18y, absence seizures
Jun 19, 2025At the age of 7 years the patient developed absence seizures, with innumerable daily events characterized by brief episodes of staring and unresponsiveness, without warning and without any post-ictal symptoms (abrupt recovery). These lasted 5-10 seconds. The EEG demonstrated typical generalized 3-3.5 Hz spike-and-wave discharges. Lamotrigine and sodium valproate were without benefit, while levetiracetam caused moodiness, prompting its discontinuation. The patient was started on ethosuximide. The seizures remitted 2 years later. A few years ago, the patient was diagnosed with non-epileptic seizures, which remitted with appropriate intervention. At the age of 15 the patient had a cluster of generalized tonic-clonic seizures for the first time ever. The patient then remained seizure-free for approximately one year, while using a combination of sodium valproate and levetiracetam.
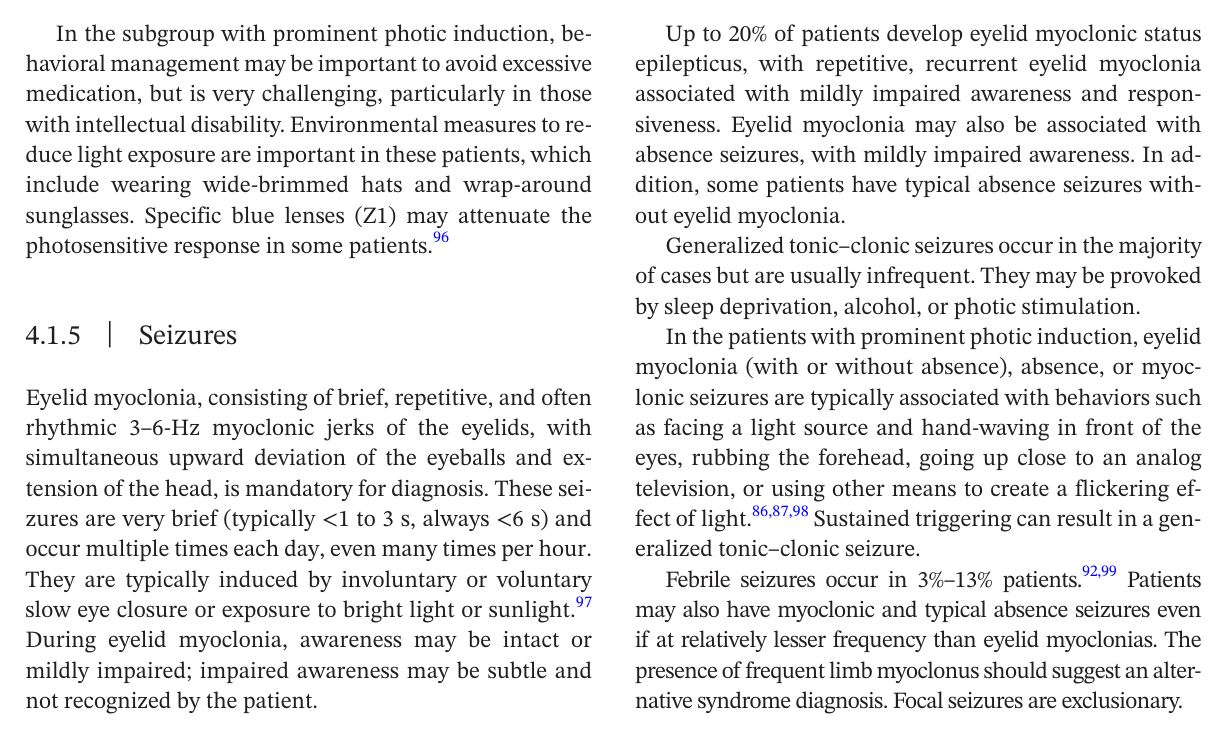
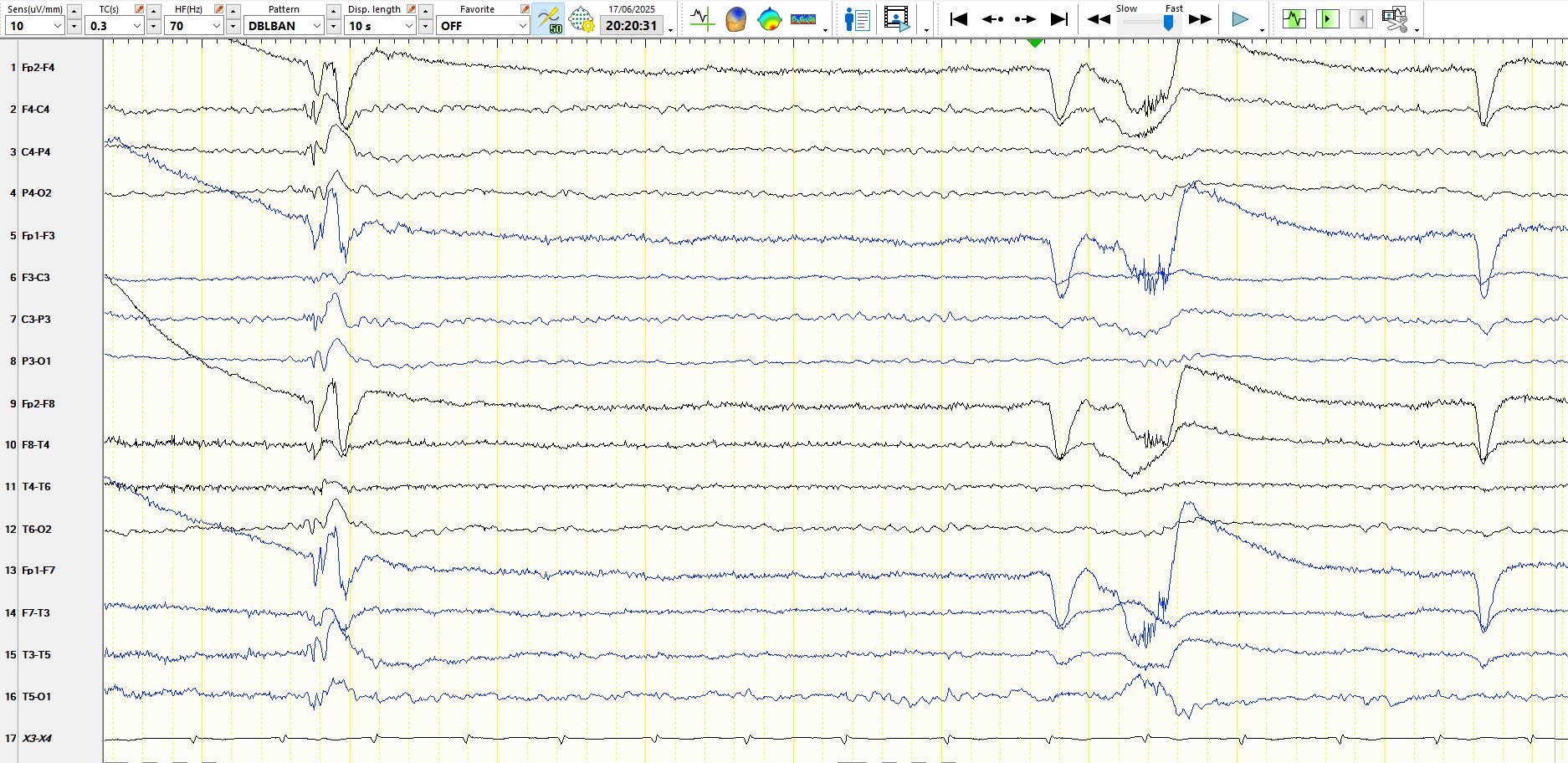
