
13y, Friday Frown
Jul 11, 2025Have a look at the following pages: the patient is initially awake and later asleep. Do you see any abnormalities during wakefulness or sleep?
Figure 1. Awake:
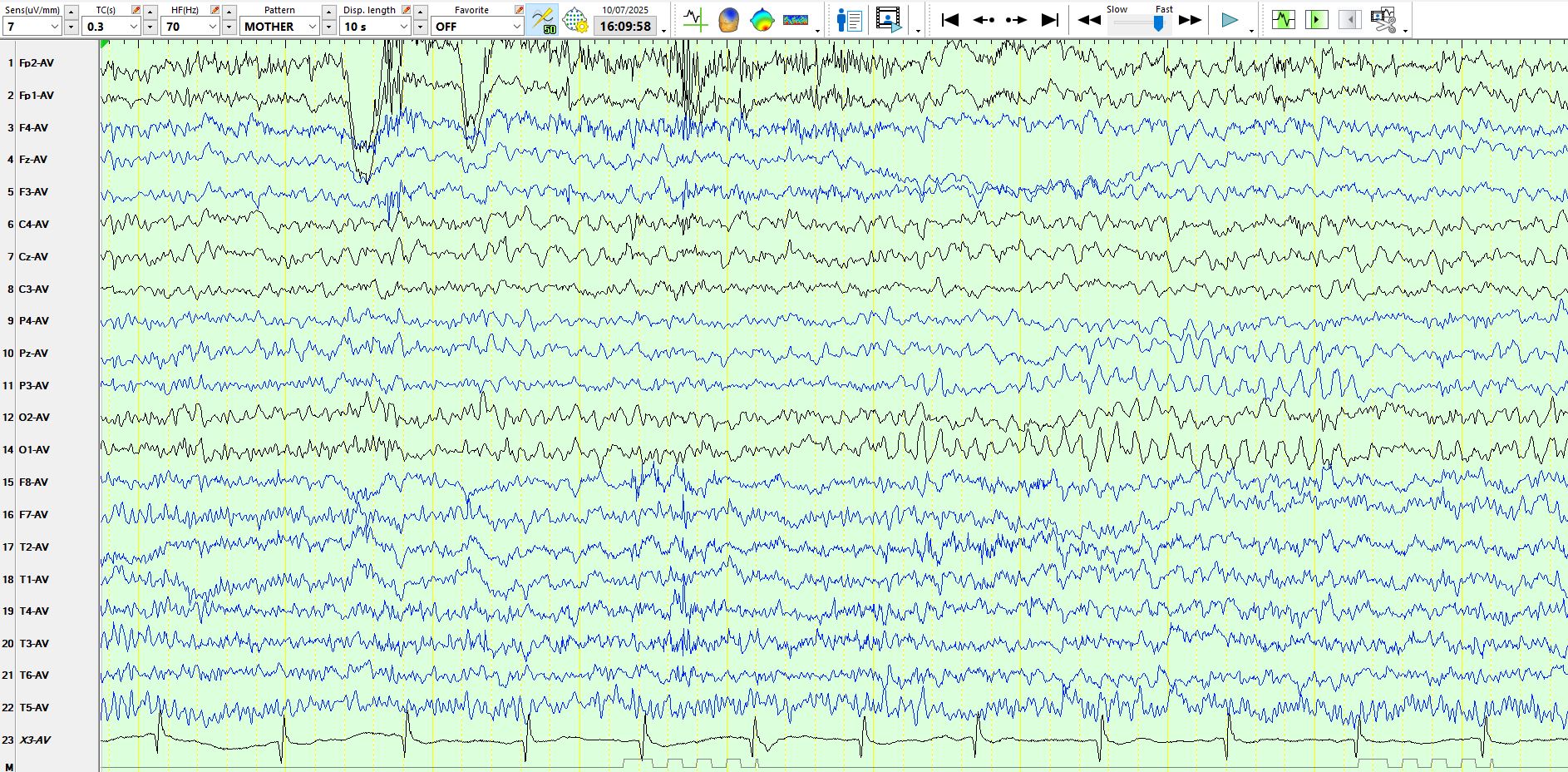
