21y, first seizures
Jun 04, 2025She developed her first neurological event four days ago, when she got up, felt dizzy and heard a high-pitched ringing sound, her vision appeared slightly blurred, she became an amnestic, regained her memory while leaning on the windowsill and recovered with no residual symptoms
Three days later she awoke at 01:00 with mild nausea followed by a high-pitched, ringing sound. She was then aware of her head being tonically being pulled to the left, she was then aware of her arms and legs shaking, she was then amnestic and her family report bilateral shaking of the limbs. Post-ictally she was "lightheaded and felt weird". Her family noted that she was slurred and unsteady, but her use of language was normal.
Two minutes later she had an identical seizure to the above. She recalls the same high-pitched ringing sound and tonic deviation of the head to the left, followed by a similar seizure. Post-ictally she felt tired and sluggish; this recovered gradually over about 24 hours.
The 20 minute EEG recording was normal
An overnight EEG was performed. What type of epilepsy do you think she has?
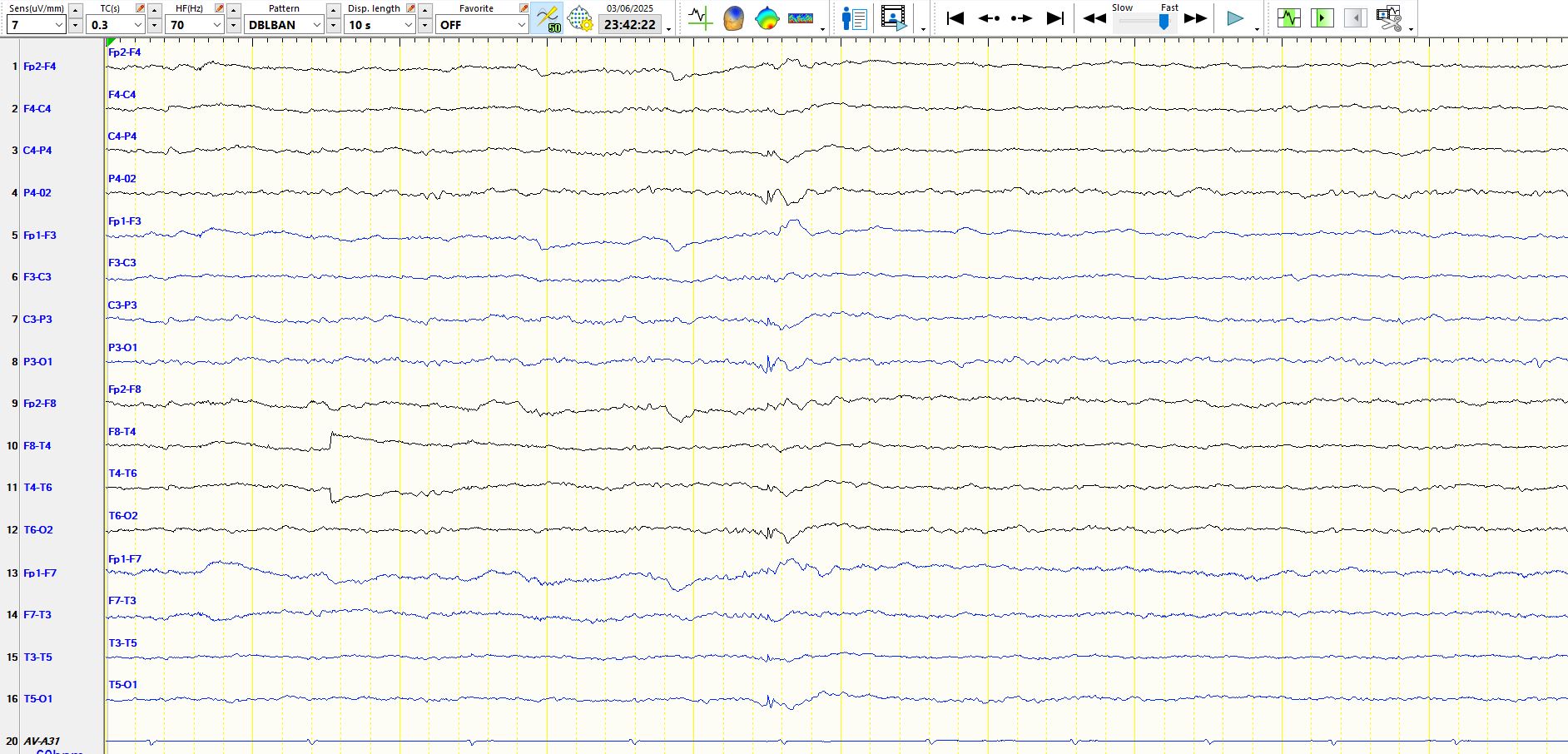
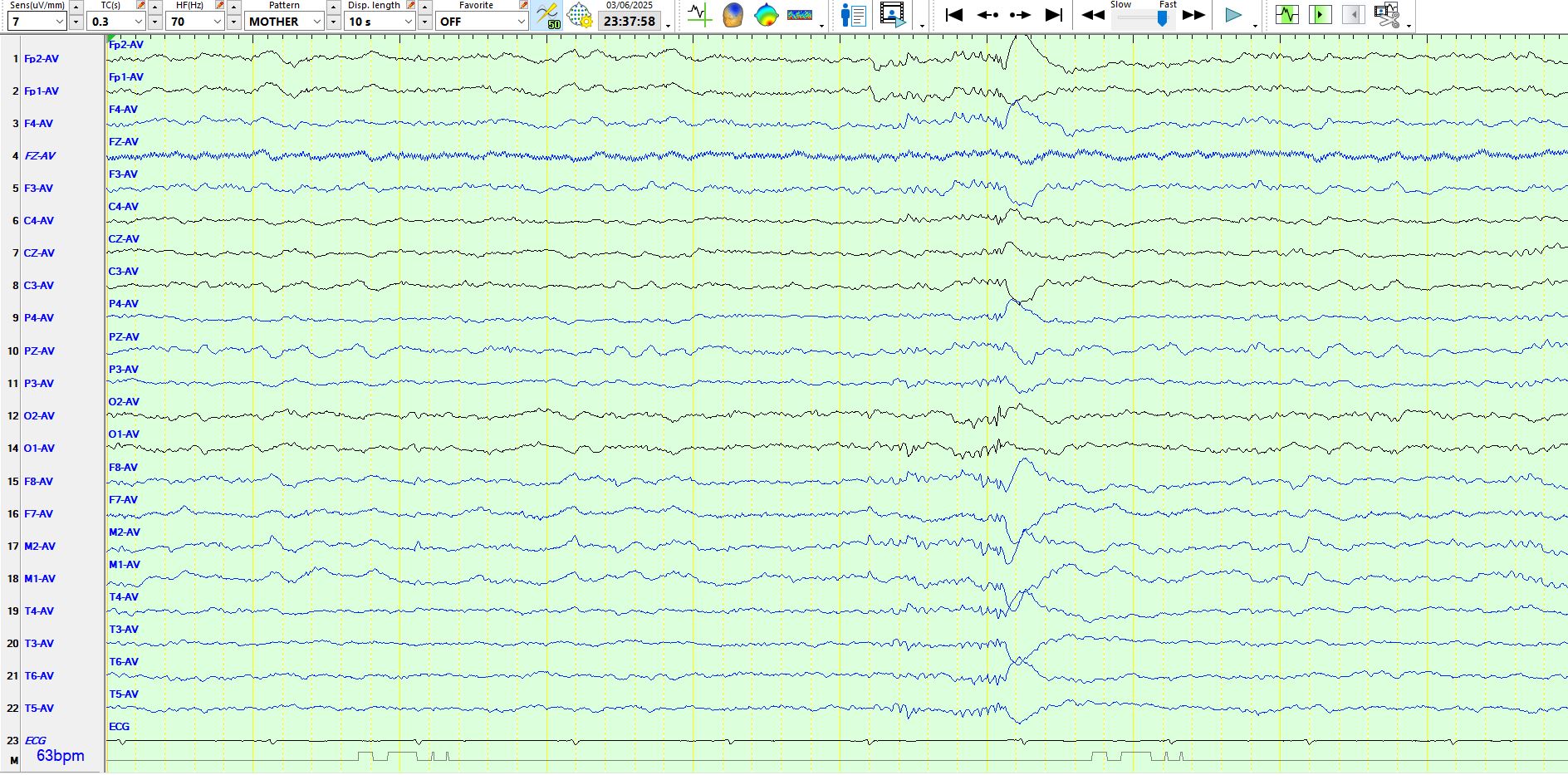