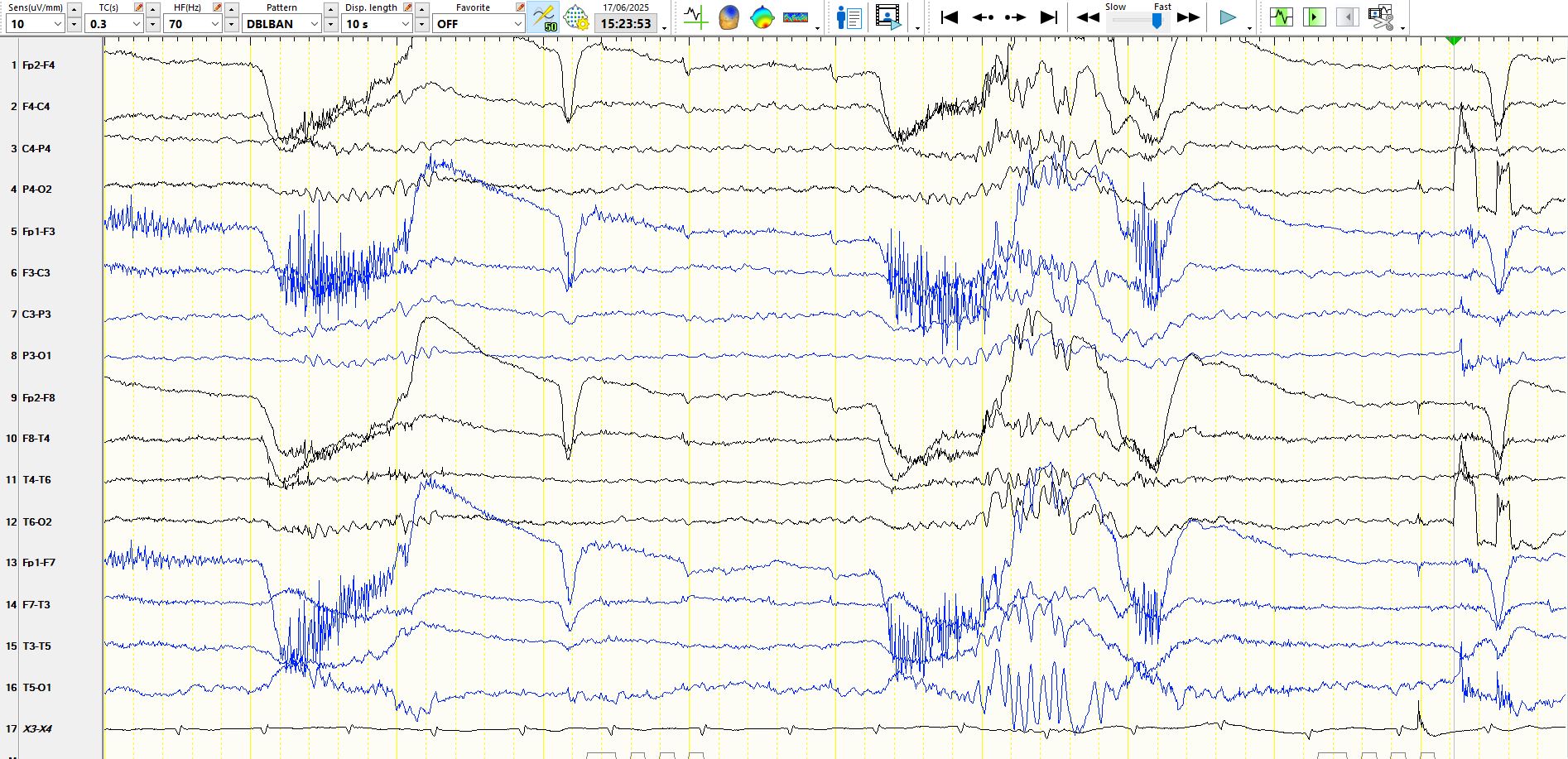
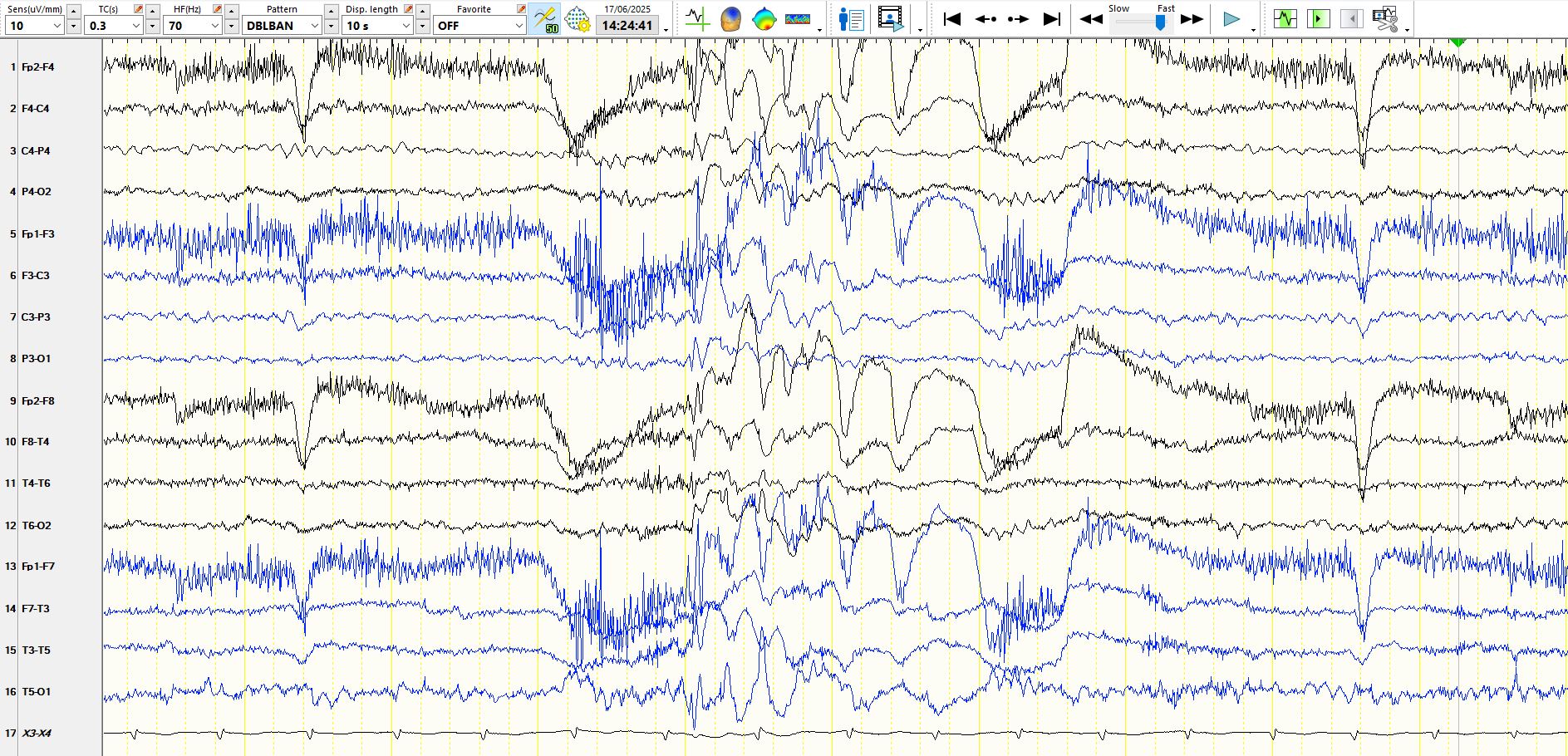
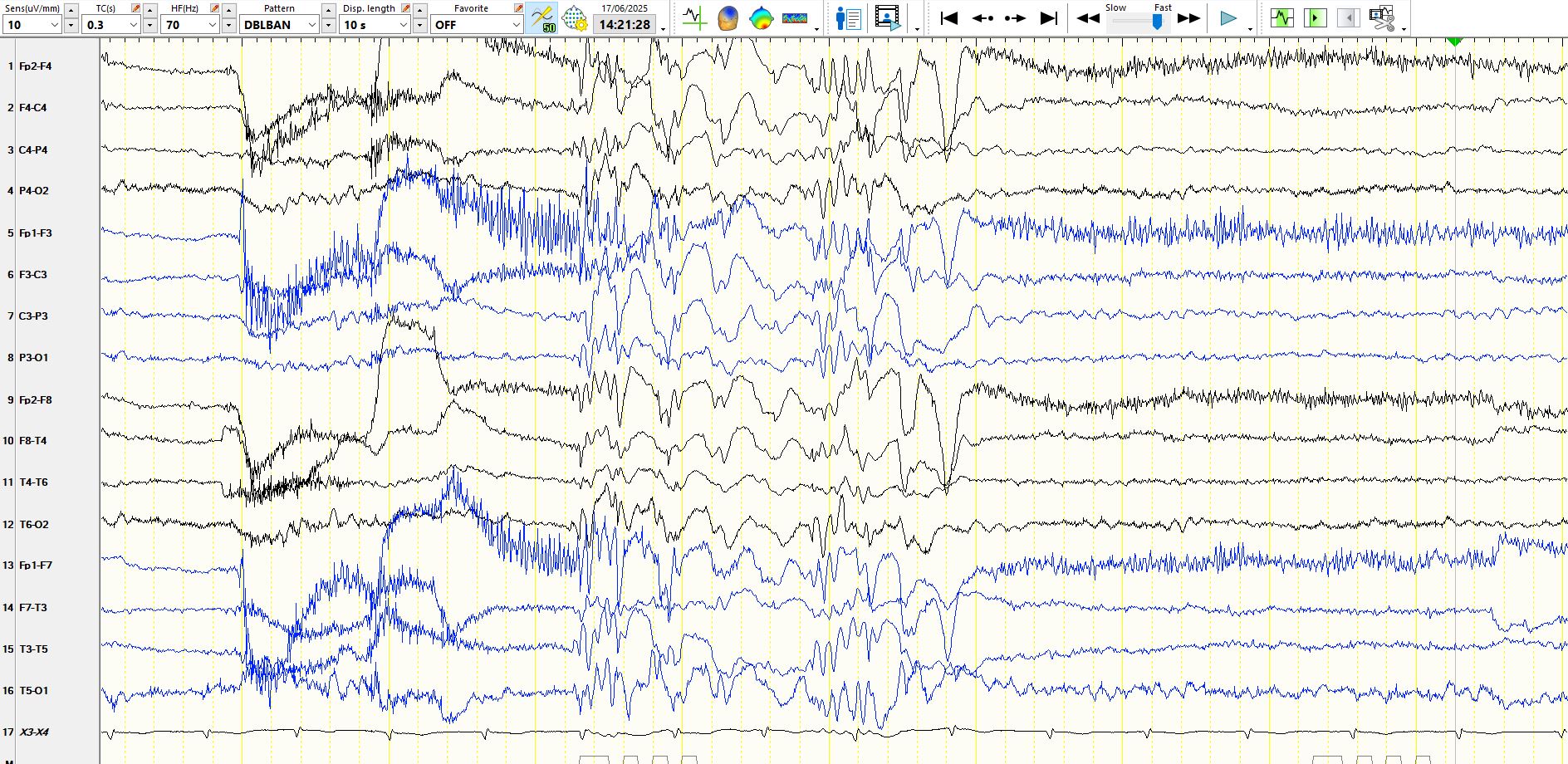
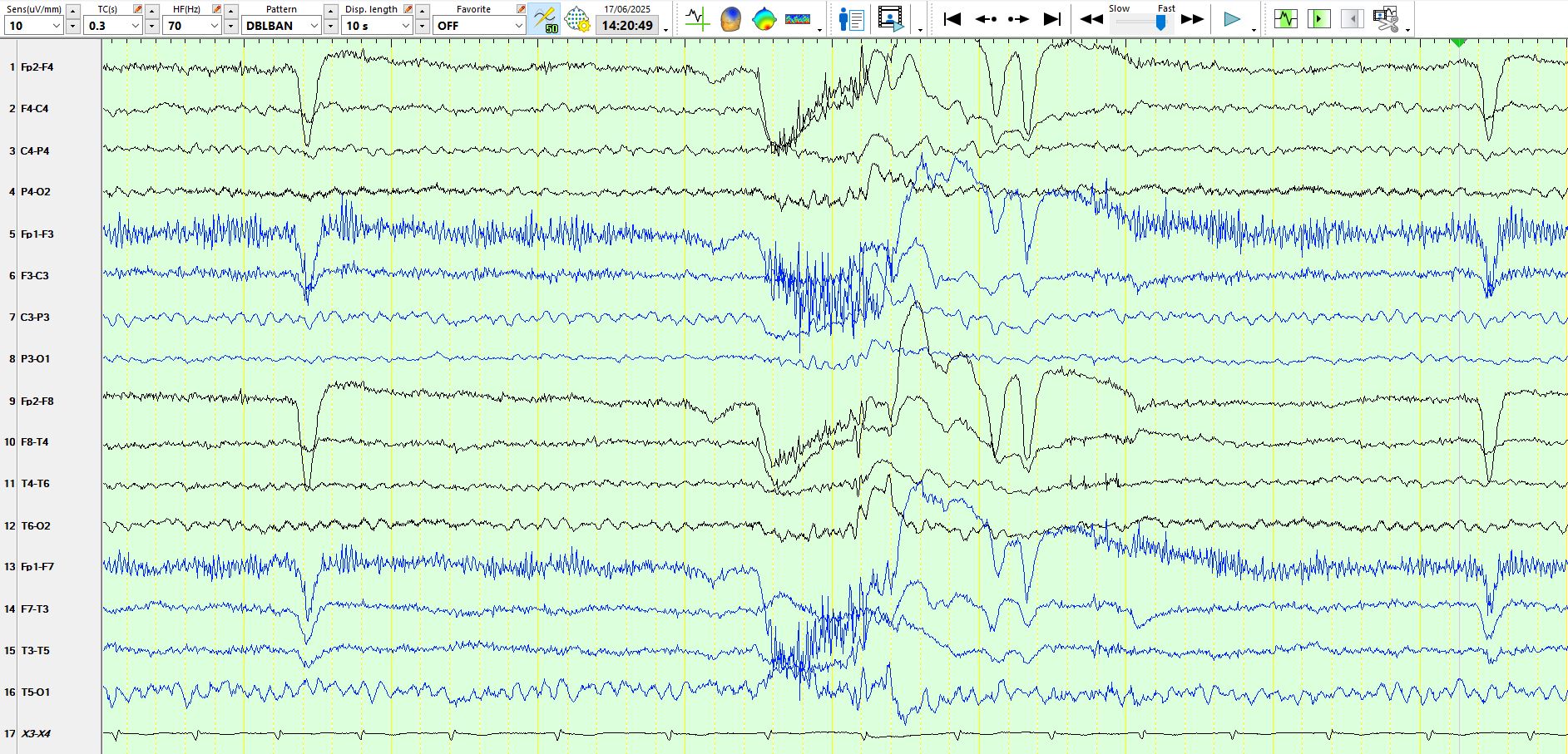
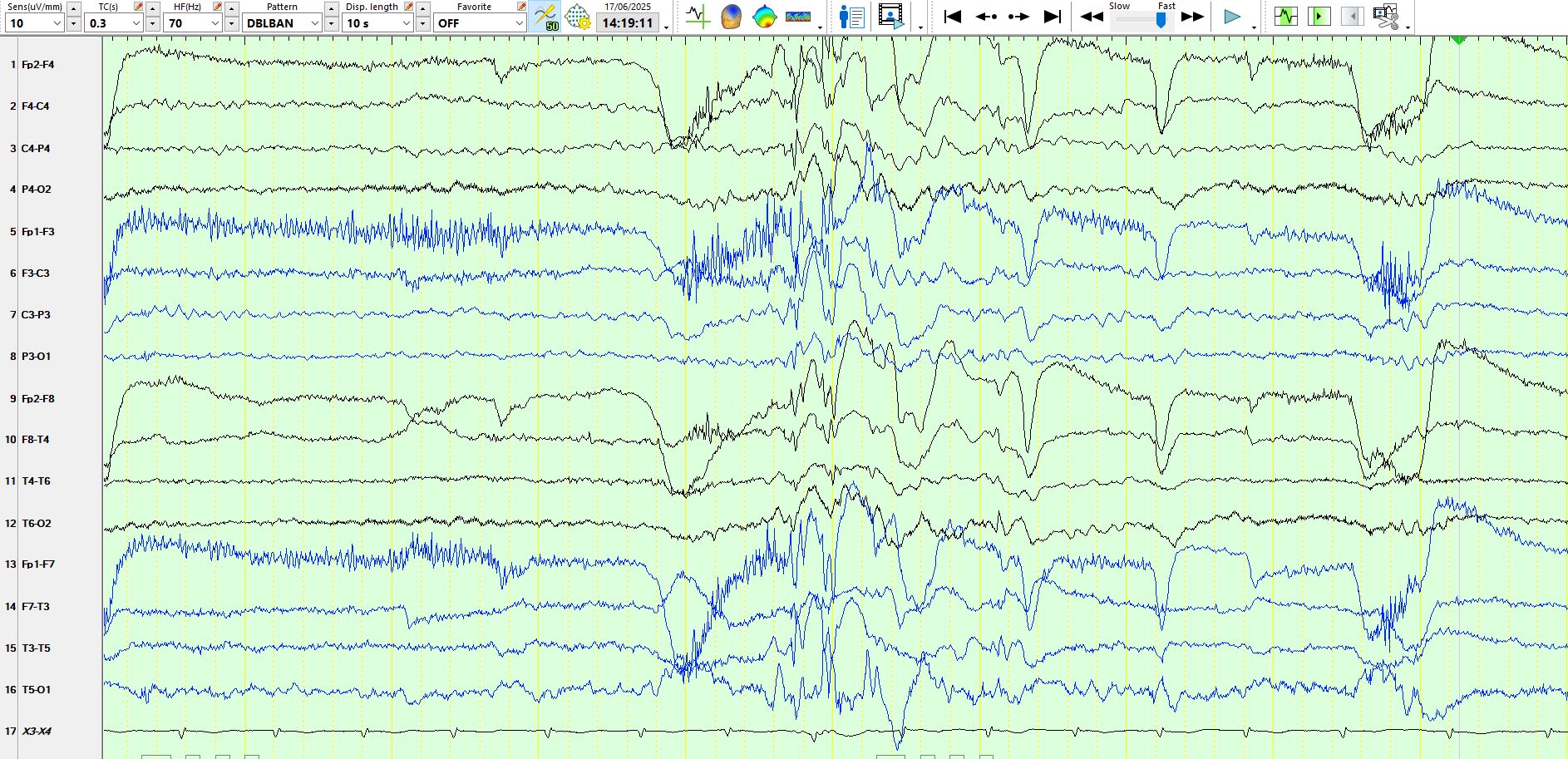
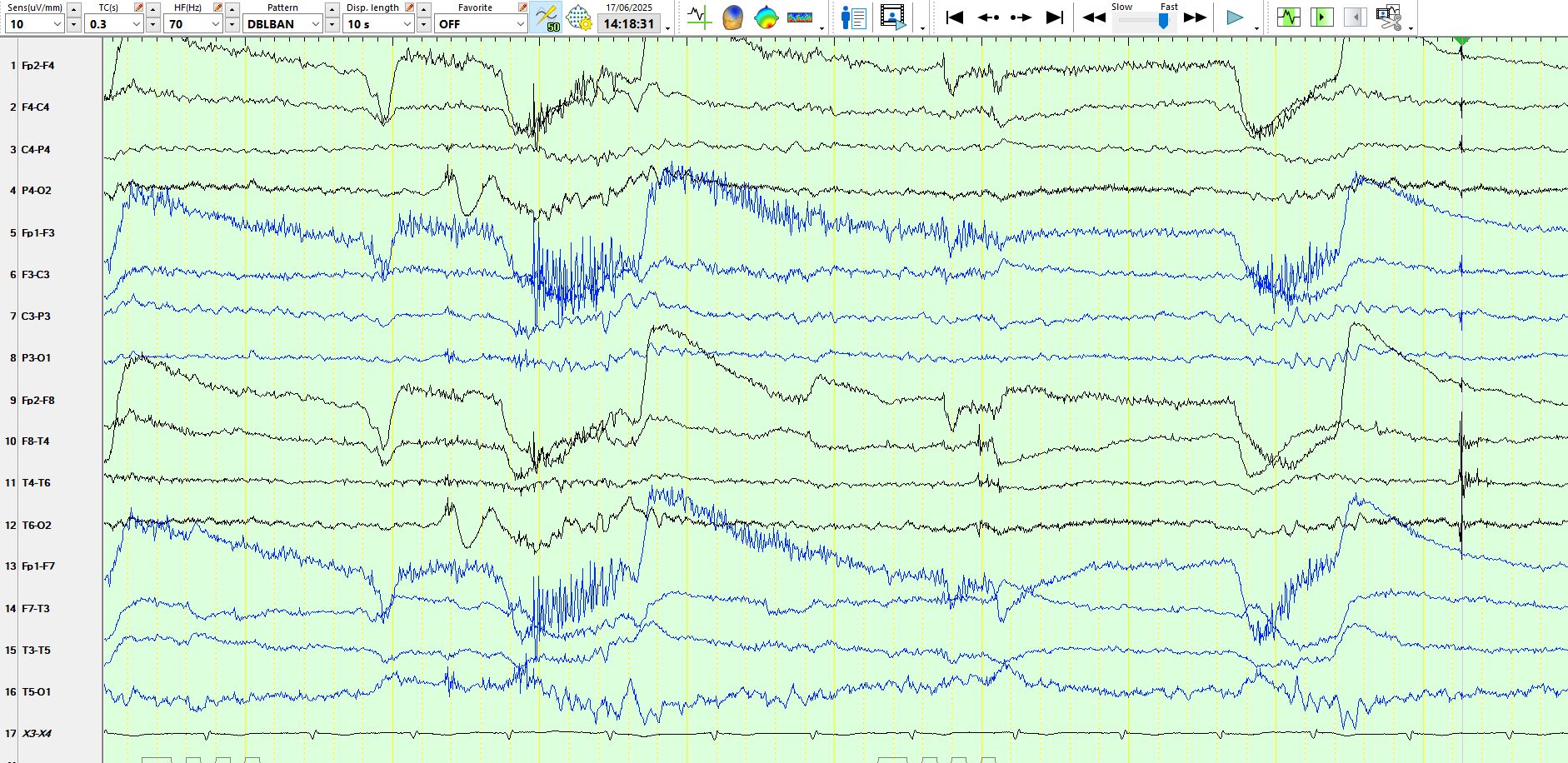
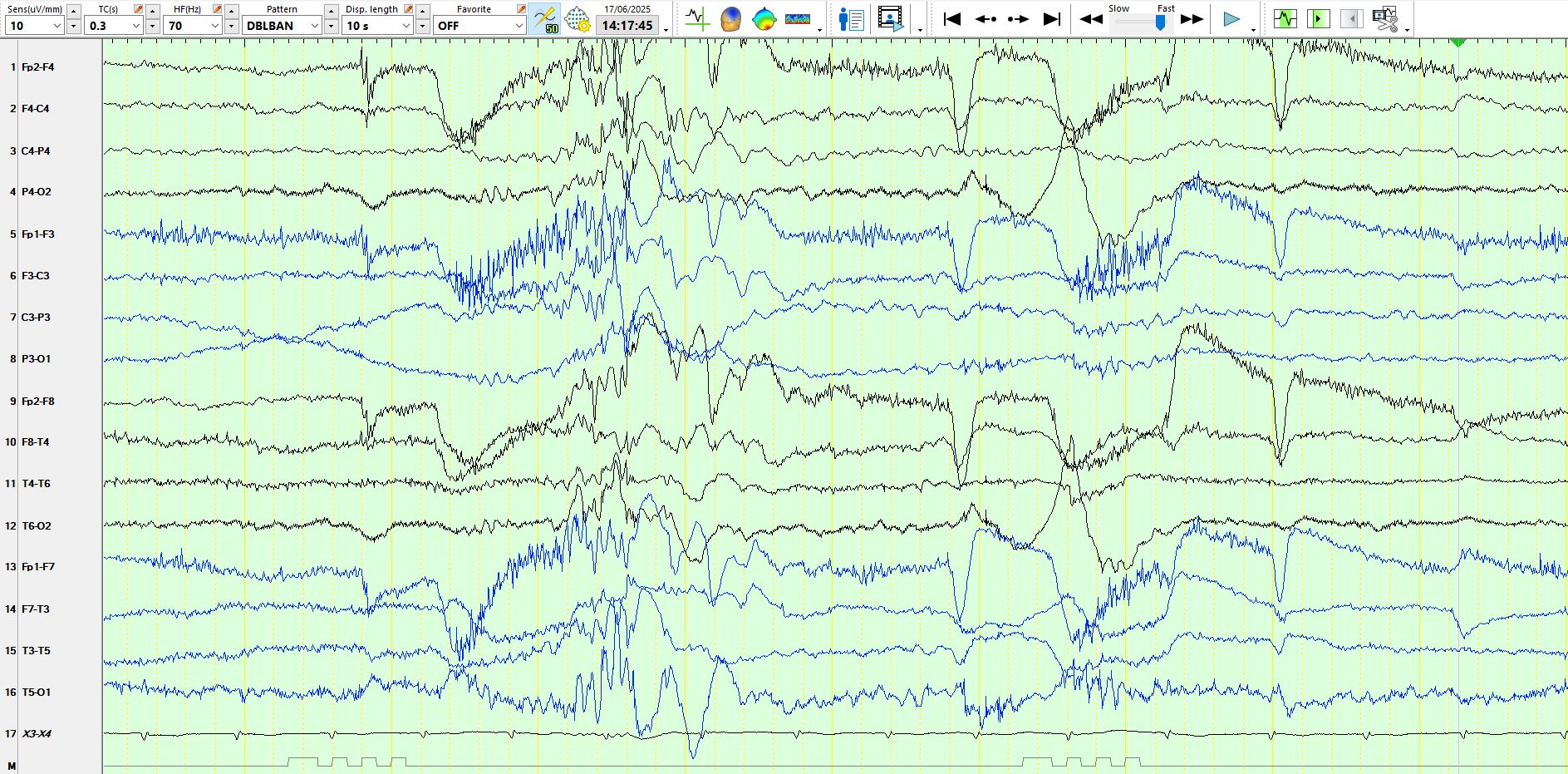
6 months ago, while using the same treatment, the patient developed absence seizures that have progressively increased in frequency, to the point that these occur innumerable times per