21y, Right-handed, Episodic visual symptoms
Jun 12, 20254-year history. Once or twice a year, "I would lose peripheral vision" (bilaterally), "objects would look crystallized" and then in some "I could not read, the words appeared jumbled" and others noticed that when she spoke, she did not make sense. She reported difficulties with finding her words during these events but thought that she was speaking sense. The visual symptoms lasted approximately 2 hours and were followed by severe headache and nausea and fatigue. In 2025 these increased in frequency so that she was having approximately 3 per week, prompting her general practitioner to commence pregabalin 25 mg at night 3 months ago, with no cessation of the events (only one mild event since then, none for more than a month prior to this EEG).
There is a strong family history of severe migraine. Visual field testing at the bedside is normal.
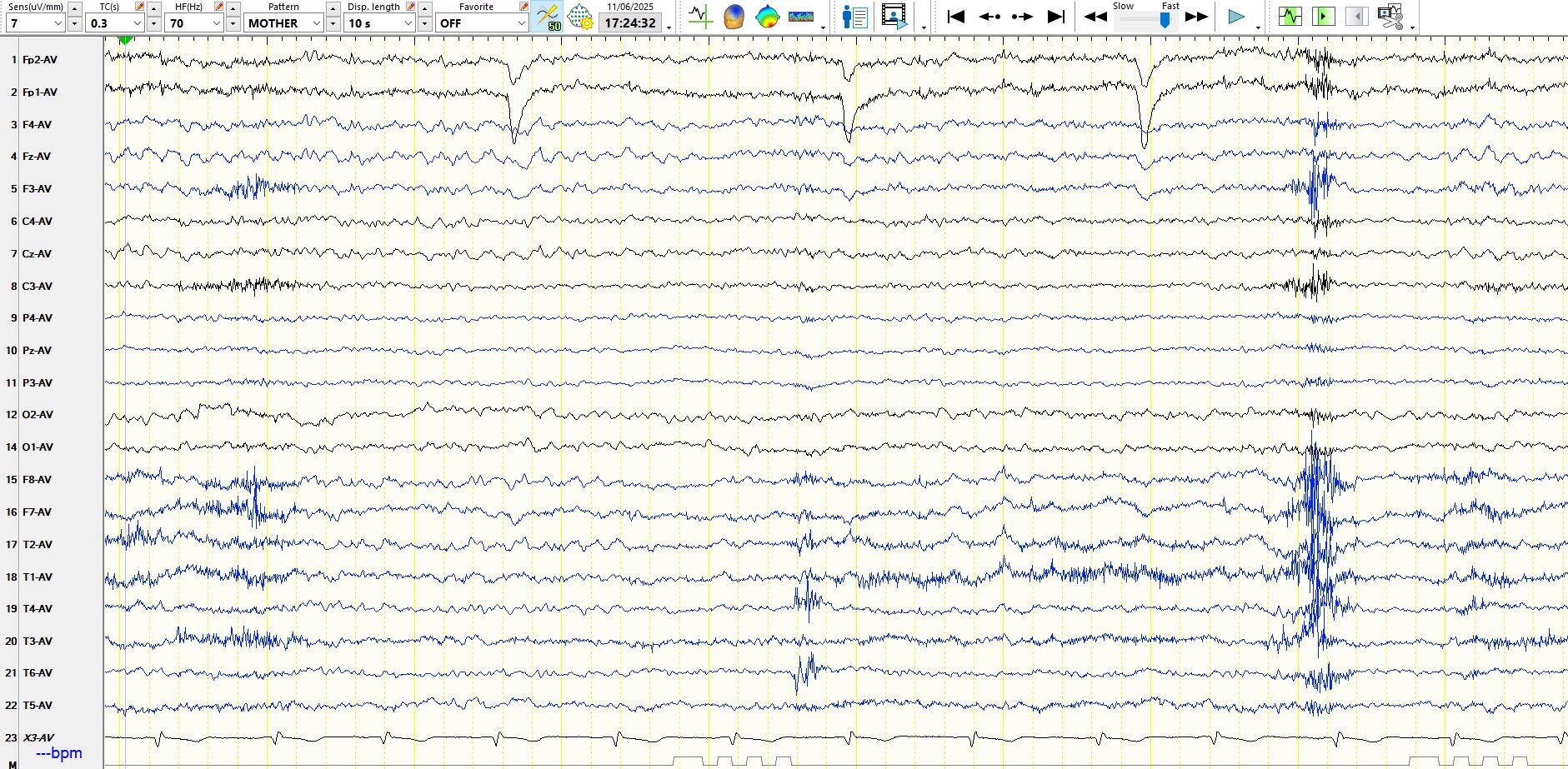
Referential montage
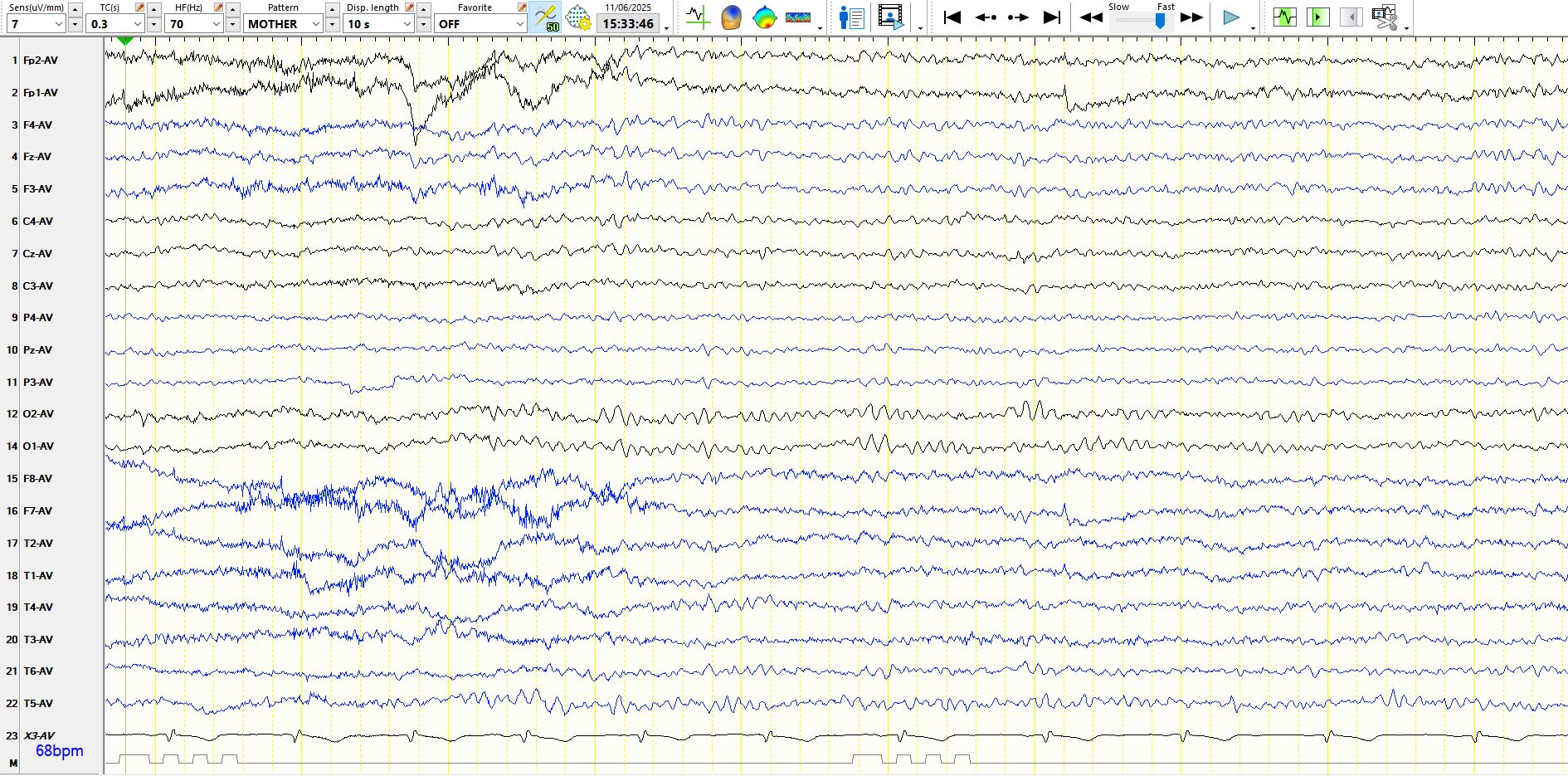
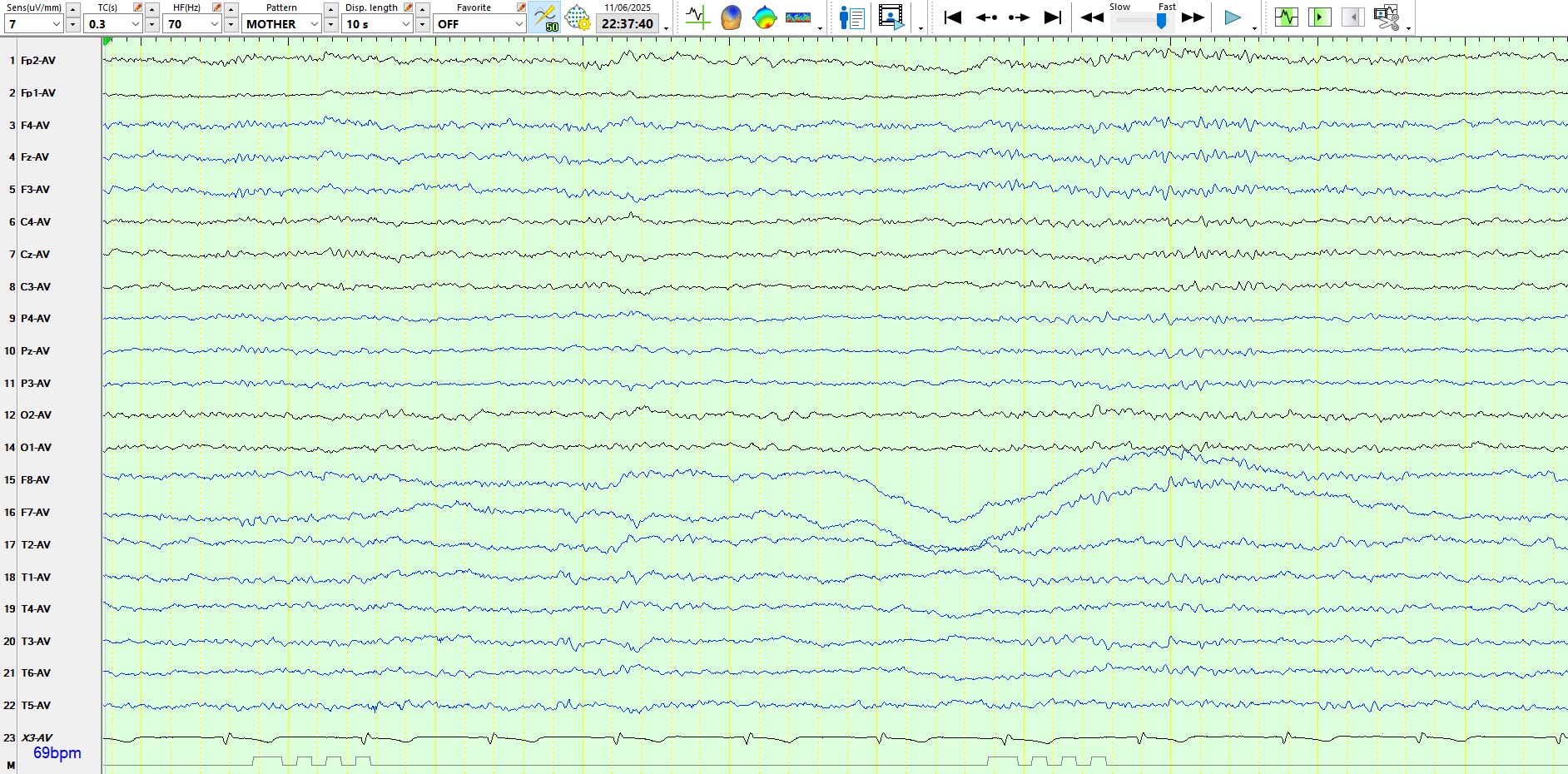
The above page is normal
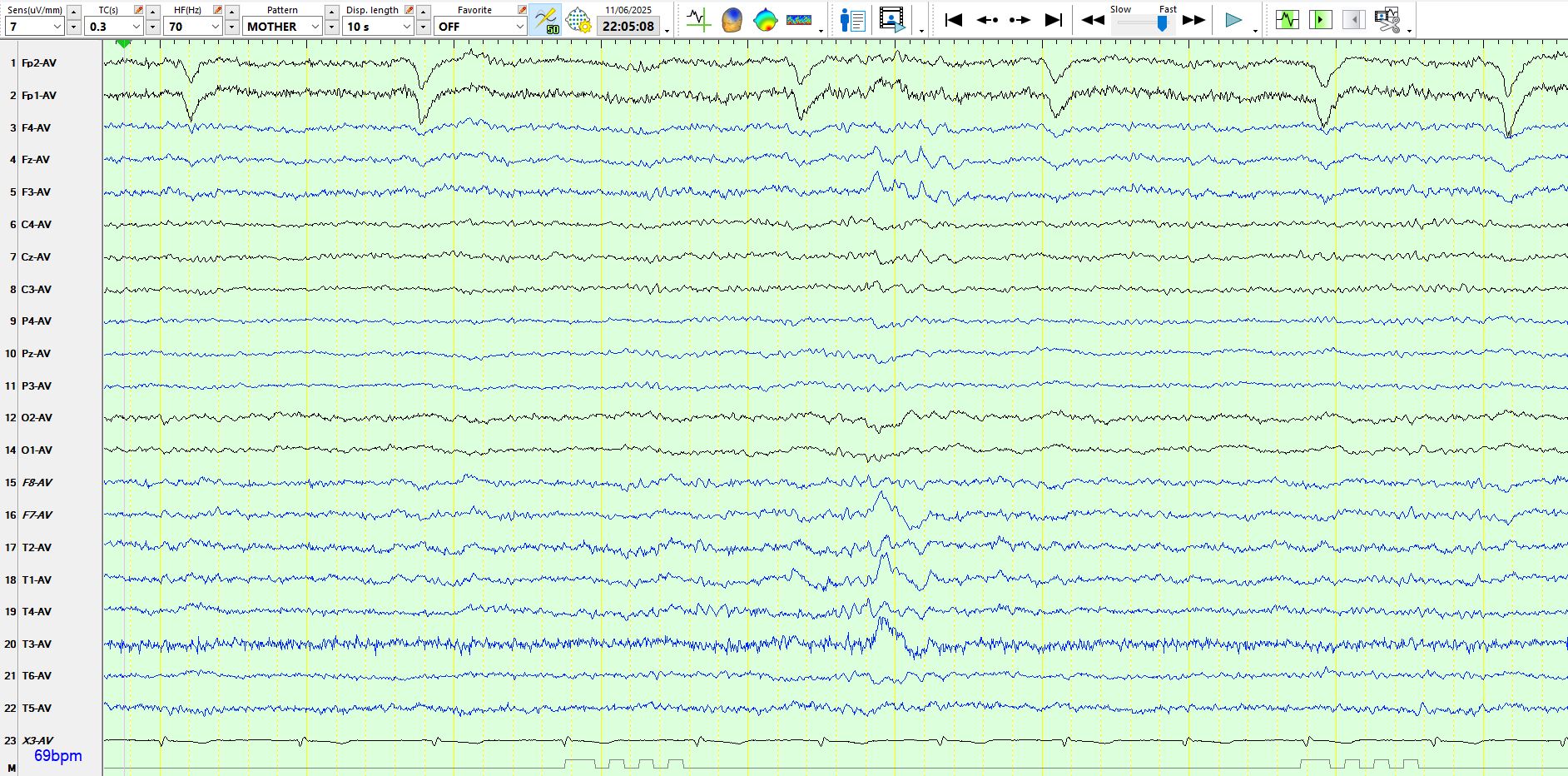