Figure 2. Awake, the eyes are open:
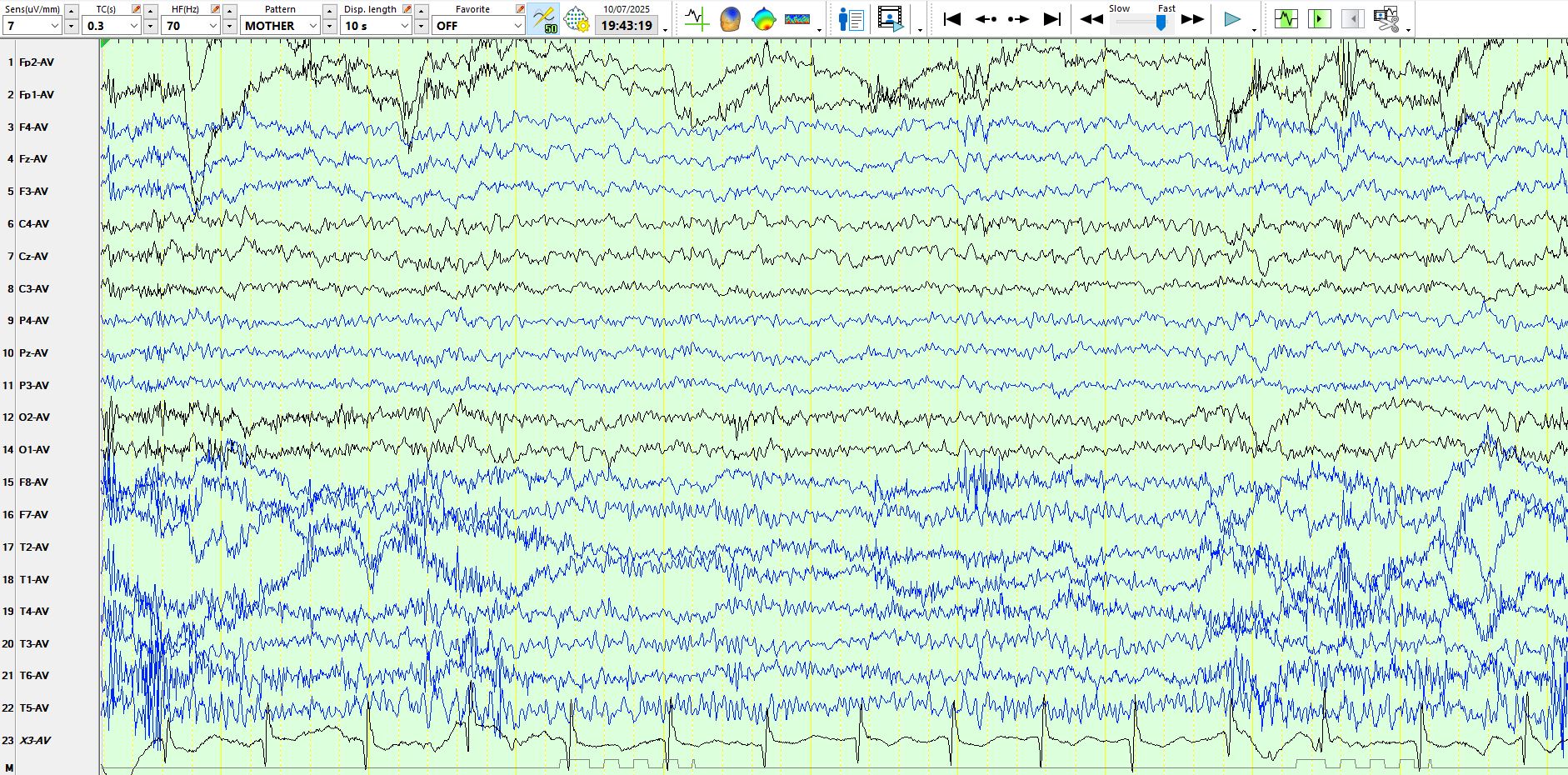
Figure 3. Awake:
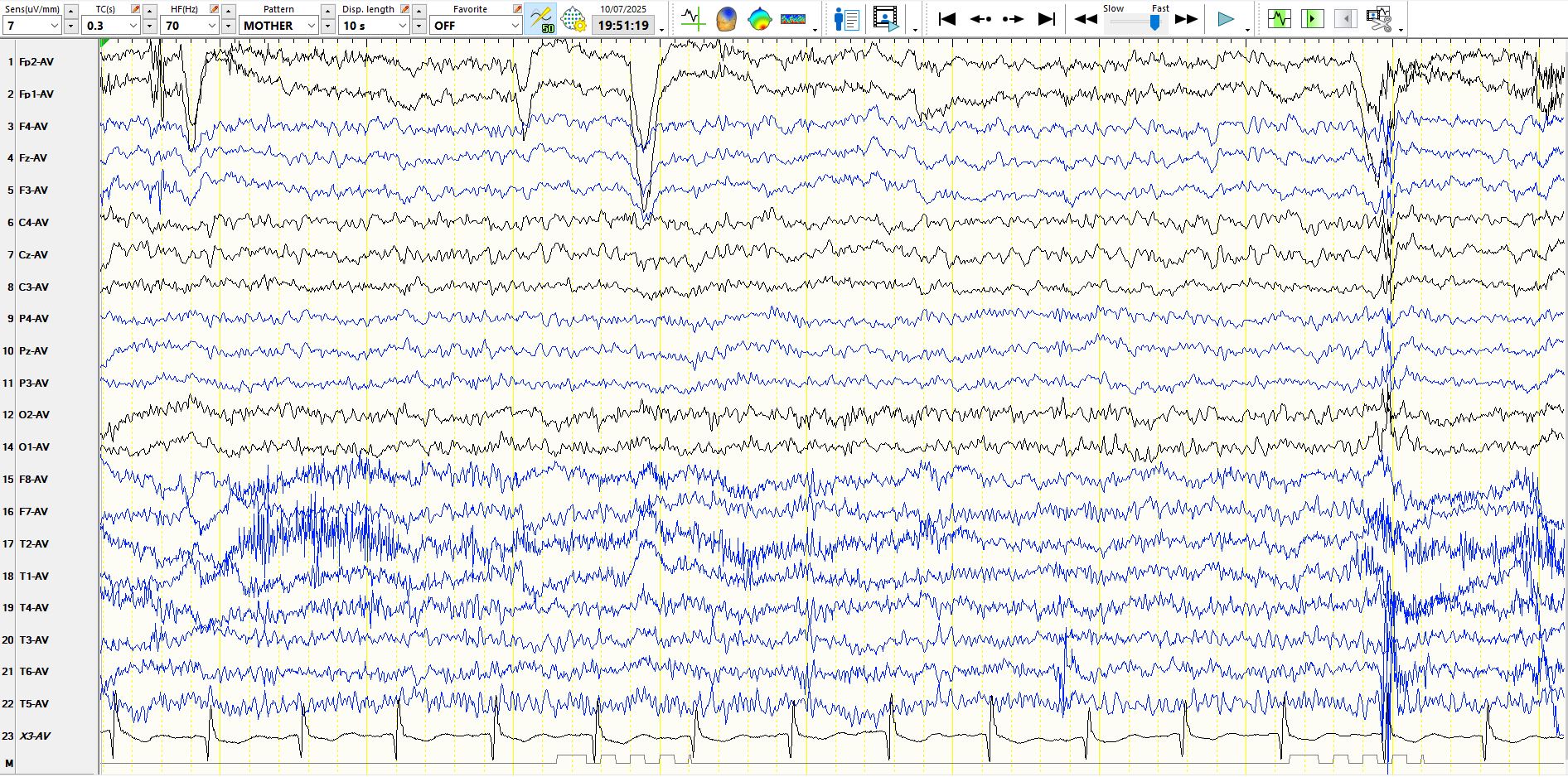