day. During these the head goes backwards slightly, there are some "twitches" of the eyelids and the left arm jerks a few times in some. The following pages appear shortly after the start of the EEG. You can make the diagnosis on the first page, if you like:
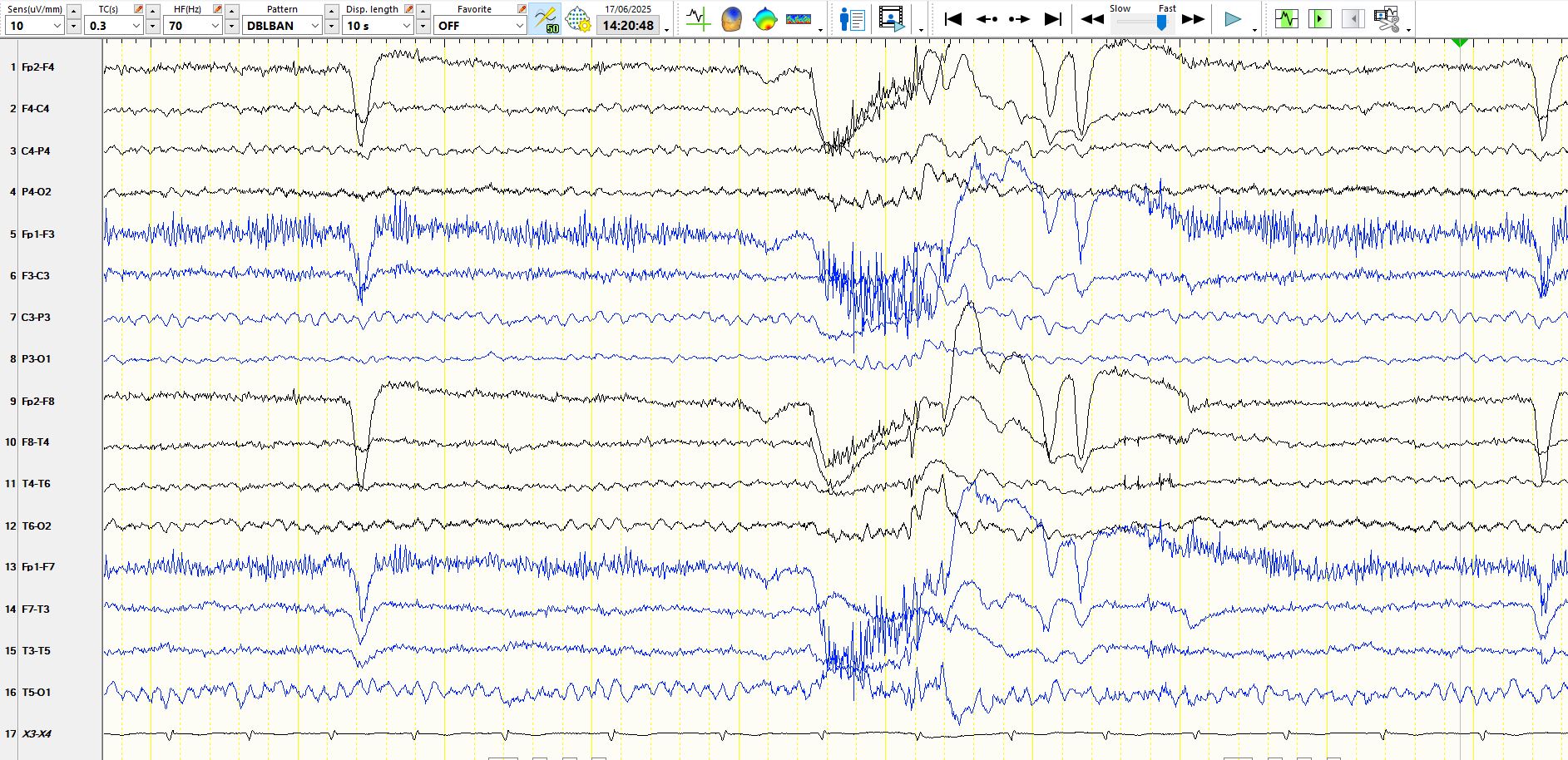
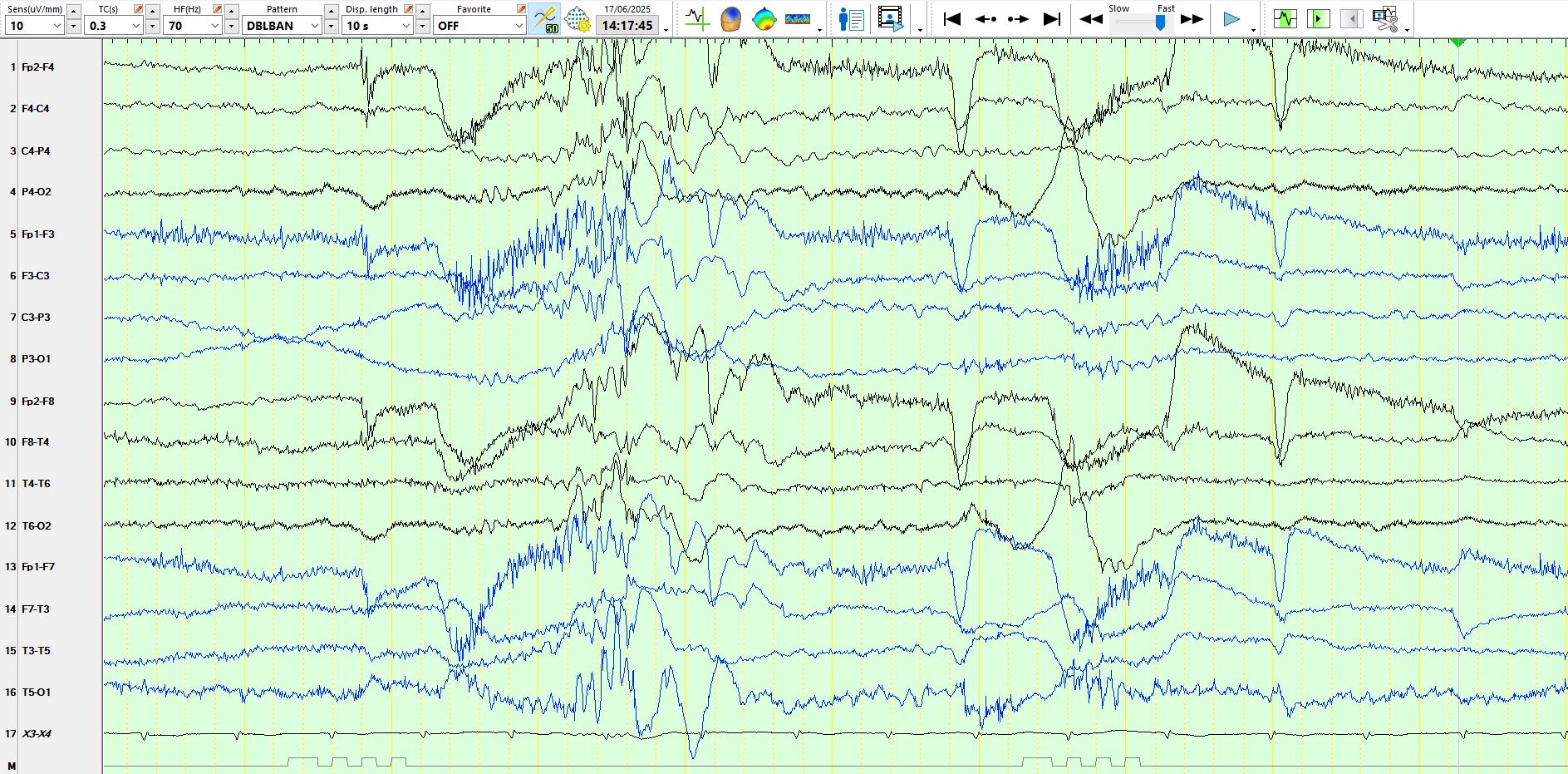
A few observations
1. Notice the EMG artifact on the "upslope" (especially) of the eye closure artefact