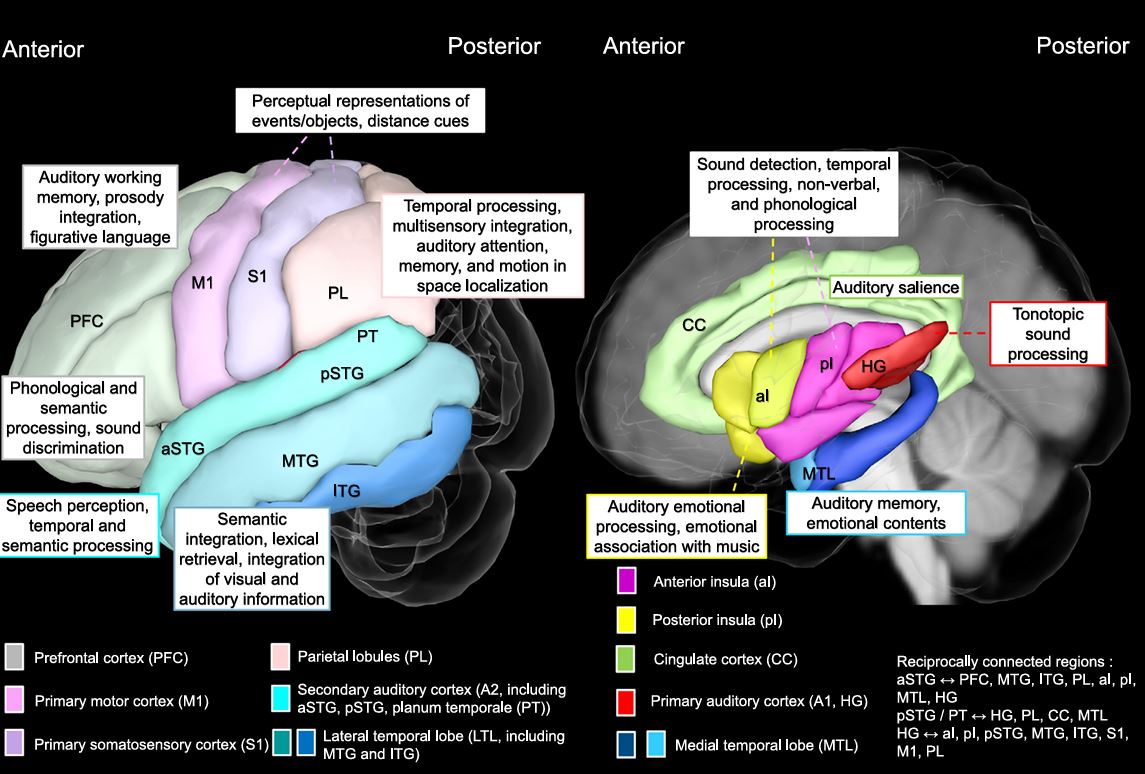
The above pages demonstrate that the patient is asleep. The apiculate, generalised, occipitally-predominant wave appears to be a spike and wave when viewed on the bipolar montage, but the frequency here is important and is in excess of 5 Hz. You will also notice the low amplitude monorhythmic waveform just preceding it. When viewed on the preferential montage the arciform nature of this discharge is apparent and has the typical morphology, frequency and amplitude of the 14 Hz component of 14- and 6-Hz postive bursts. This is therefore a normal variant.
