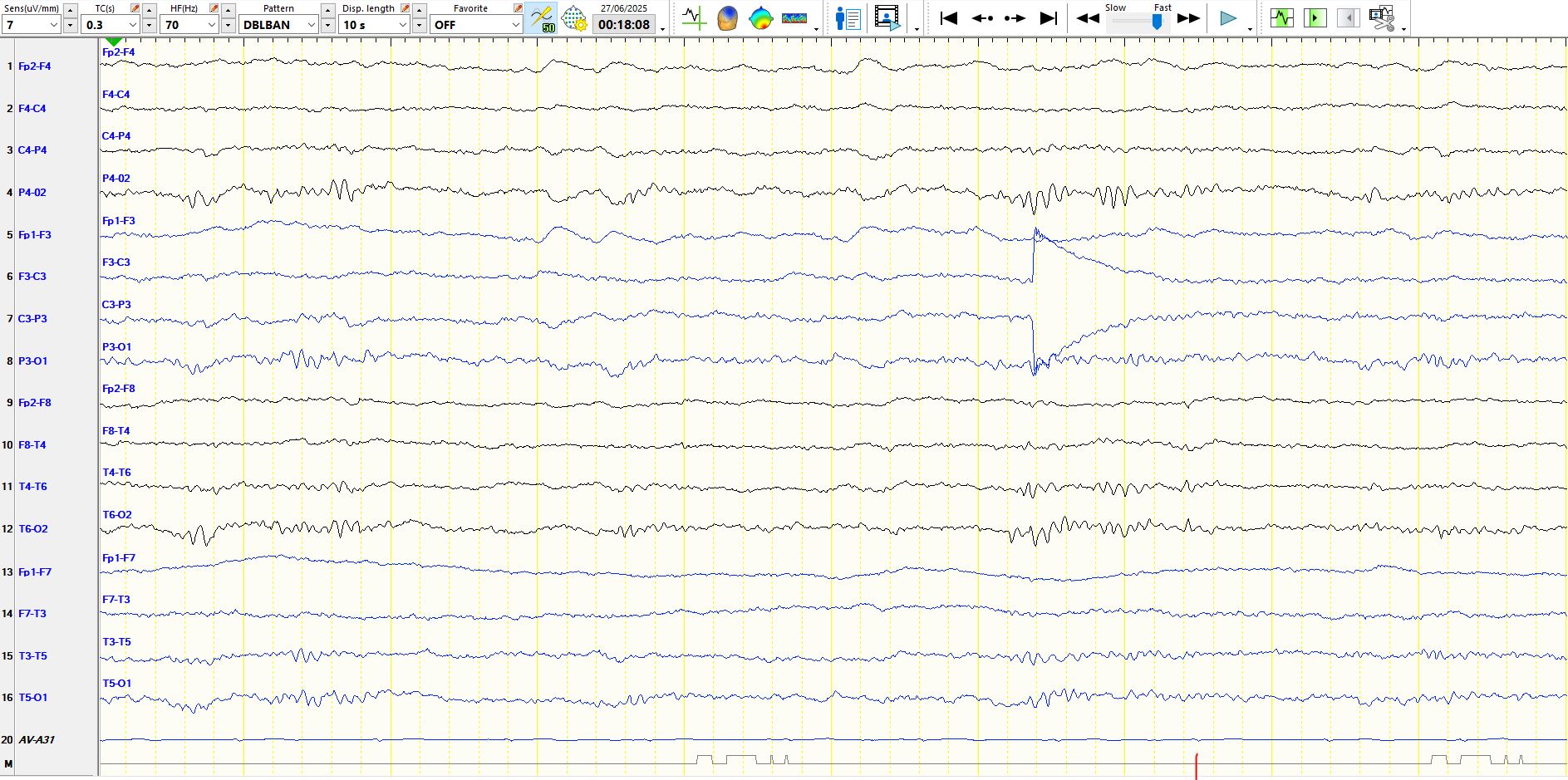
The following is the bipolar representation of the above page:
On the bipolar, the second wave has the morphology and polarity of a POST.