2. When this EMG artifact is superimposed on the 2nd phase of this eye closure, this waveform has a more gradual upslope than other blinks of the eyes
3. At the time that these occur, there is no clear cortical discharge to indicate a seizure(s), especially in the occipital regions
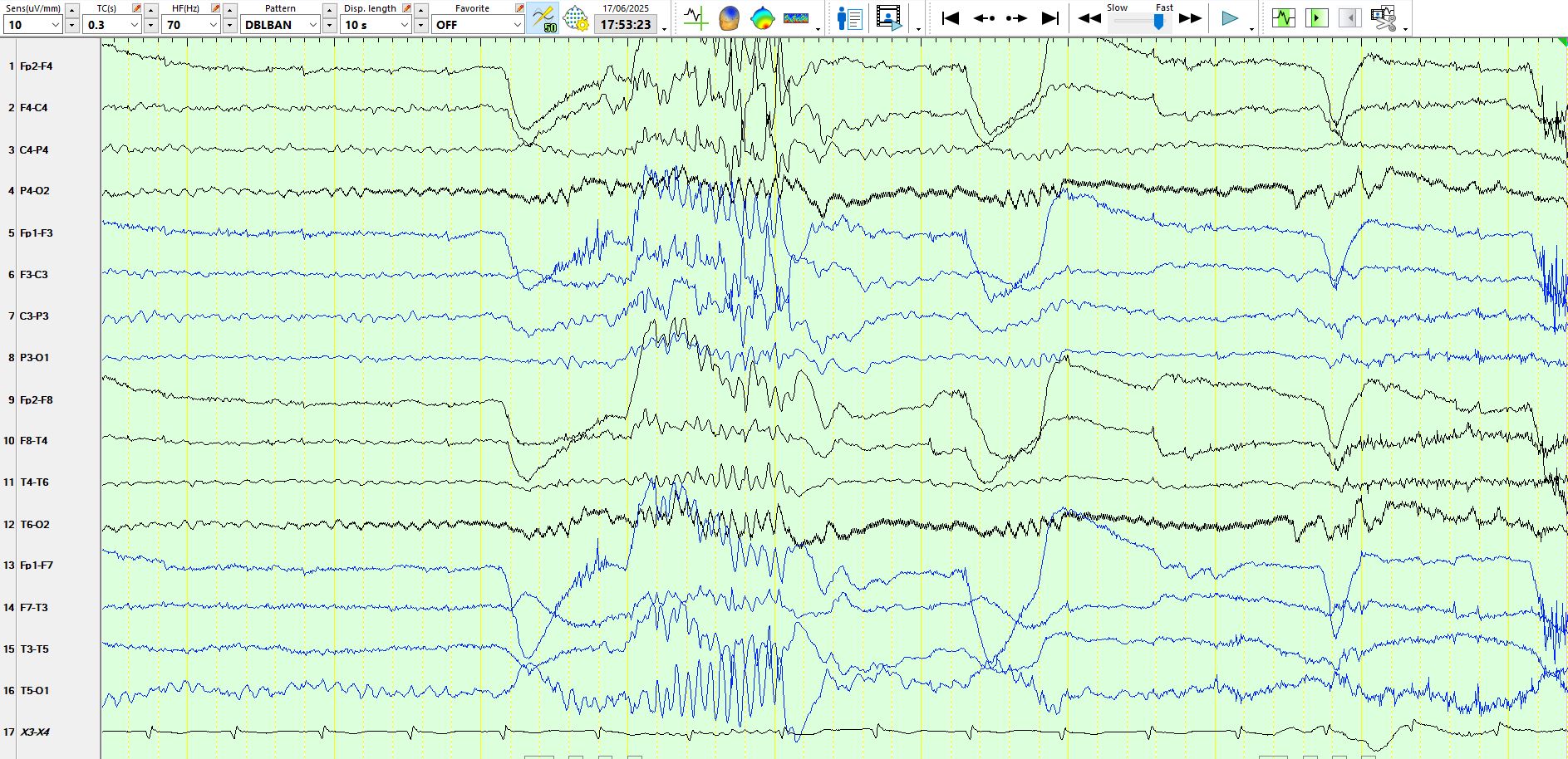
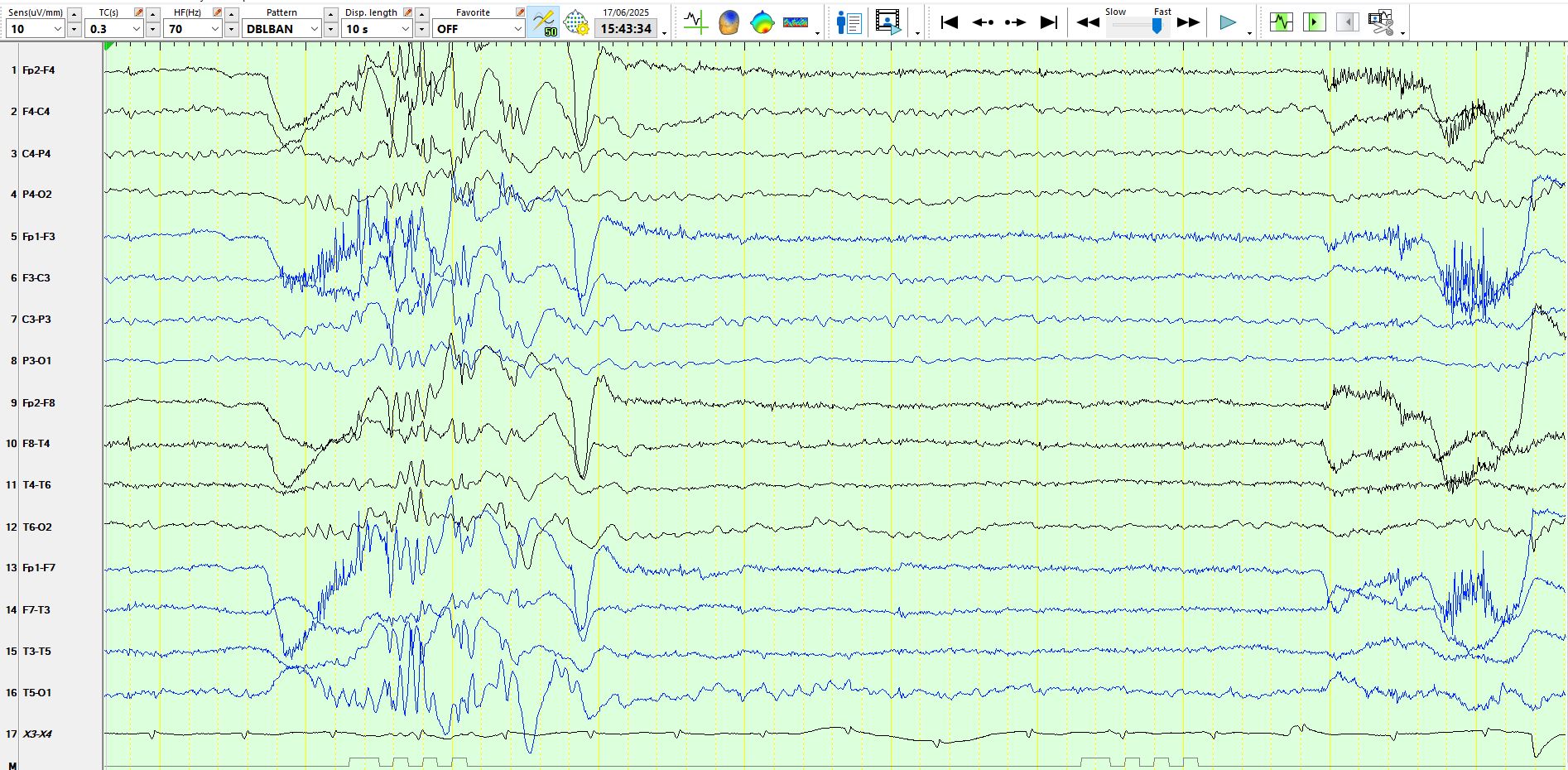
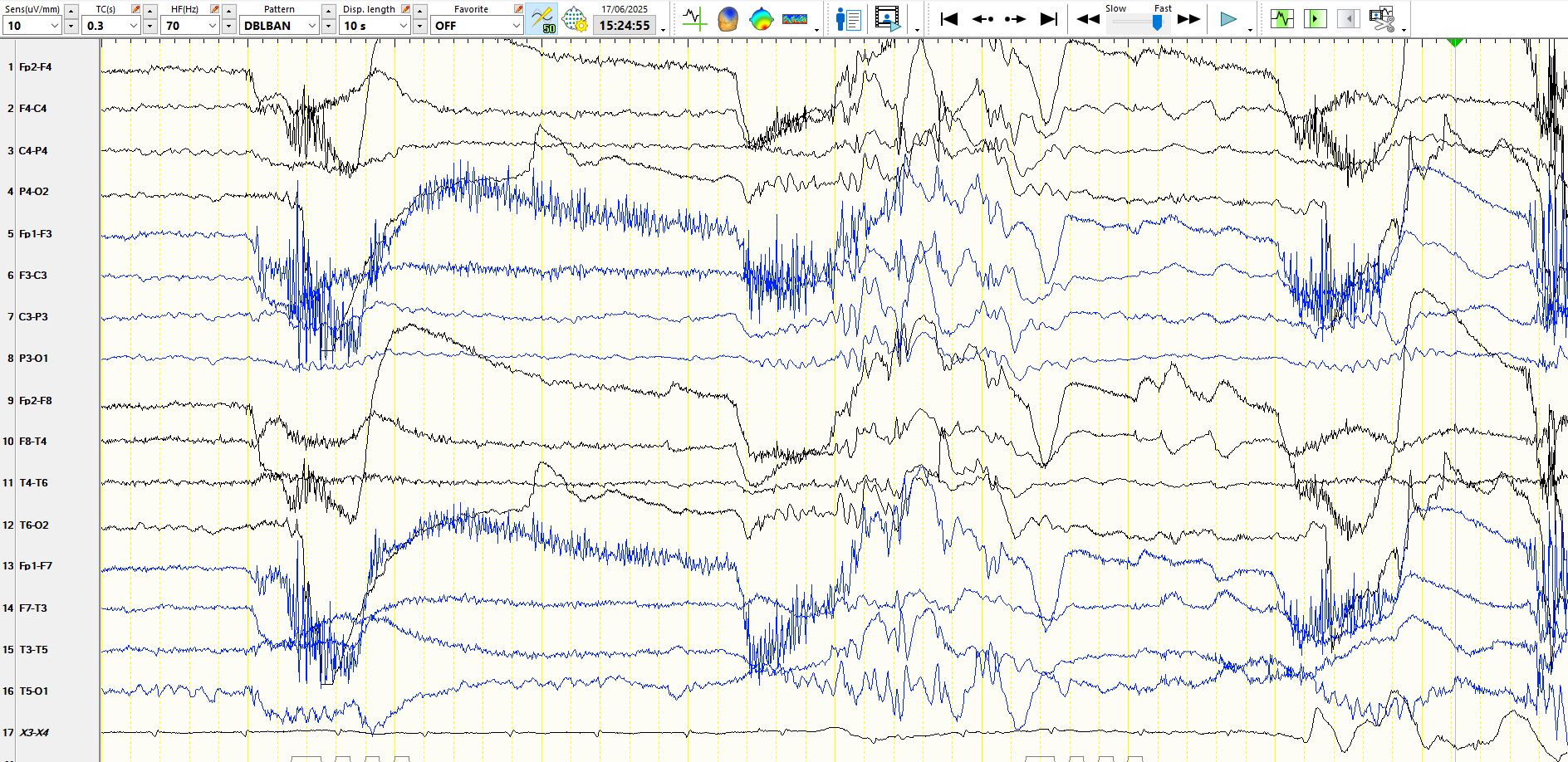
4. Some of these eye movements are followed by generalised, polyspike and wave