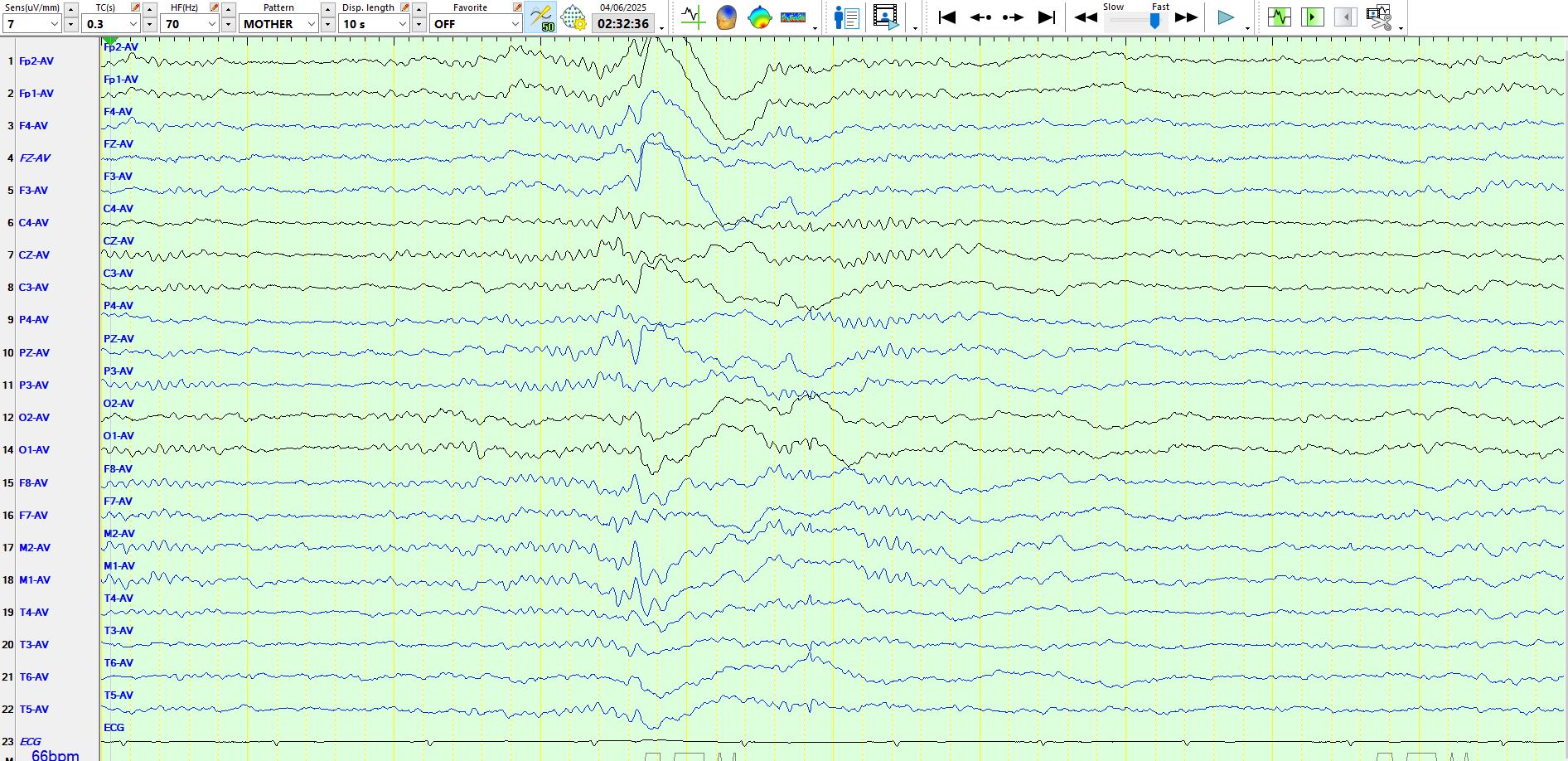
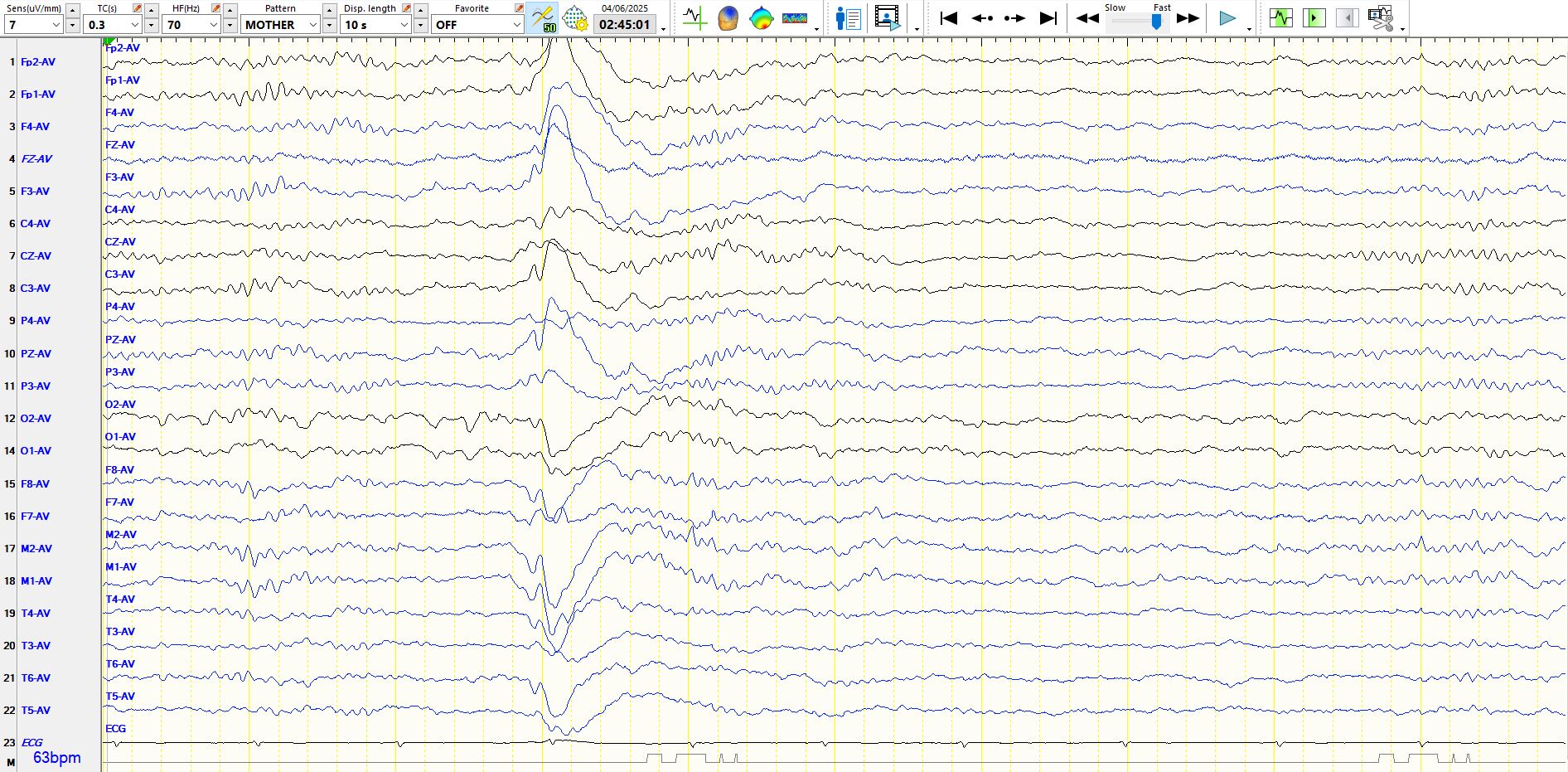
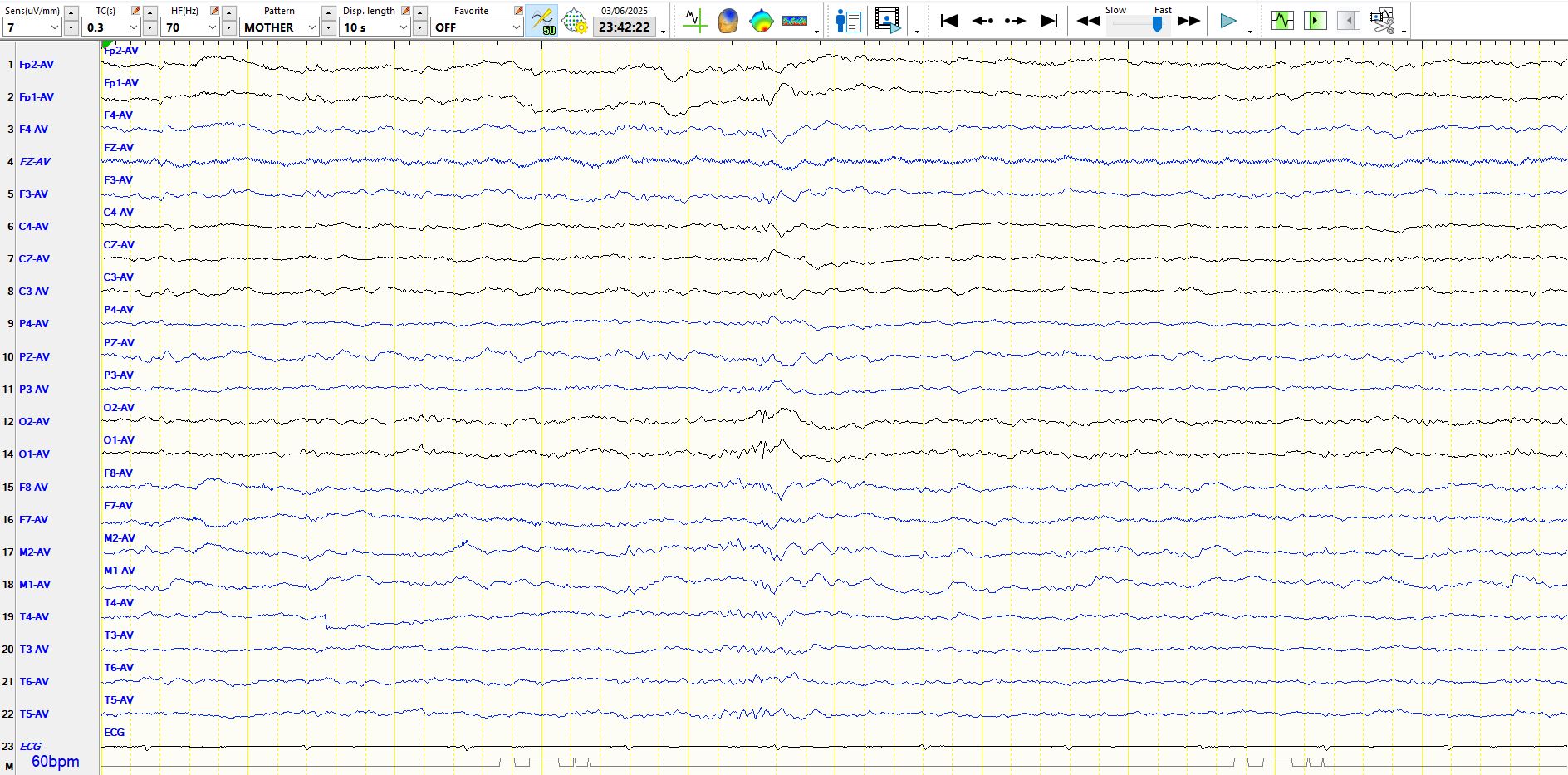
These are typical K-complexes, defining stage II sleep. In referential montages they may sometimes be confused with slow spike-and-wave but the distribution and morphology are characteristic and in this instance there is an after-coming spindle, as is characteristic of K-complexes. Recall that K-complexes have initial short negative component, followed by an electropositive component and then a final electro-negative component. On scalp EEG they may appear biphasic or triphasic. This again is a normal variant. You can read a little more about them here:
The human K-complex: Insights from combined scalp-intracranial EEG recordings - ScienceDirect
In this instance version of the head to the one side at the start of a seizure is reliably indicative of contralateral frontal involvement. This is not to say that the seizure started on the frontal lobe, but the retained awareness indicates that the seizure is still relatively spatially restricted, even if it has propagated from insular cortex or frontal or temporal operculum. The EEG demonstrated no spikes, while the MRI demonstrates evidence of a right frontal developmental venous anomaly. These are relatively common coincidentalomas; I have yet to see one associated with the region of seizure onset (symptomatology and electrophysiology have always indicated otherwise), but this one may be causally related. There is precedent for this, albeit rare.