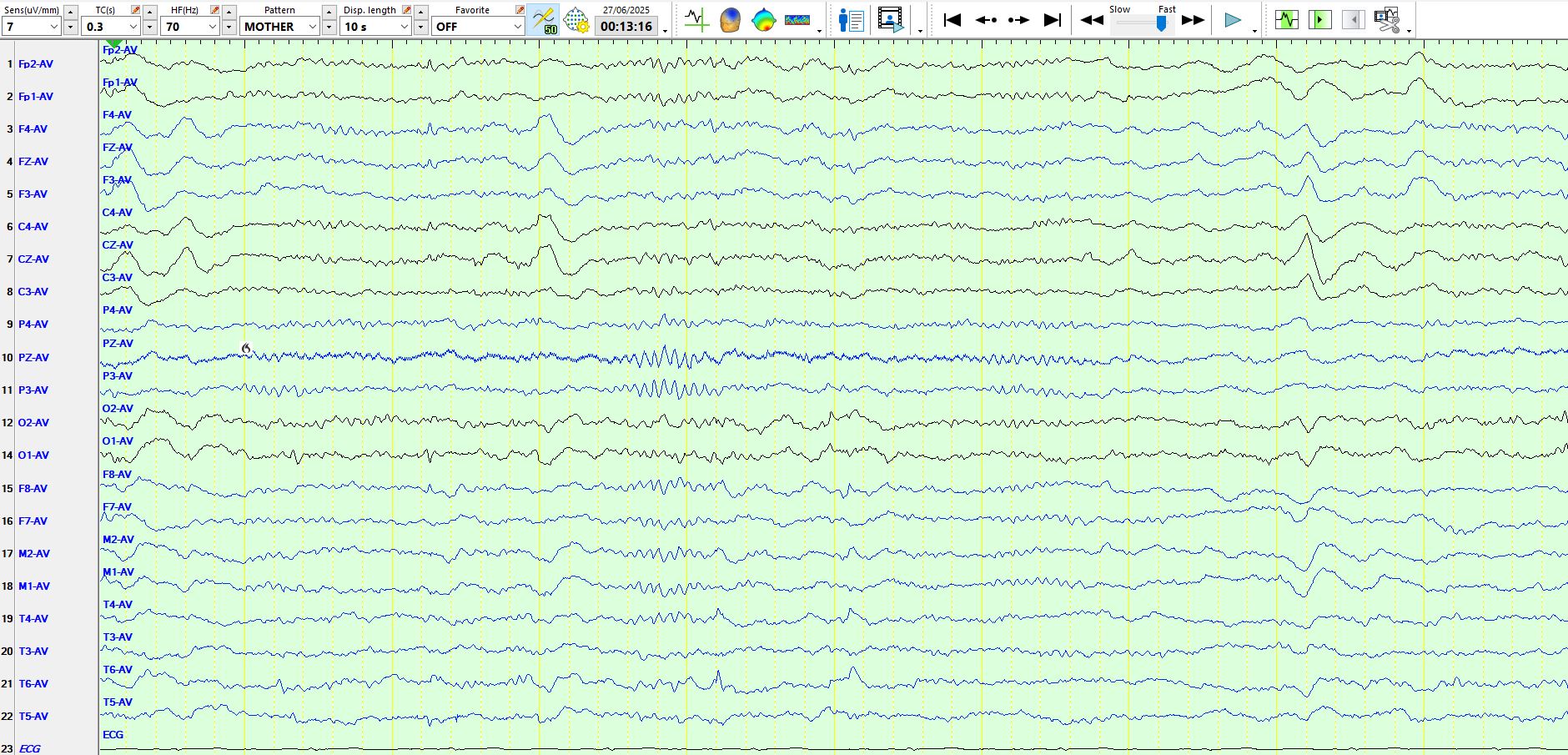
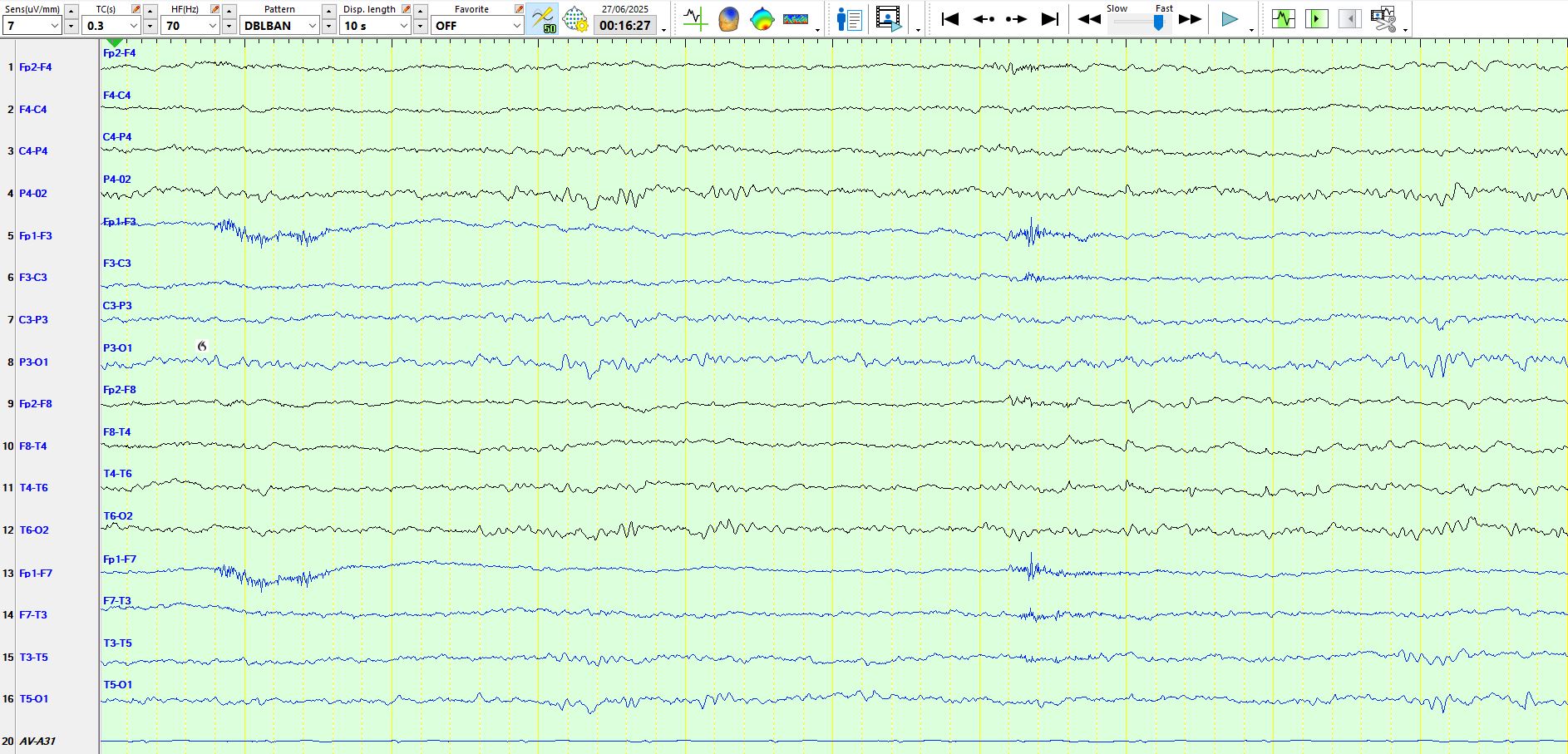
Here is a third page:
The above page is particularly telling. the first low amplitude apiculate wave appears electropositive at T6-T4 (seven seconds) and synchronicity electro-negative at F8-M2, indicative of a dipole. There is no involvement of the left temporal derivations, excluding a small sharp spike. You will also notice a train of rhythmic, approximately 4 Hz theta waves prior to and around the time of these discharges. The second discharge appears approximately 500 ms later and has the opposite polarity of the first discharge. If you look carefully, you might see a few more low amplitude similar waveforms after the first two, especially at T6-T4.
The following is the bipolar representation of the above page:
The bipolar montage confirms the above. The rhythmic theta waves that appear at F8-T4-T6 throughout the last three seconds of the page can be clearly seen, while the frequency of the discharge and the restricted field is not typical of phantom spike-and-wave. Although one has to be doubly careful about calling low amplitude apiculate waves inter-ictal epileptiform discharges, the case here becomes compelling, given the collection of the characteristics described above and the exclusion of alternative possibilities.
Here is the 4th page:
In the above, if you only saw this page, you would rightly have to be very sceptical about the nature of the low amplitude apiculate wave about 2.5 seconds from the end of the page at F8-M2-T4-T4. The above illustration is to draw your attention to how inconspicuous inter-ictal epileptiform discharges may be, but equally you should be vaccinated against calling these inter-ictal epileptiform discharges when you see similar waveforms on other EEGs.
Here is the bipolar representation of the above page:
In the image above, you can see that the field is very similar to the previous discharges.