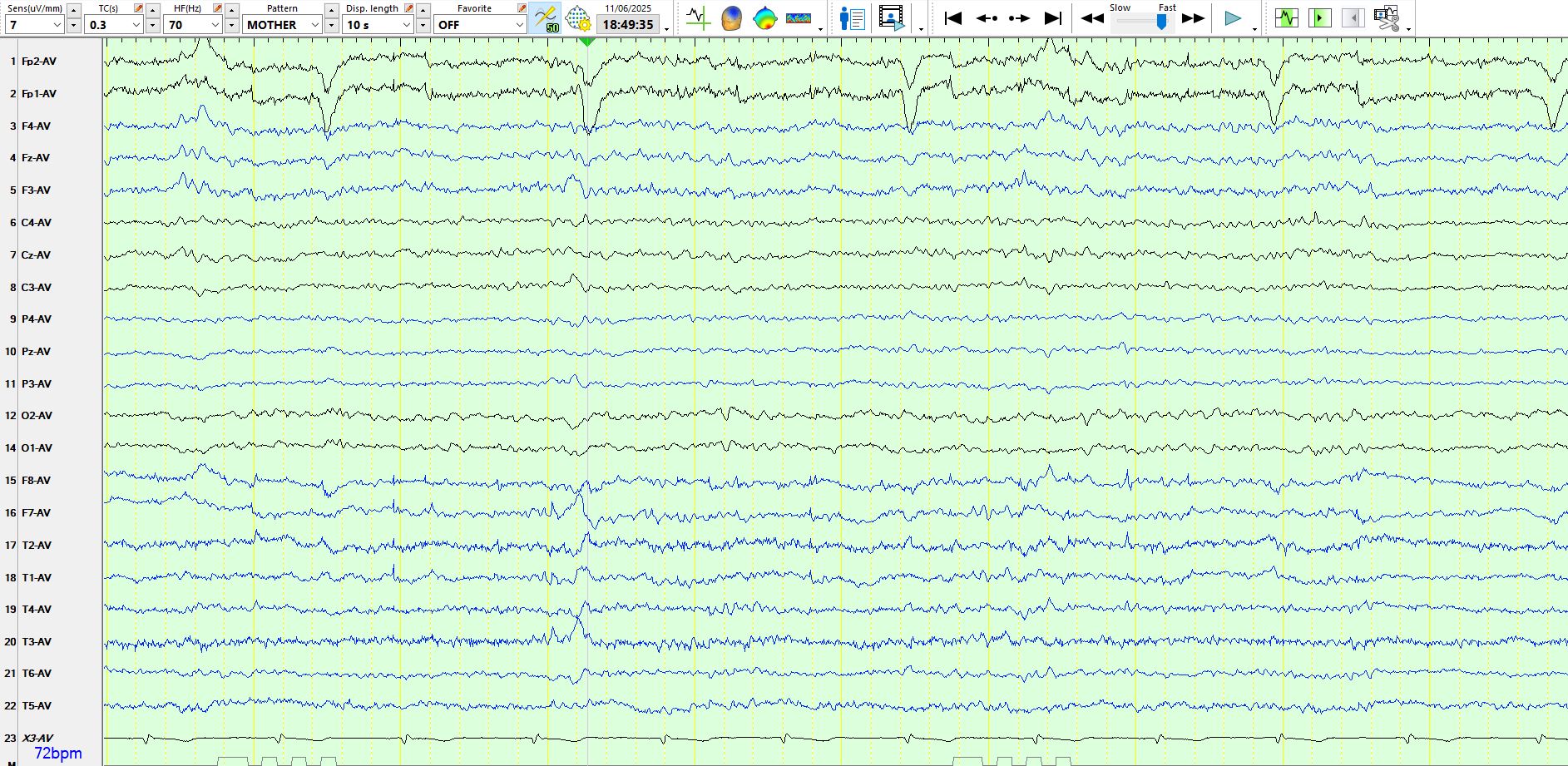
The following are 3 consecutive pages:
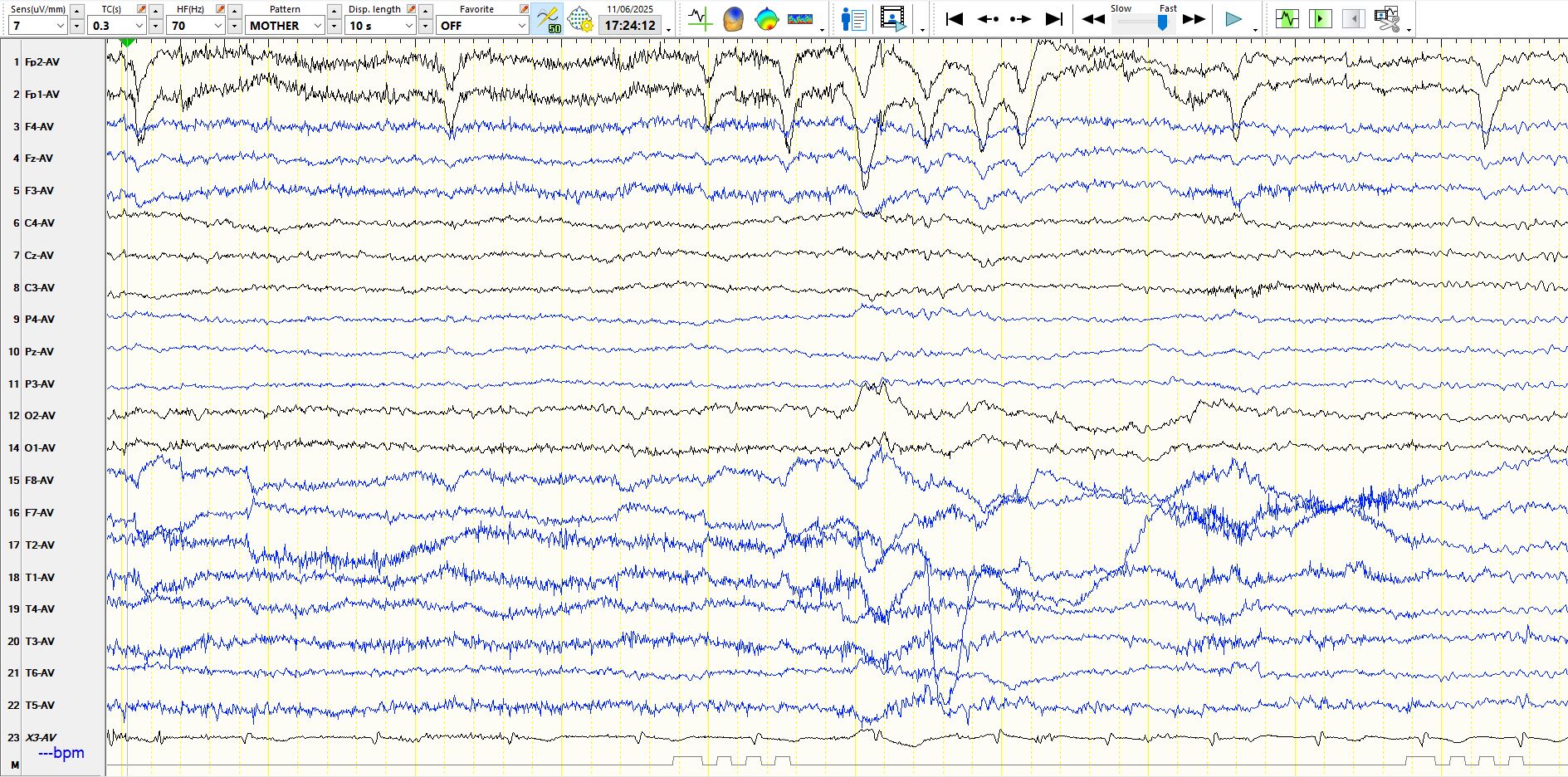
On the first page above, the patient is fully alert, with eyeblinks, EMG and normal background rhythms. On the 2nd page there continue to be eyeblinks and EMG artifact, but the presence of sagittal theta waves (FZ-CZ) is characteristic of early