Epilepsy and cerebral developmental venous anomalies (DVAs): A systematic review - PubMed
MRI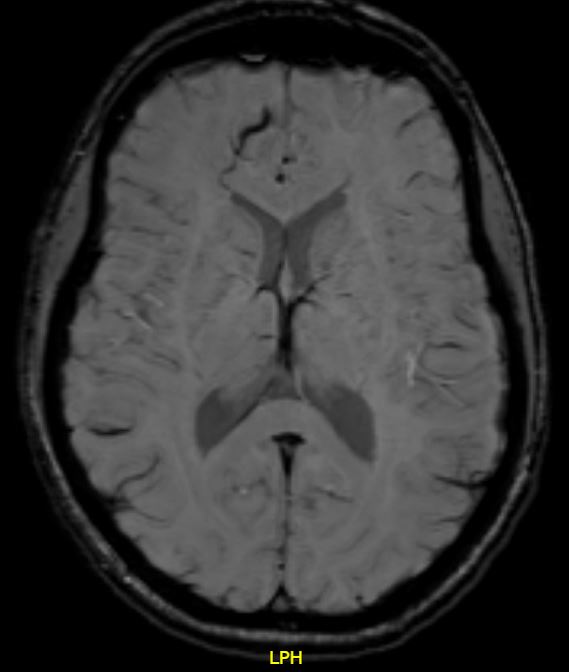
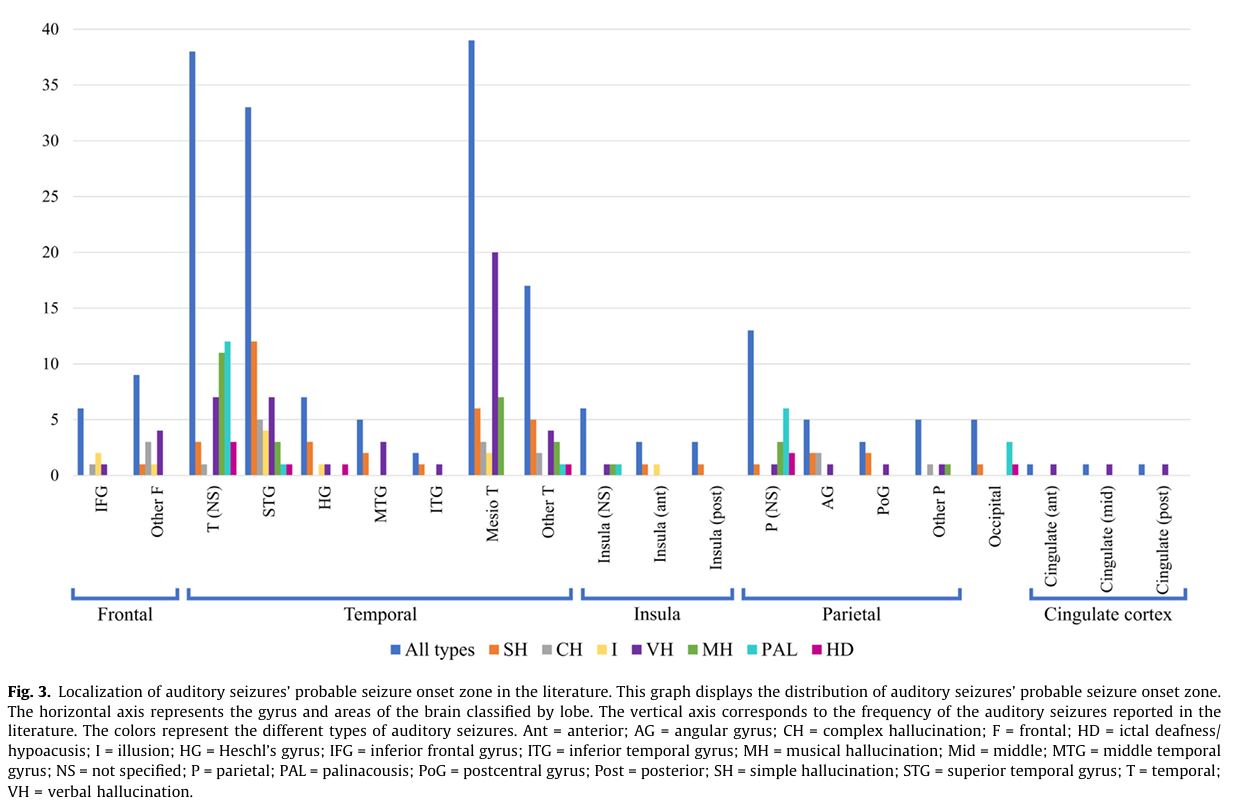
The high pitched sound, characteristic of a Heschl's gyrus onset, is undoubtedly sometimes seen in patients with frontal lobe epilepsy. If it is the former, then there is an alternative cause, perhaps a focal cortical dysplasia or a genetic cause. I vividly recall a patient with left anteromedial frontal lobe epilepsy who used to hold her ears, kick and scream and reported a noise; her MRI was normal. Scalp EEG was normal ictally and interictally and the seizures were eventually located with intracranial electrodes; she had surgery for this and has been seizure-free for many years.
Auditory aura in frontal opercular epilepsy: sounds from afar - PubMed
Localizing and lateralizing value of auditory phenomena in seizures - PubMed
The precise physiology of these extra-temporal auditory auras is unclear although one could speculate...Remember that "seizure onset zone" is a construct and that seizures need to be considered in respect of systems that are involved at onset and during the evolution of seizures
It is surprising how few cases are reported; they are not infrequently encountered in clinical practice