Figure 4:.Awake/mildly drowsy:
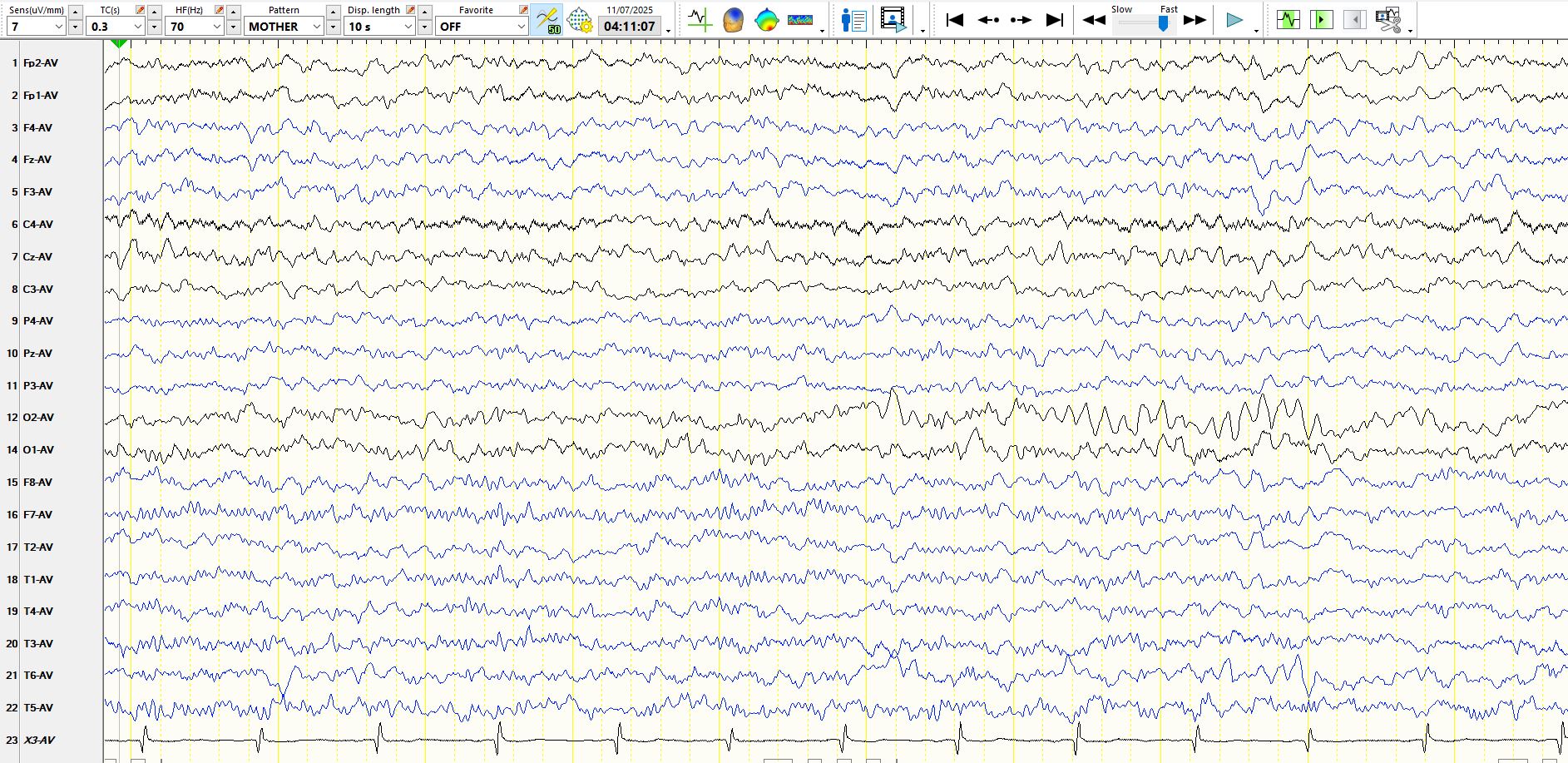
Figure 5:
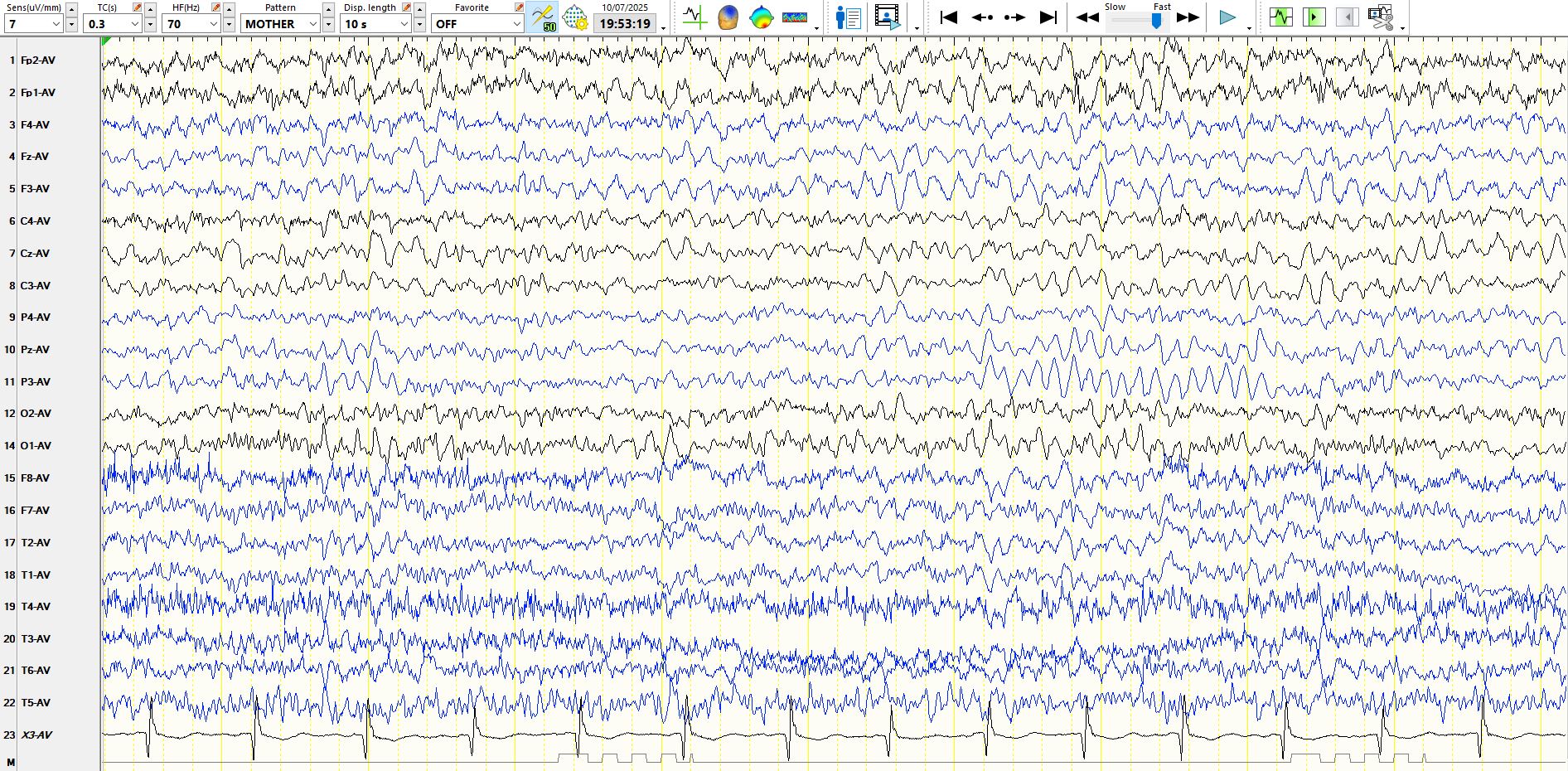
Figure 6. Sleep:
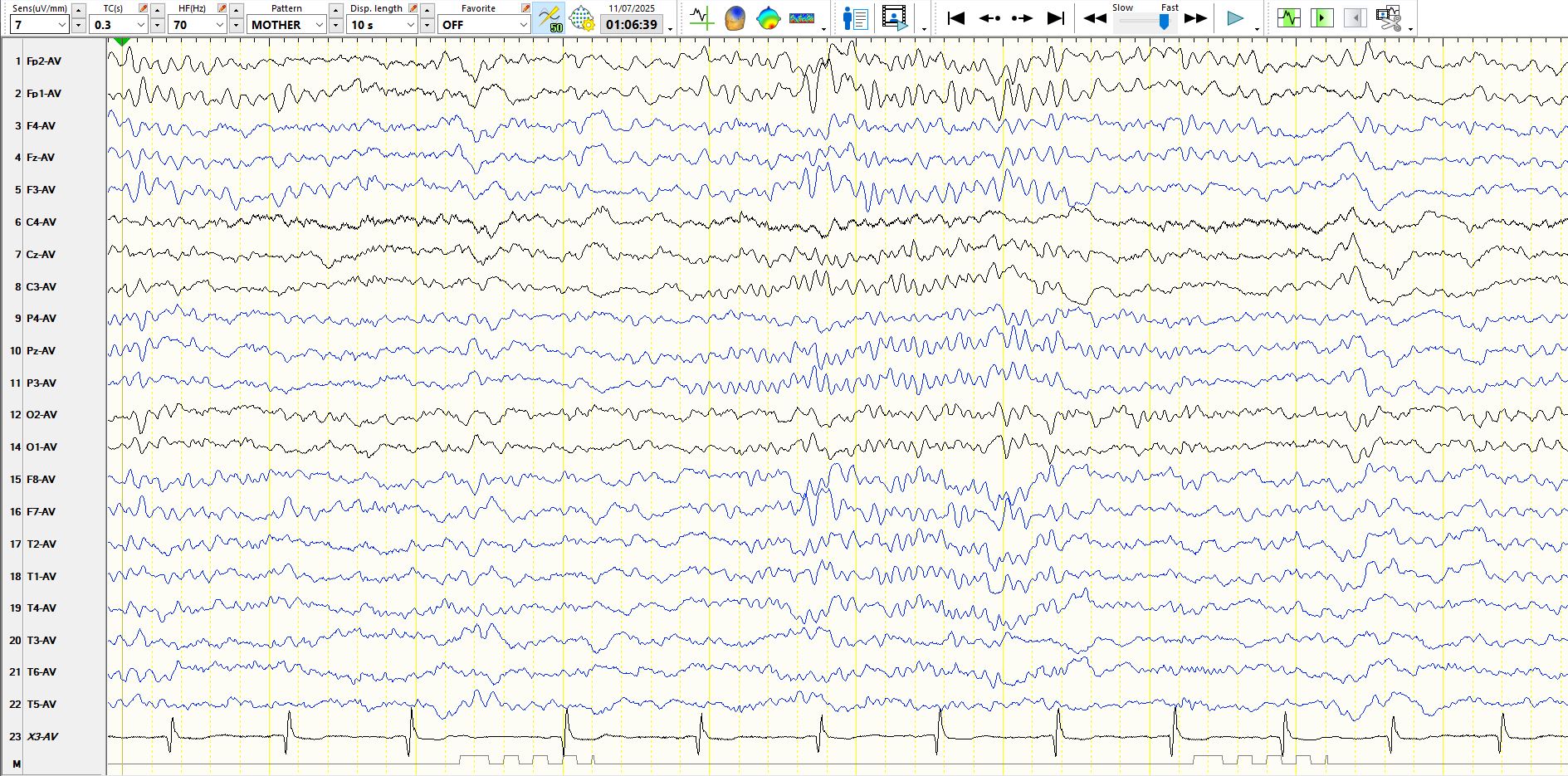
Figure 7:
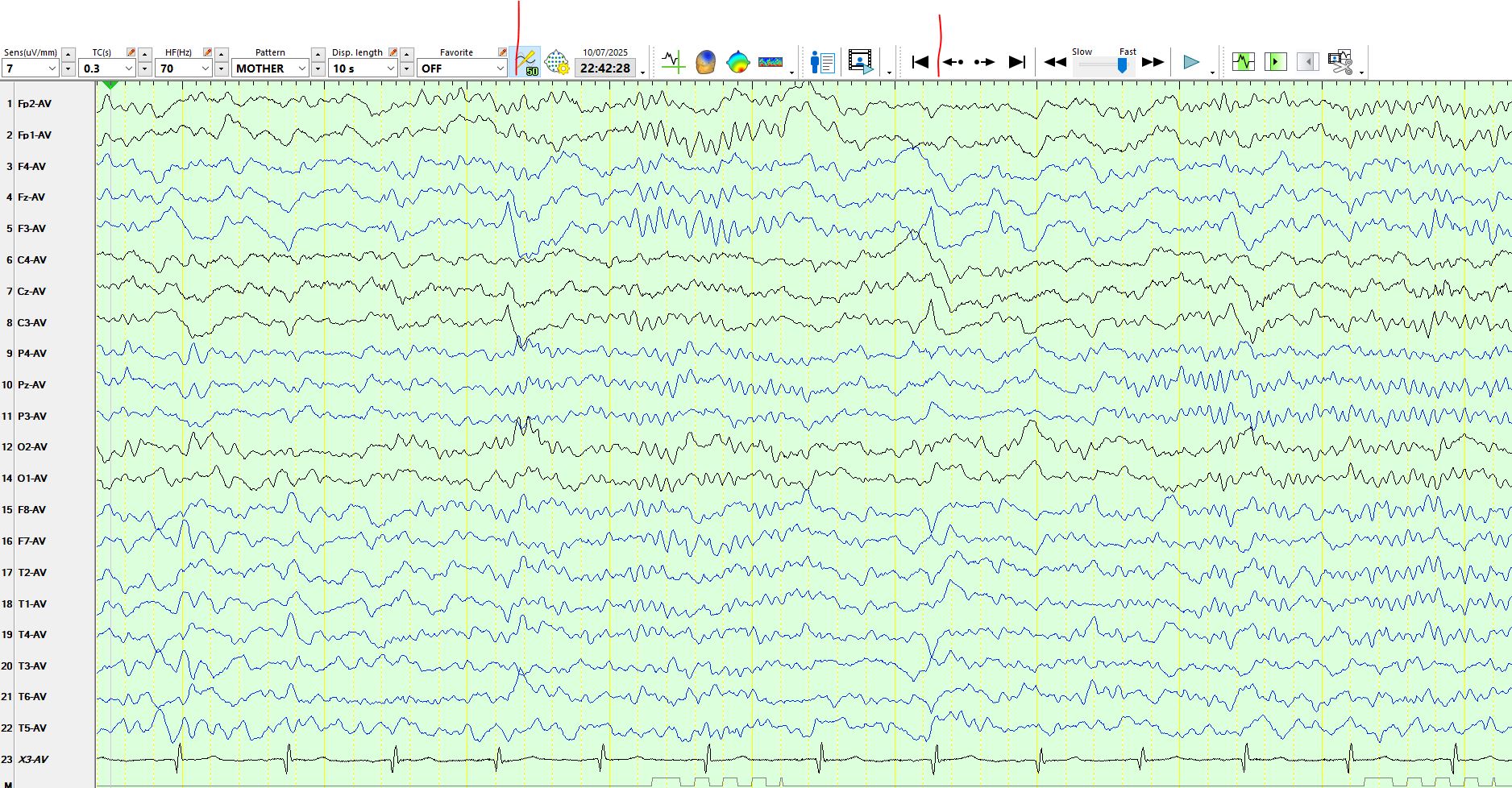