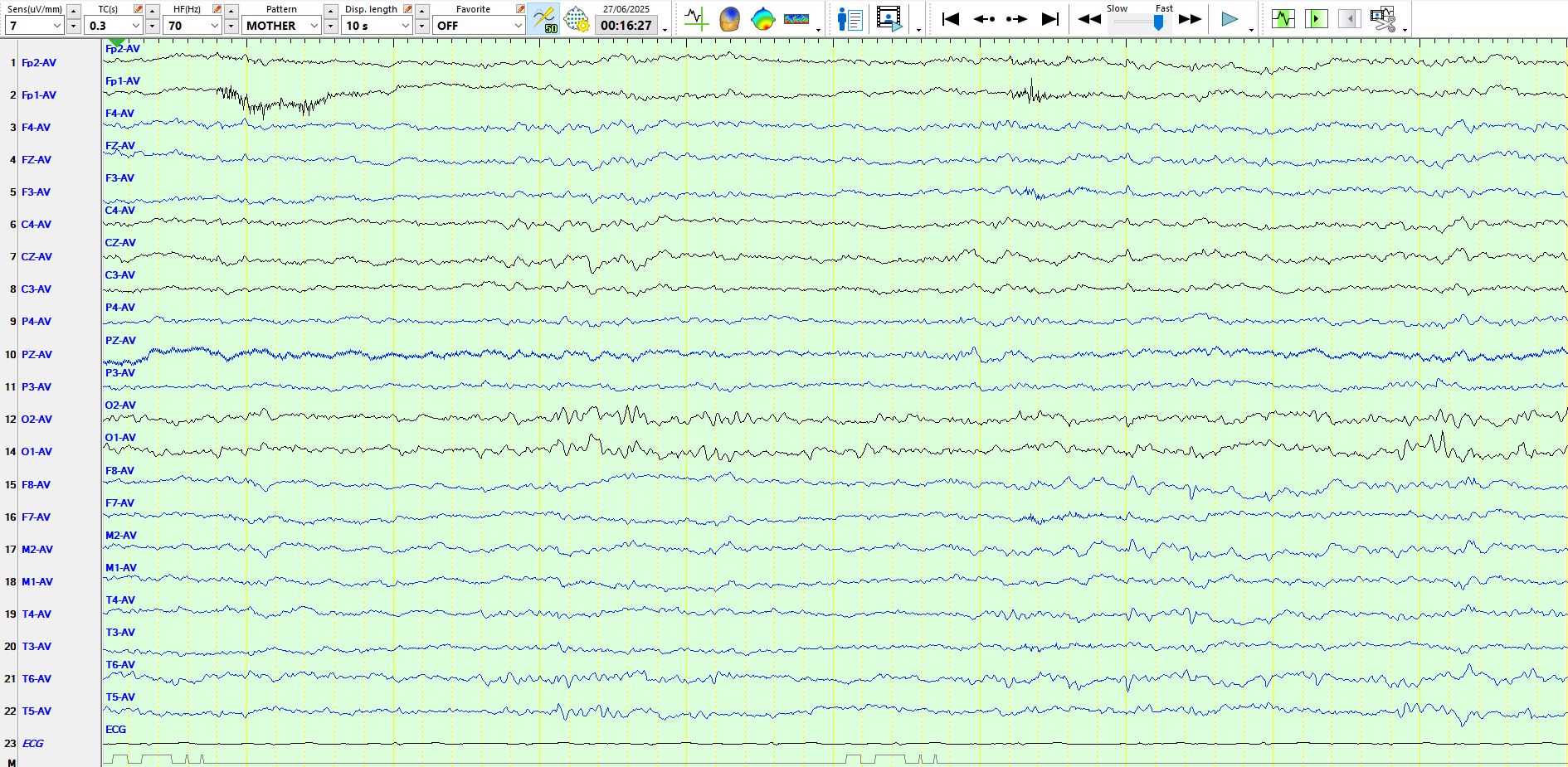
Here is the 5th page:
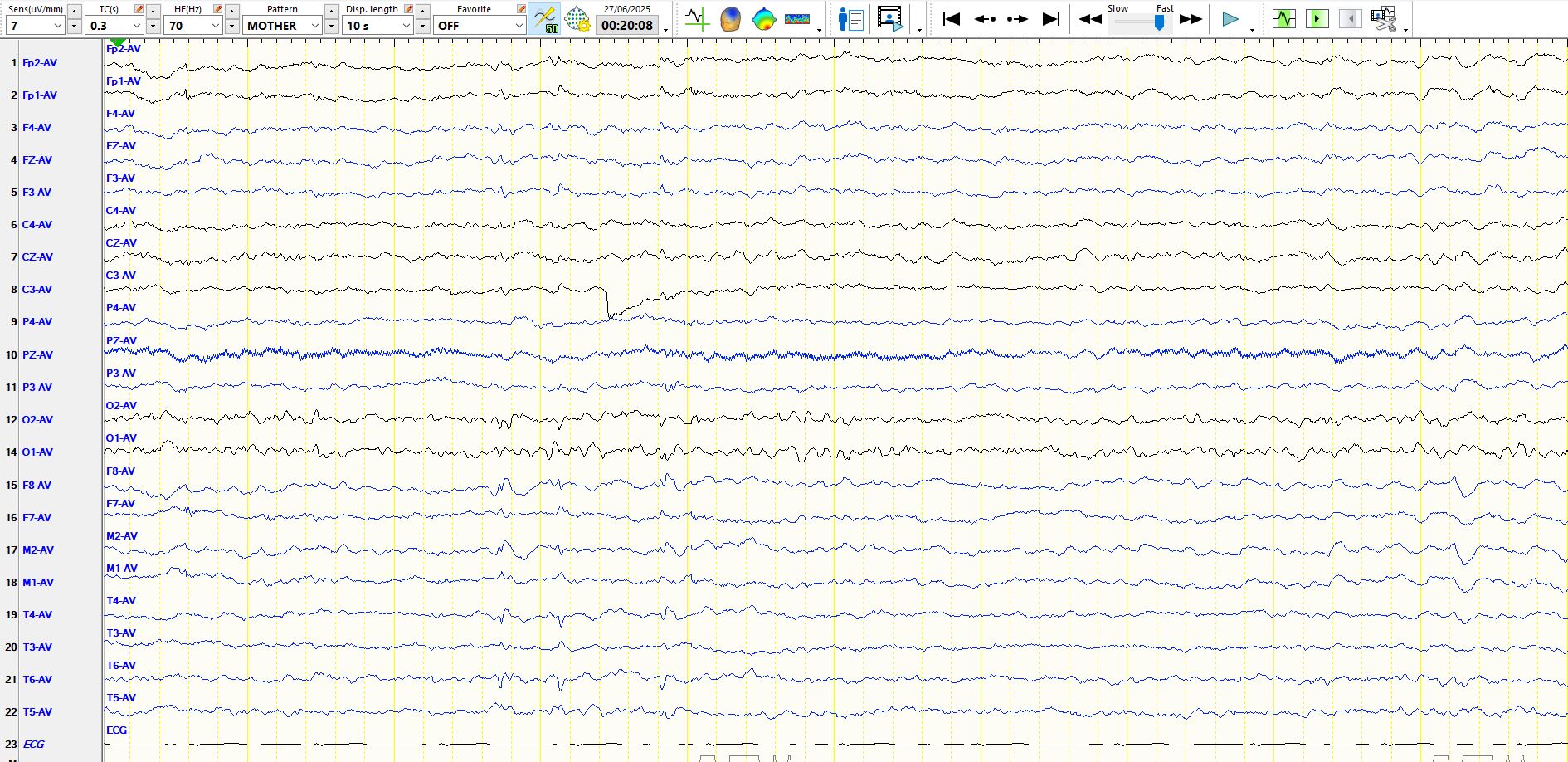
Here is the above page on bipolar montage:
Bottom line?
Be very sceptical about low amplitude sharply-contoured waves. In this example, if you had voted for