drowsiness and this argument is further strengthened by the presence of theta waves in the temporal regions during the 7th-10th seconds above, at which time EMG also diminishes
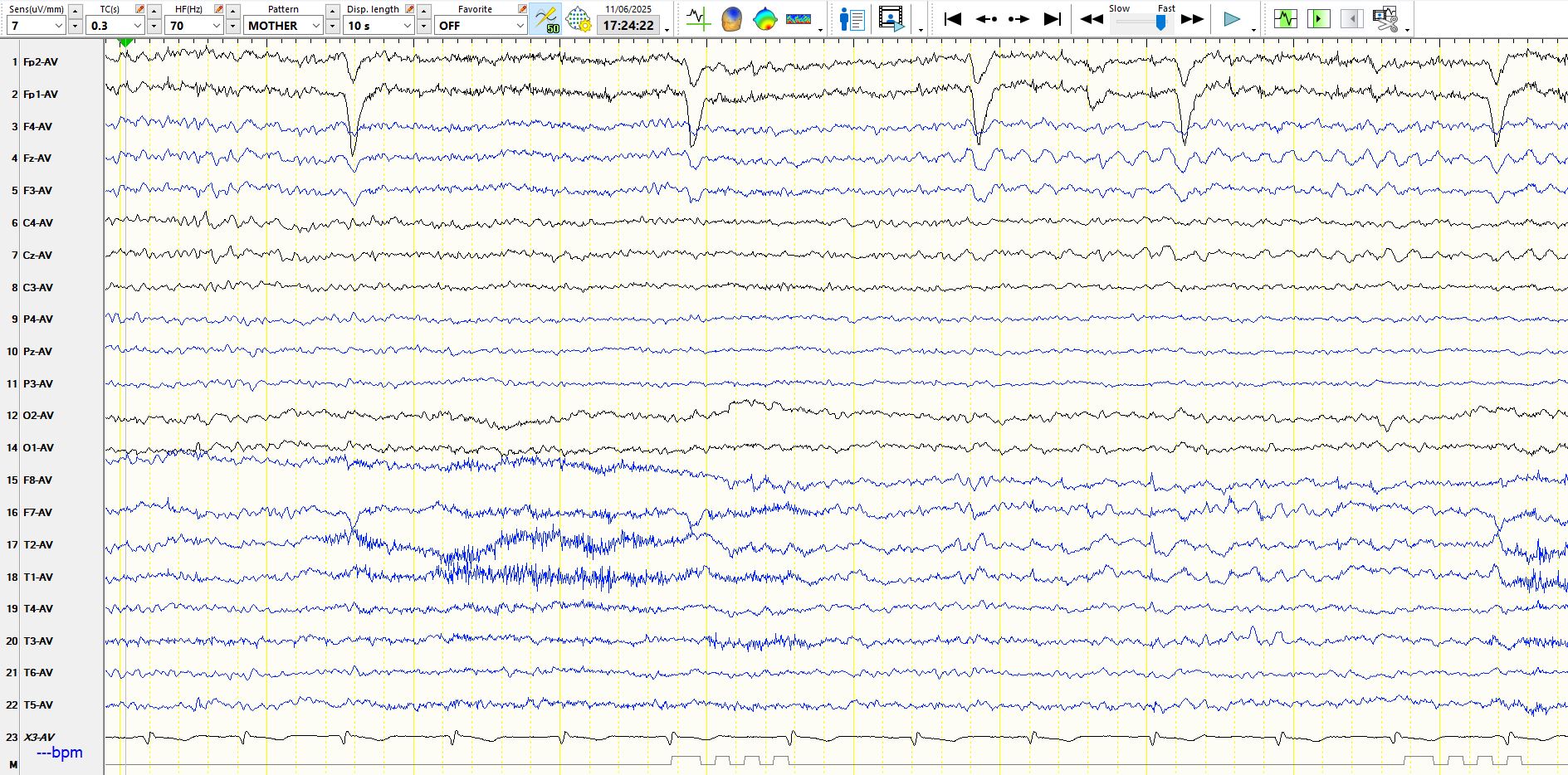
The same page as above, the bipolar AP montage (below)
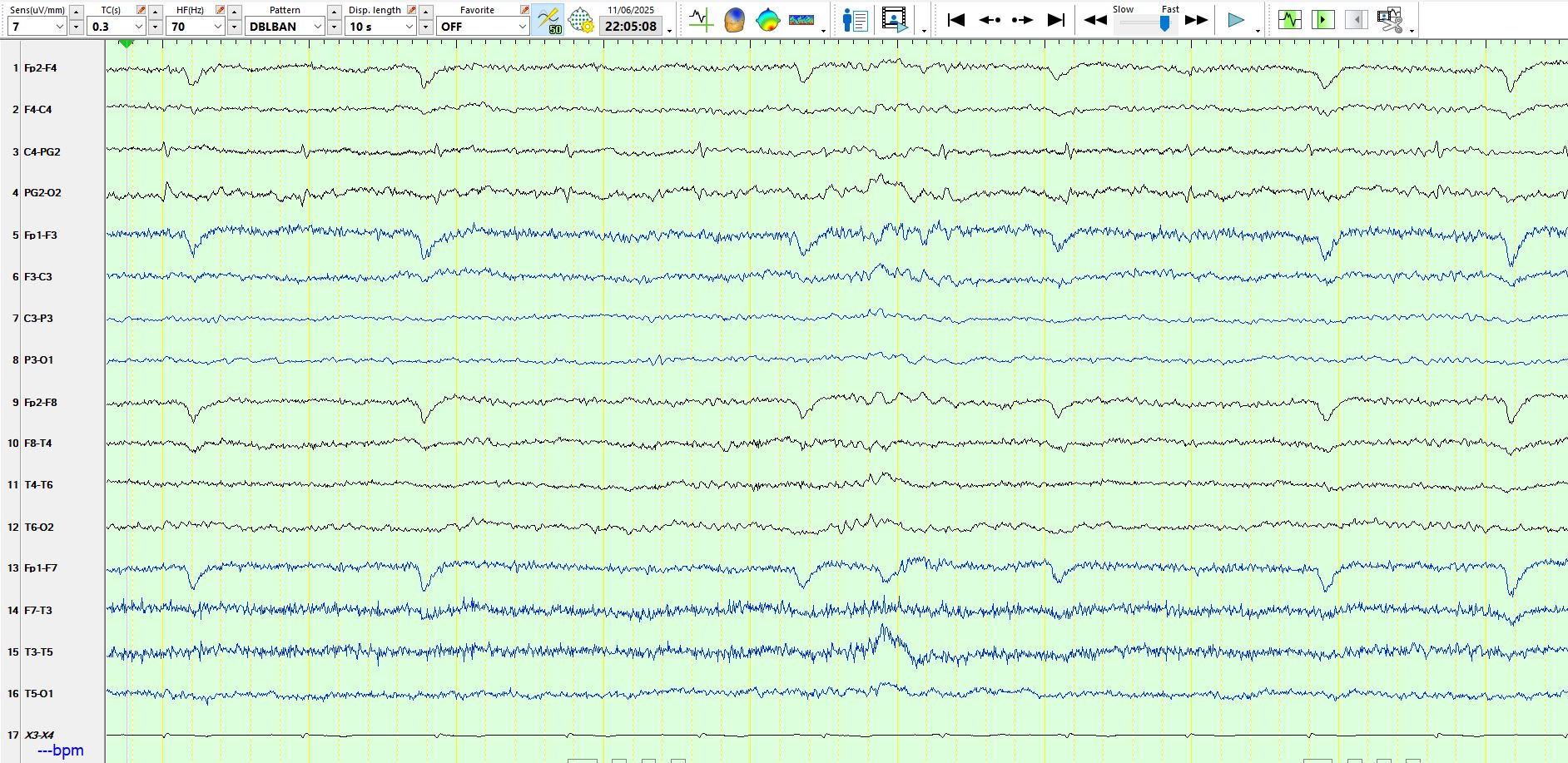
There is a delta wave at F7-T3, barely involving M1 and