5. Some of these eye movements have no following generalised polyspikes and wave and therefore no associated spikes or polyspikes
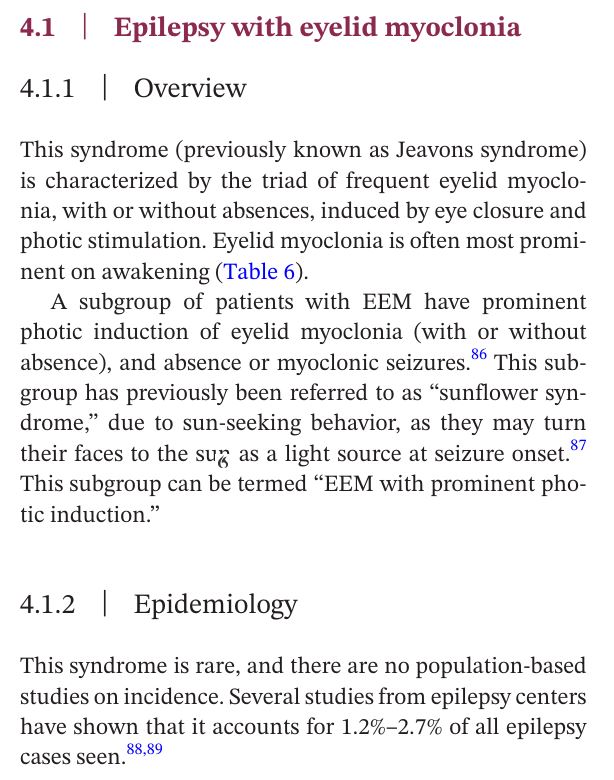
6. The EEG is diagnostic of epilepsy with eyelid myoclonia. It is easily missed.
The EMG artifact on the upslope of the eye movement artefact represents eyelid myoclonus. The current view is that visual input (or at least the cessation by eye closure) produces a discharge in the occipital regions, which project to the frontal regions and produce the eyelid myoclonus.
Epilepsy With Eyelid Myoclonia (Jeavons Syndrome) - PubMed
The "International league against epilepsy classification and definition of epilepsy syndromes with onset in childhood: position paper by the ILAE task Force on nosology and definitions" has the following to say:
International League Against Epilepsy classification and definition of epilepsy syndromes with onset in childhood: Position paper by the ILAE Task Force on Nosology and Definitions - PubMed
I cannot agree with the above statement, highlighted in yellow. The statement above is factually incorrect, since myoclonus of cortical origin may exhibit no change on the EEG. Hence, the conclusion that this represents a movement disorder is based on flawed facts. And since these myoclonic movements of the eyes are strongly associated with absence seizures and generalised polyspike-and-wave (have a look at the EEGs above), the logic of the conclusion has to be strongly questioned. I will look up the reference number 95 at a later stage.