anything other than inter-ictal epileptiform discharges, you would not be wrong, as you likely will not be over-calling sharply contoured discharges in your everyday EEG reporting. This is an admirable trait and a quality that you should retain. The above example is an exception and as always one has to be careful of the exception changing your behaviour.
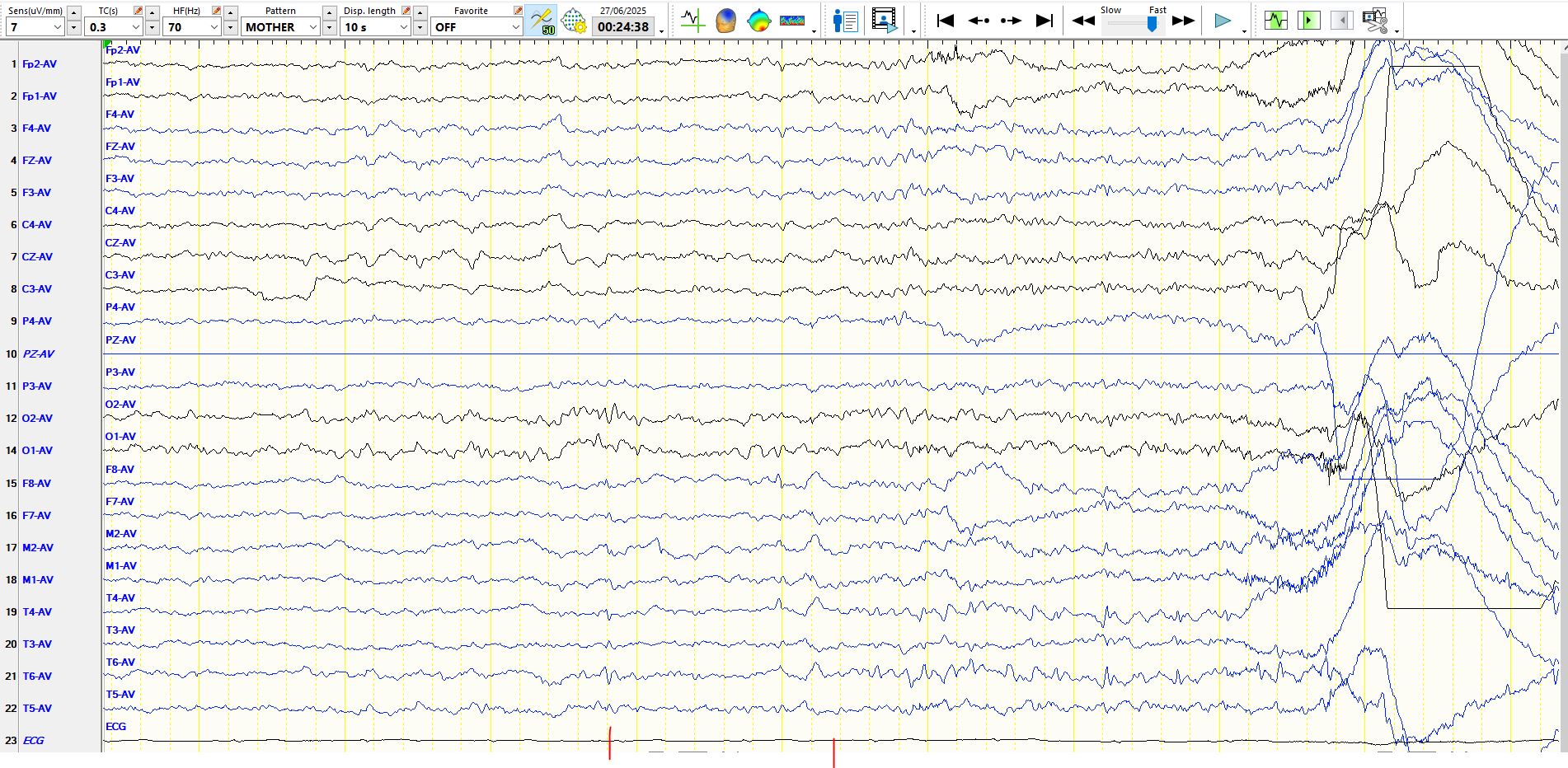
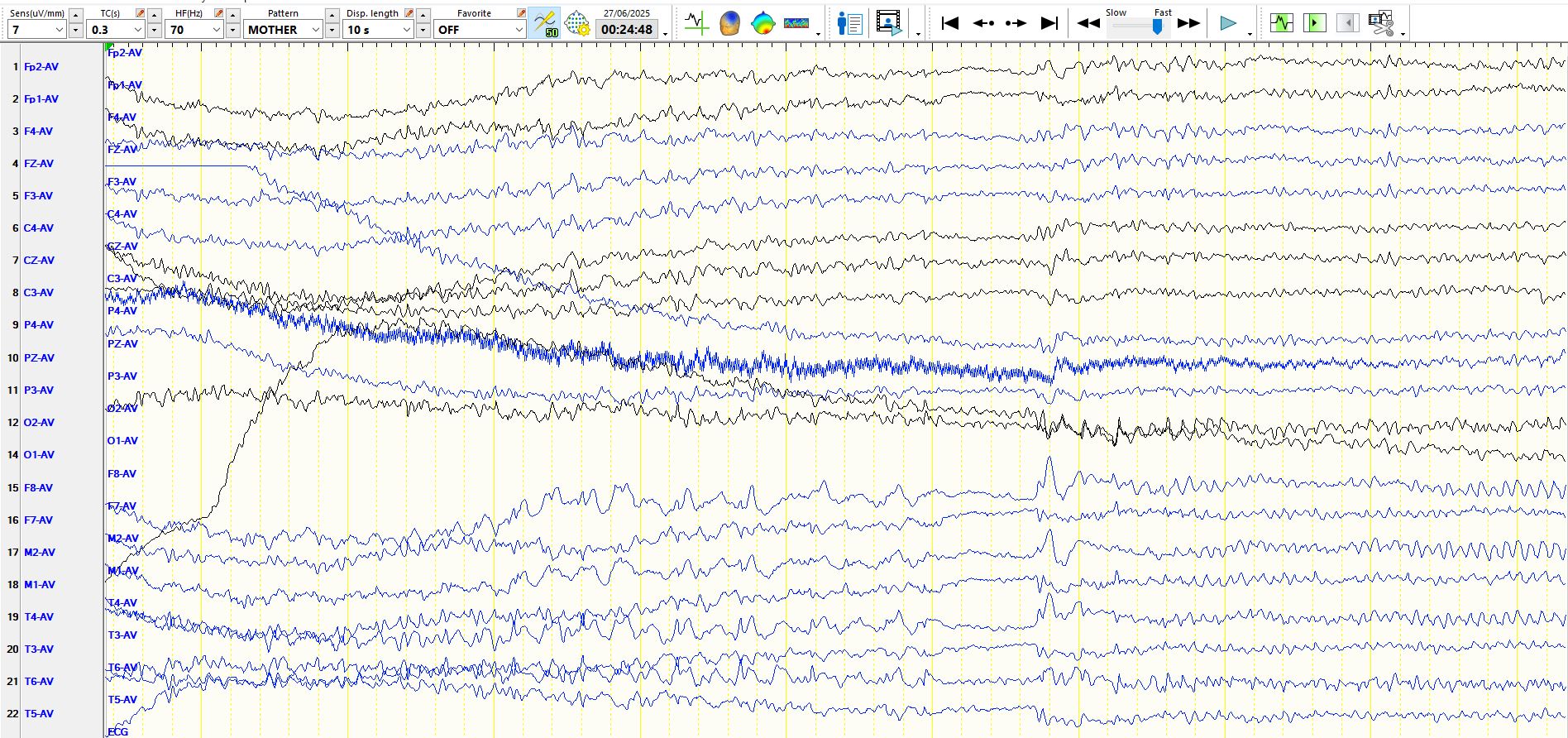
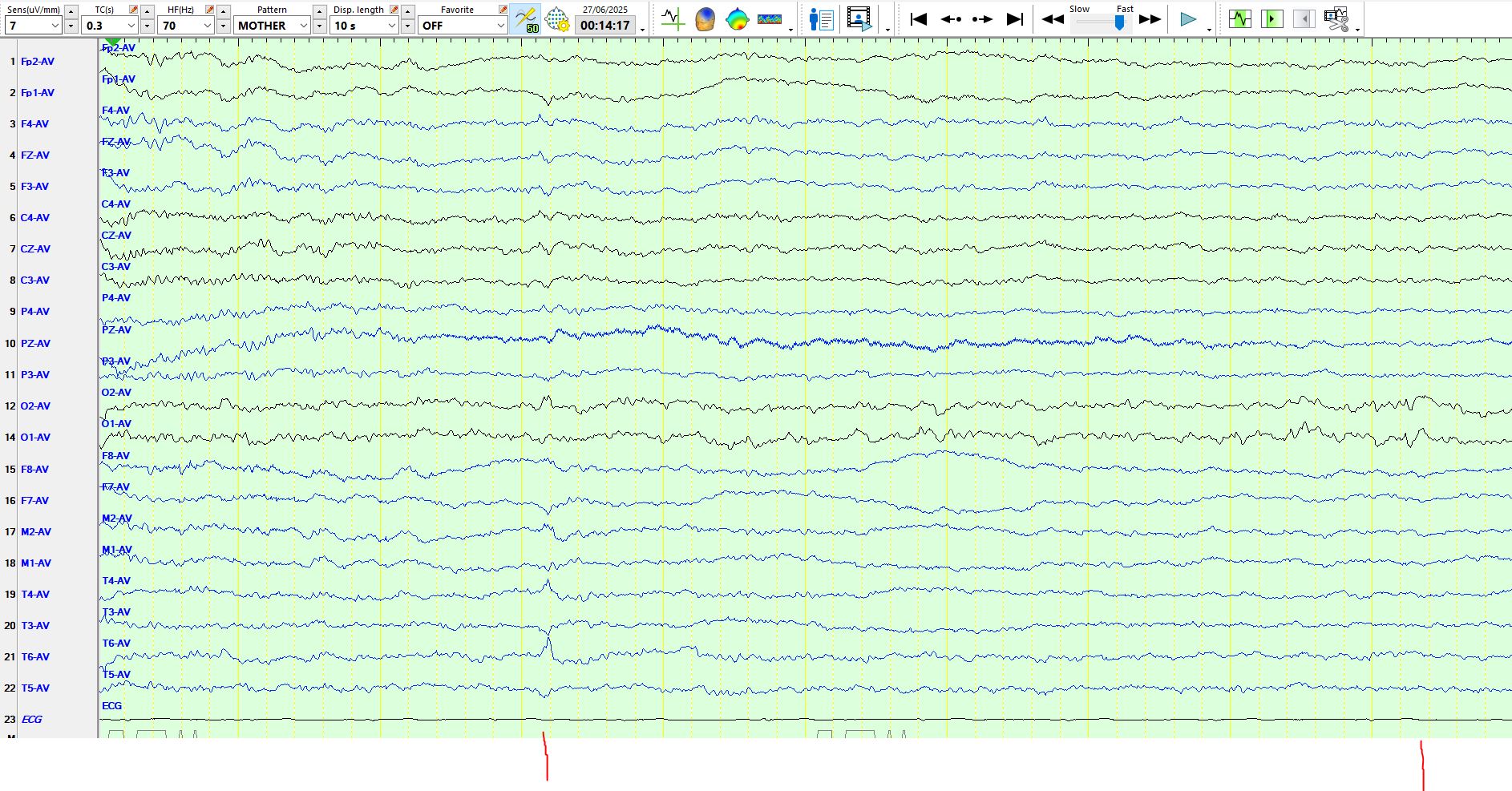
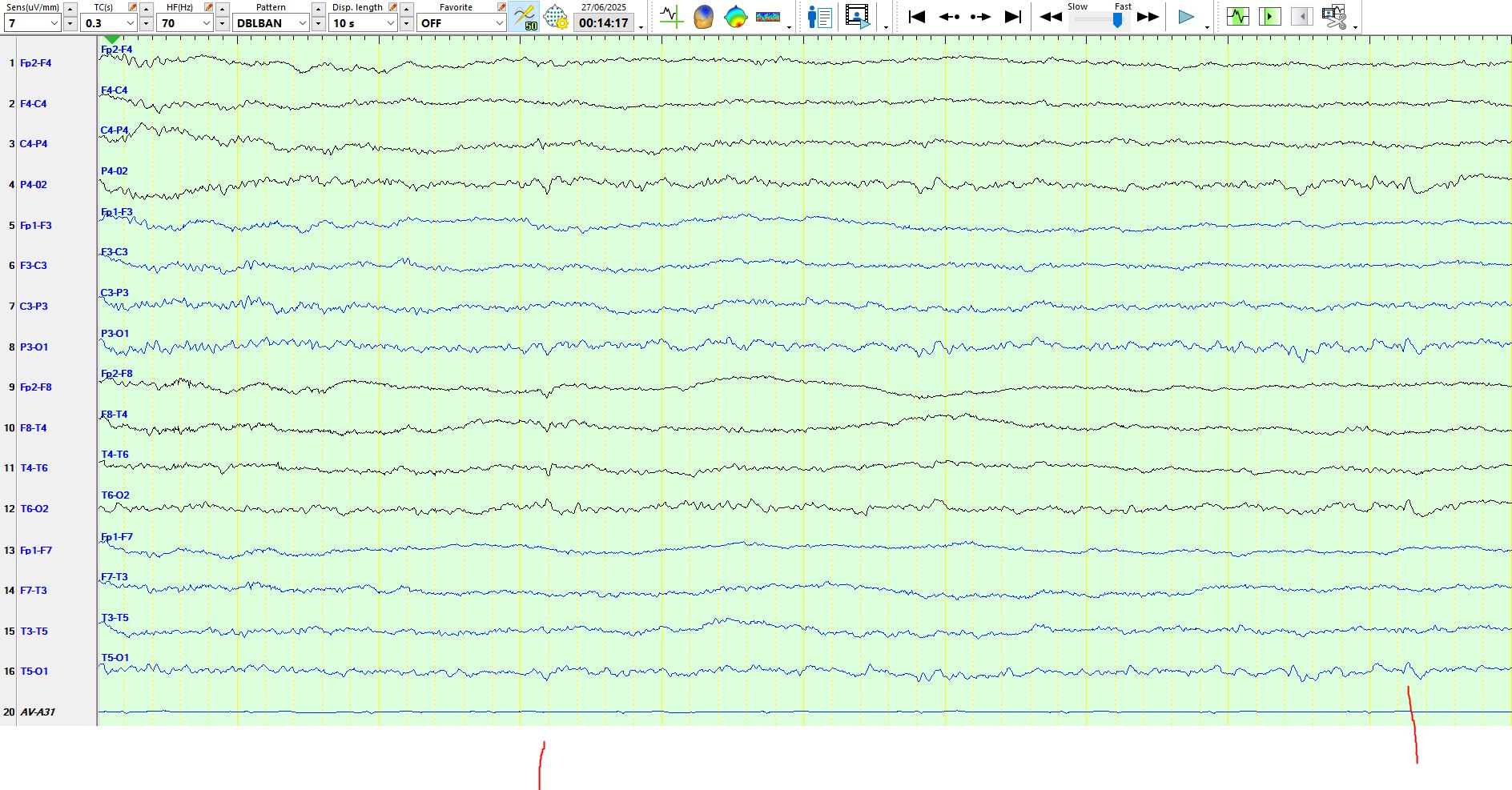
The patient subsequently had several seizures, each lasting approximately one minute, originating from the same area (T6-T4) and propagating to the right anterior, inferior temporal region (F8-M2). The following are two sequential pages. The first red line corresponds to a probable Inter-ictal epileptiform discharge at T6-T4 and the second identifies the start of the seizure as a faster frequency discharge at T6-T4. The patient had numerous subclinical seizures (neither the patient, fellow patients, the nurses recognised the seizures)