therefore reflecting neocortical temporal dysfunction, rather than "inferior temporal" dysfunction
3 consecutive pages:
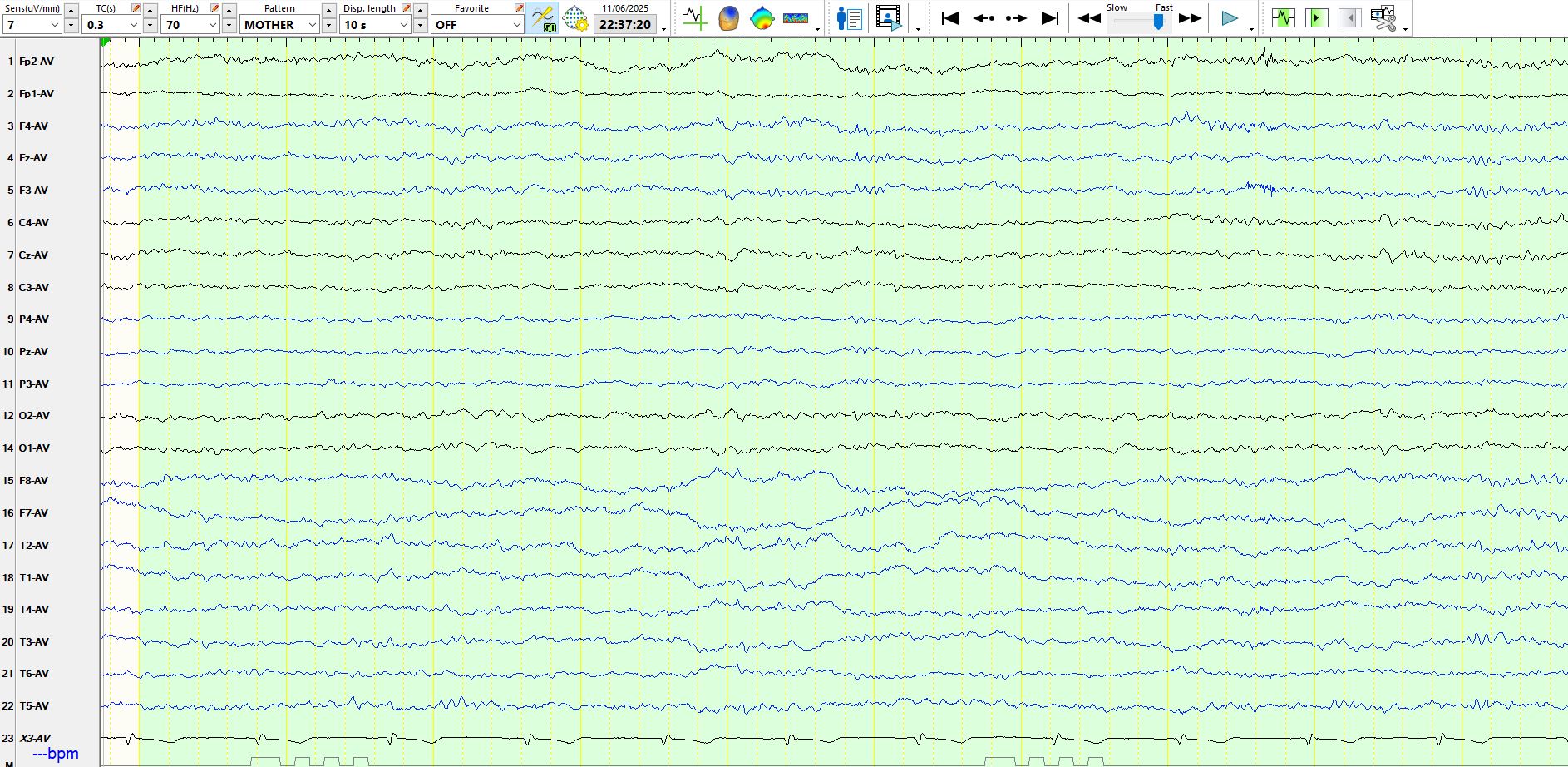

In the middle page there is a delta wave at T3-F7 during stage I sleep
Theta wave at F7-T3 while awake (above)
The patient had no more than a few left temporal theta and delta waves. Nevertheless, these are abnormal.
