
27, clinical diagnosis: probable dominant hemisphere TLE
Jun 10, 2025The following are the same page represented on 3 different montages
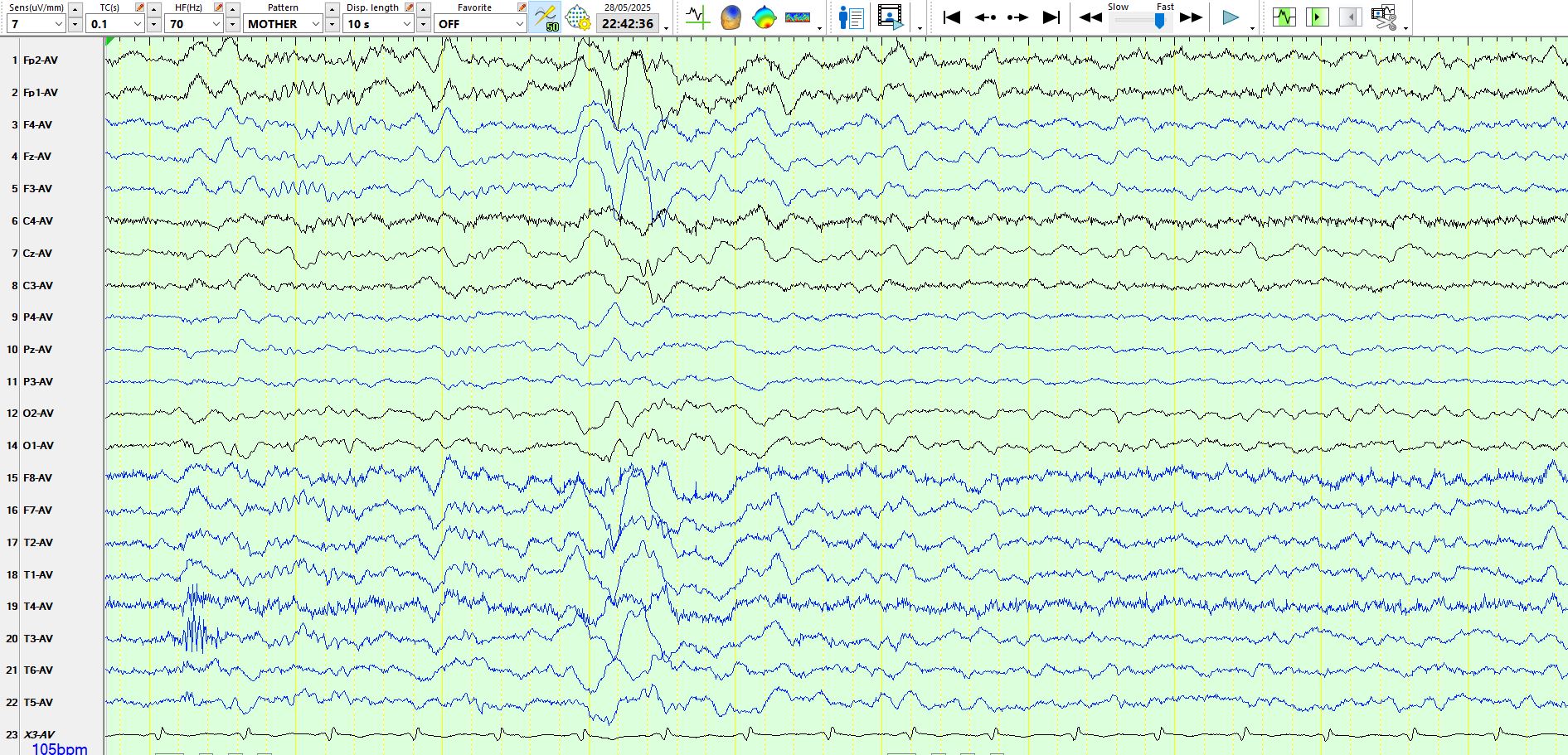
Referential montage
Bipolar AP montage:

Coronal montage:

While the above resembles spike-and-wave during sleep, the apiculate wave occurs bilaterally and approximately symmetrically on referential montage, raising the possibility of an F-wave, followed by a slow wave in sleep. This likelihood is markedly increased by the virtual disappearance of the same wave on the bipolar AP and coronal montages. I have a golden rule that I avoid calling waves spikes that cannot be seen in at least 2 different montages and are unambiguous on both. Then there is the question of reproducibility, field, morphology, exclusion of physiological waves and artefacts.
The following two images represent the same page on 2 different montages:
Referential montage
The above is of interest as the field of the spike differs somewhat from the slow wave. This likely is a spike preceding the slow wave, as the discharge is very sharply contoured, does not have the morphology and distribution of a physiological wave in sleep (the distribution is not typical of a small sharp spike), it has a typical field of temporal spike (M1-F7-T3) and an artefact does not explain its appearance And distribution.
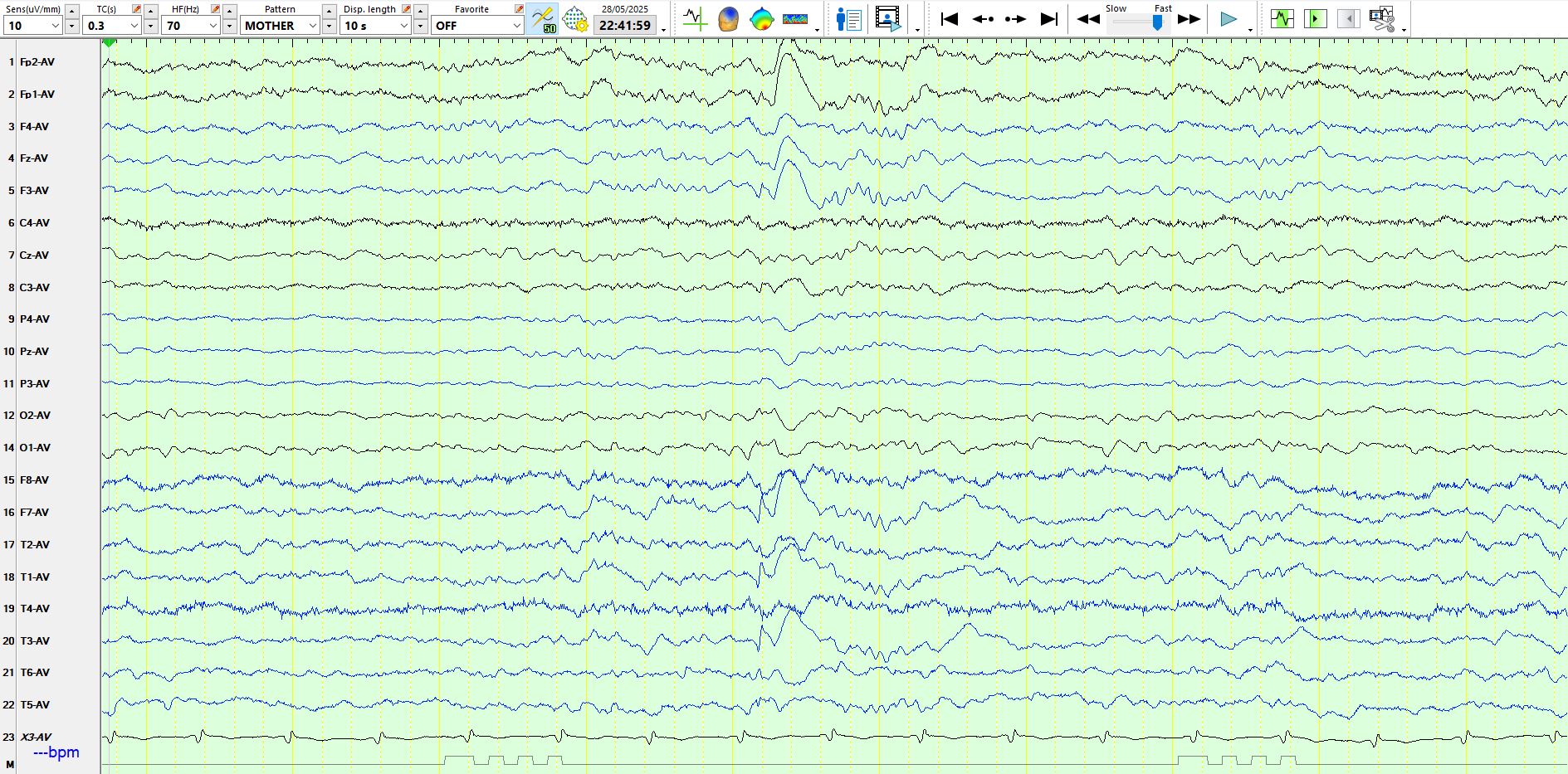
Bipolar anterior-posterior montage:


In the above image, the patient is asleep. There is an F-wave about halfway across the page. This is preceded by a biphasic spike very similar in morphology to the spike-and-wave that occurs on the image 2 slides up. It is located at F7-FP1-F3. While it resembles a small sharp spike in morphology, its distribution is atypical of a small sharp spike. Its association with a delta wave in the next 2 slides above further increases the certainty that this represents a spike rather than a small sharp spike. It is clearly reproducible and is not explained by an artefact. The idea of reproducibility is important in EEG as it is in science (of course artefacts and physiological waves might also look the same), so reproducibility is but one criterion. But there is more...

The above is a spike/sharp wave, depending upon whether you look FP1 or at F7. It has a field, is not part of the background and is not a wicket wave in the temporal region, given its strong expression at FP1-F3 and the above wave is therefore further evidence for inter-ictal epileptiform discharges over the left anterior temporal/lateral frontal region/prefrontal region (more about that below). Notice that this sharp wave is also followed by an F-wave that is bilaterally symmetric.

In the above there are 2 sequential delta waves at F7-M1-T3-FP1





MRI shows a probable left temporal pole encephalocoele; histology of the left temporal pole and hippocampus to follow