EEG in migraine: a review of the literature - PubMed
Bottom line
1. The EEG may be abnormal in people with migraine
2. The location of the non--epileptiform dysfunction on EEG in the above patient, remote from the time of the most recent migraine, is anatomically congruent with migraine that involves the occipital and left posterior peri-Sylvian region. This association likely is not coincidental. Electrode T3 Is the closest electrode to Wernicke's Area.
3. Non-epileptiform dysfunction has various causes. While finding is non-specific, it is nevertheless abnormal.
PS Is the duration of the above aura atypical?
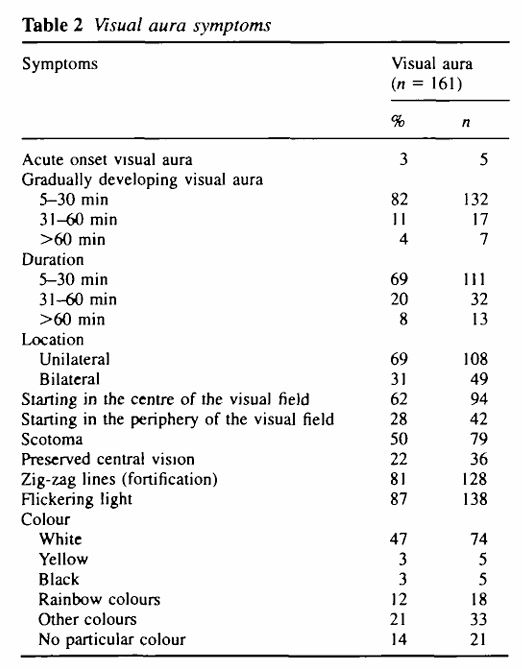
A nosographic analysis of the migraine aura in a general population - PubMed