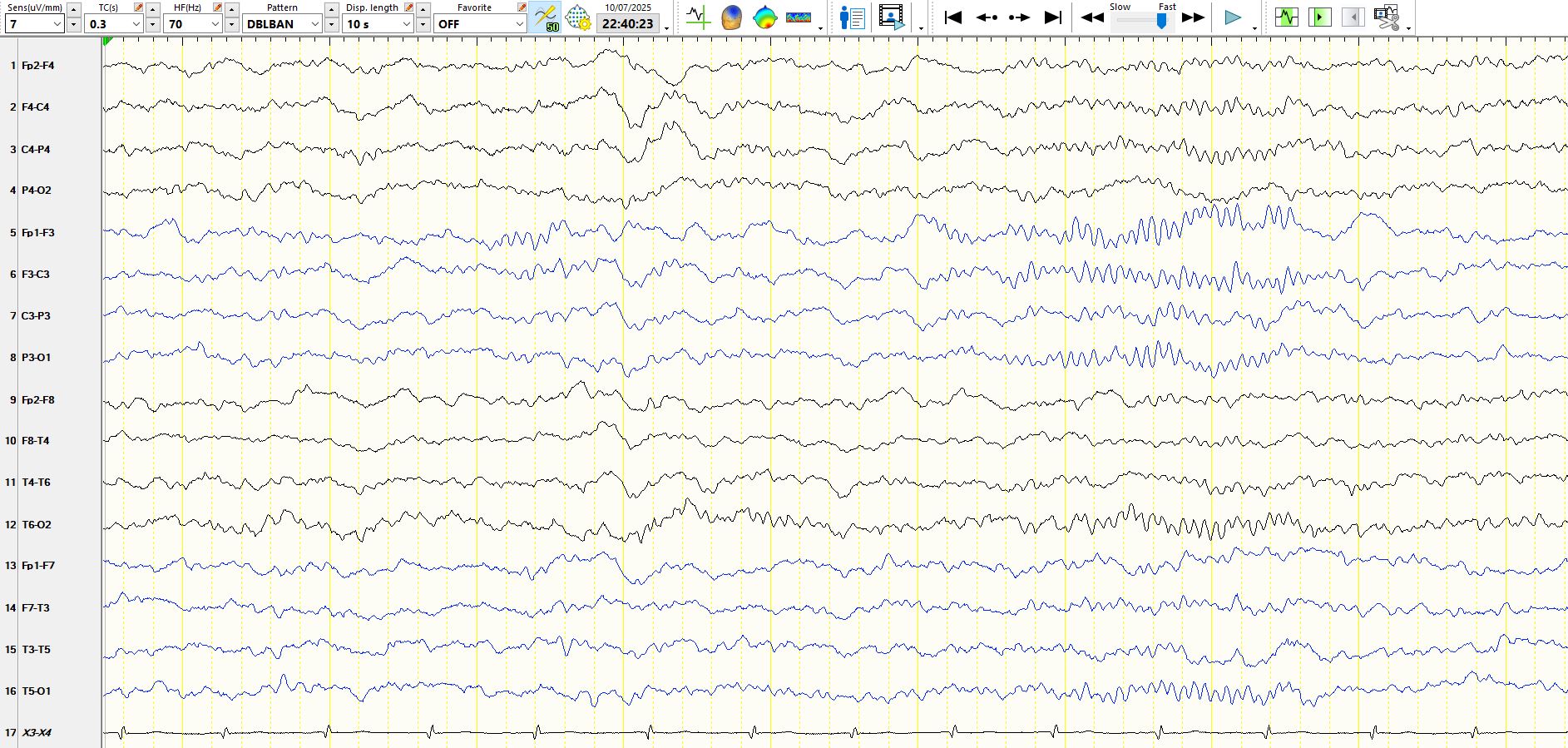
Figure 8:
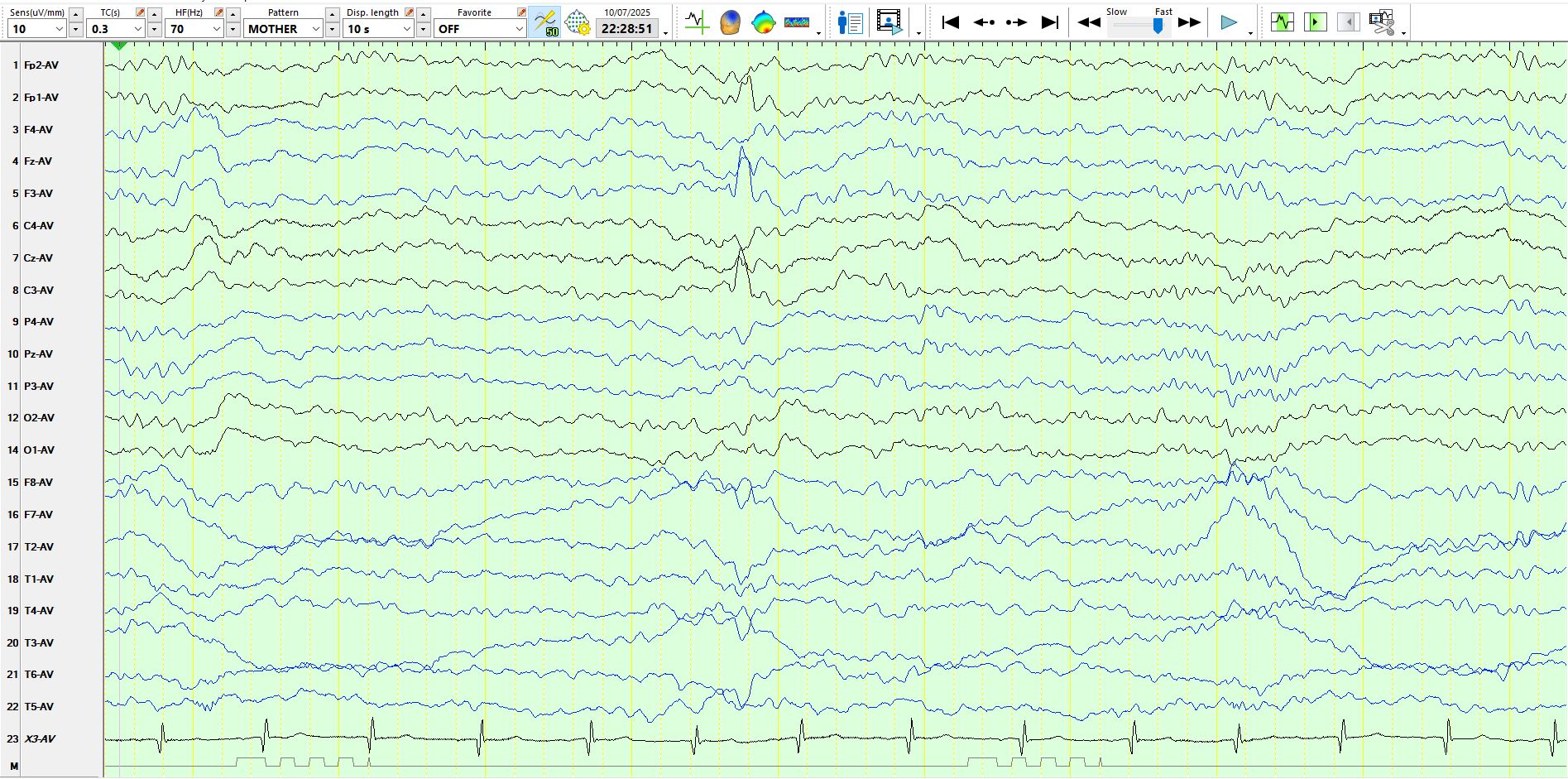
figure 9:
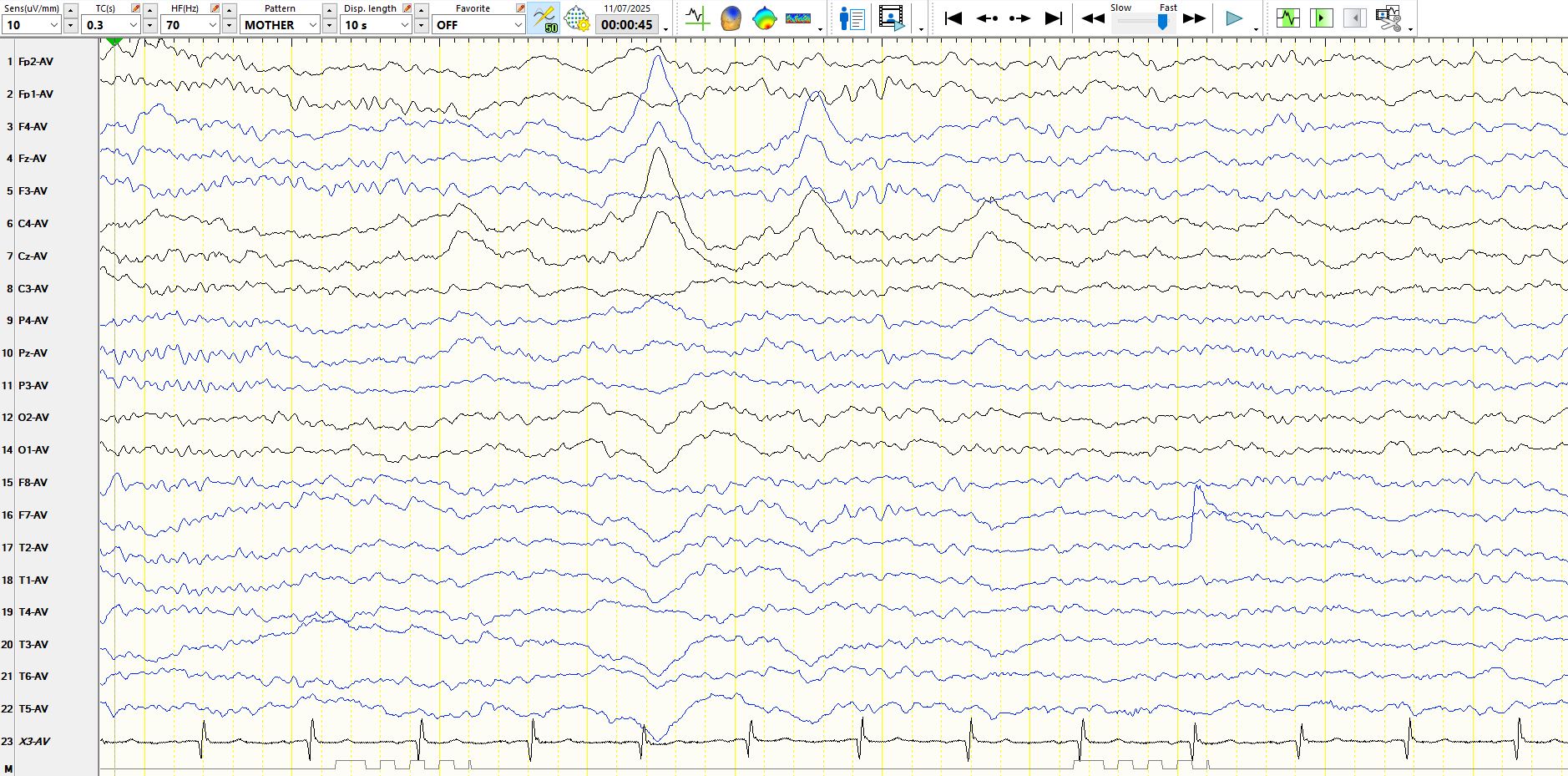
Figure 10:

Figure 11:
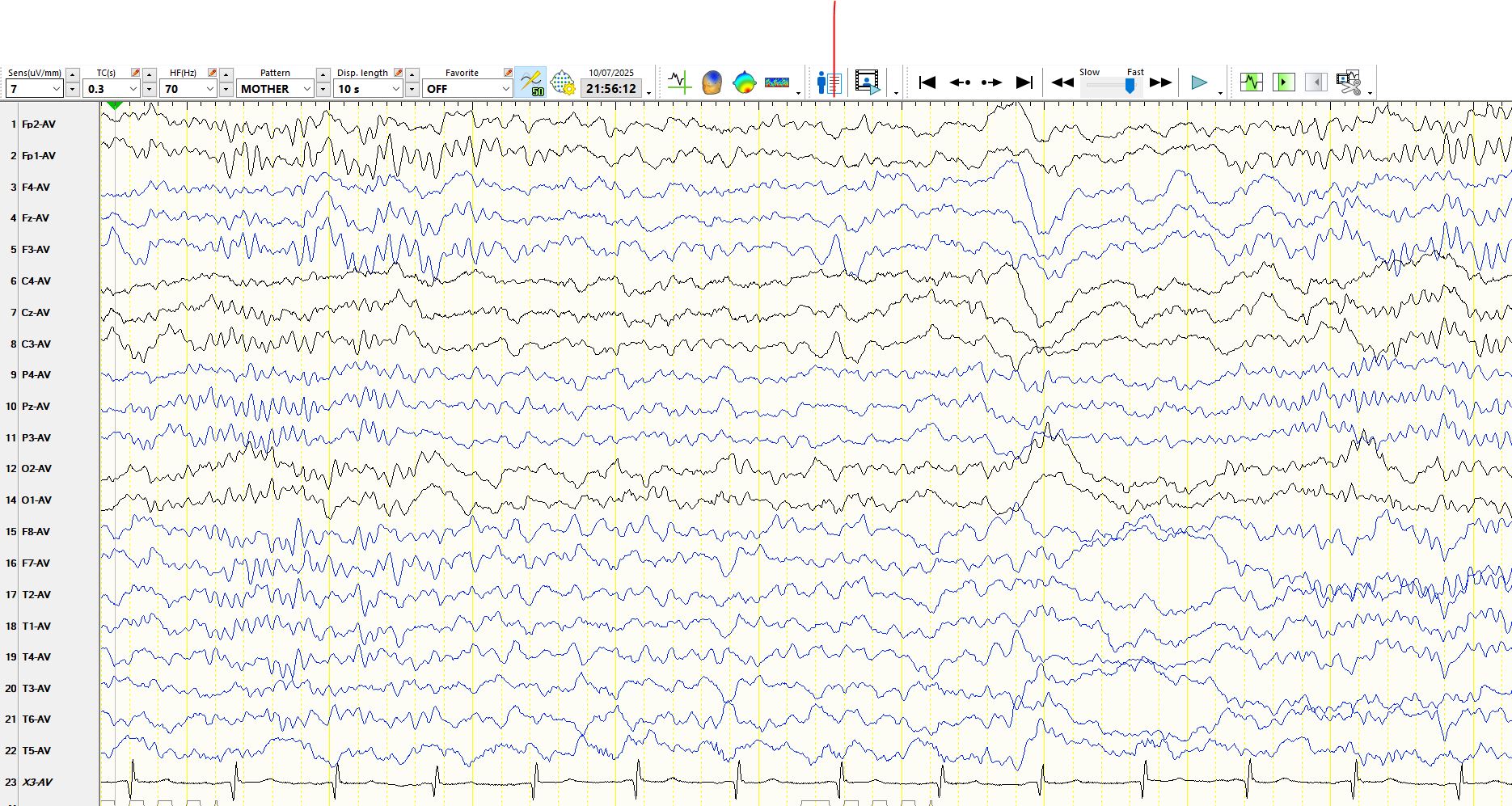
Figure 12:
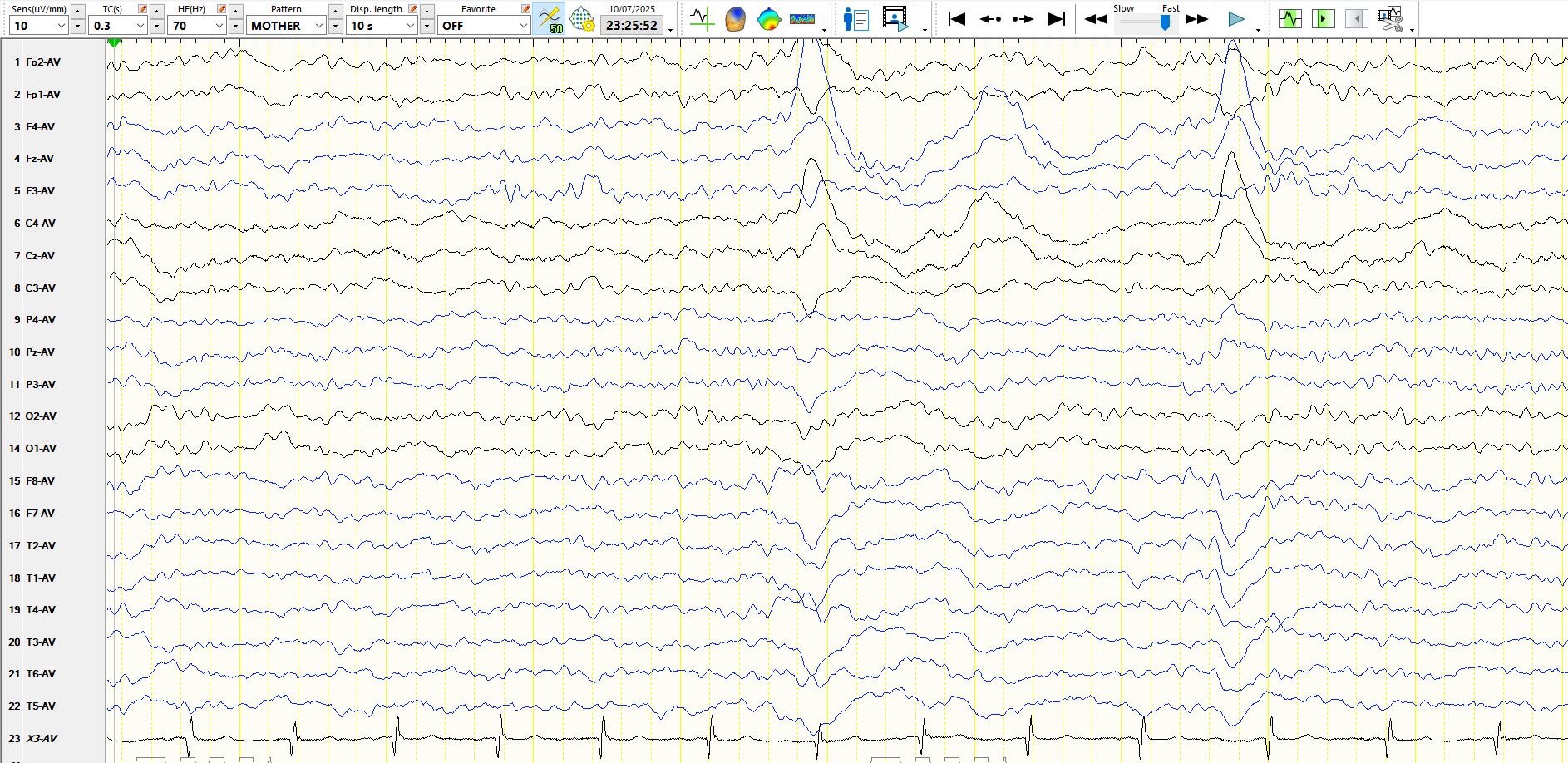
Figure 13:

Figure 14:
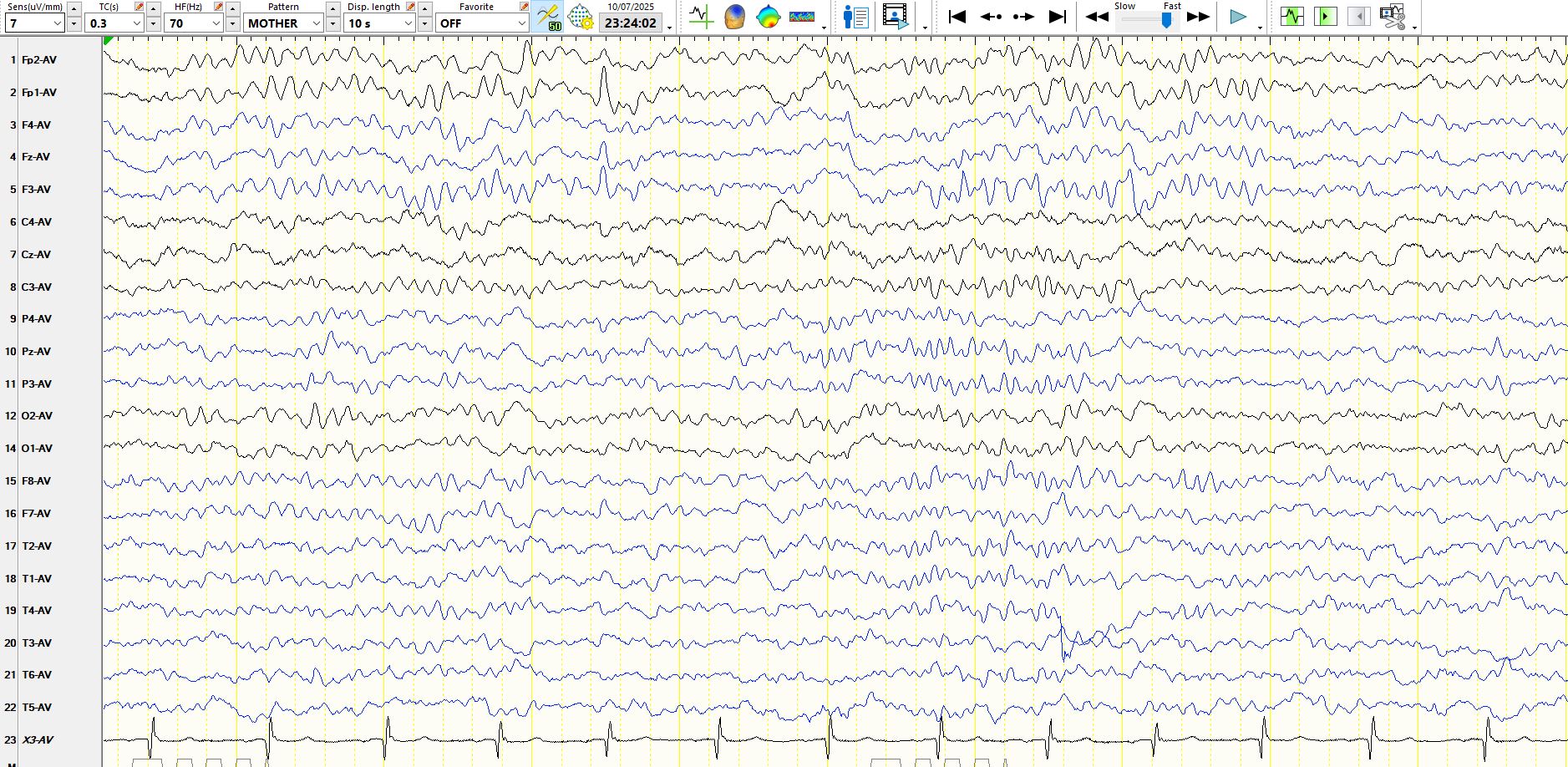
Figure 15:
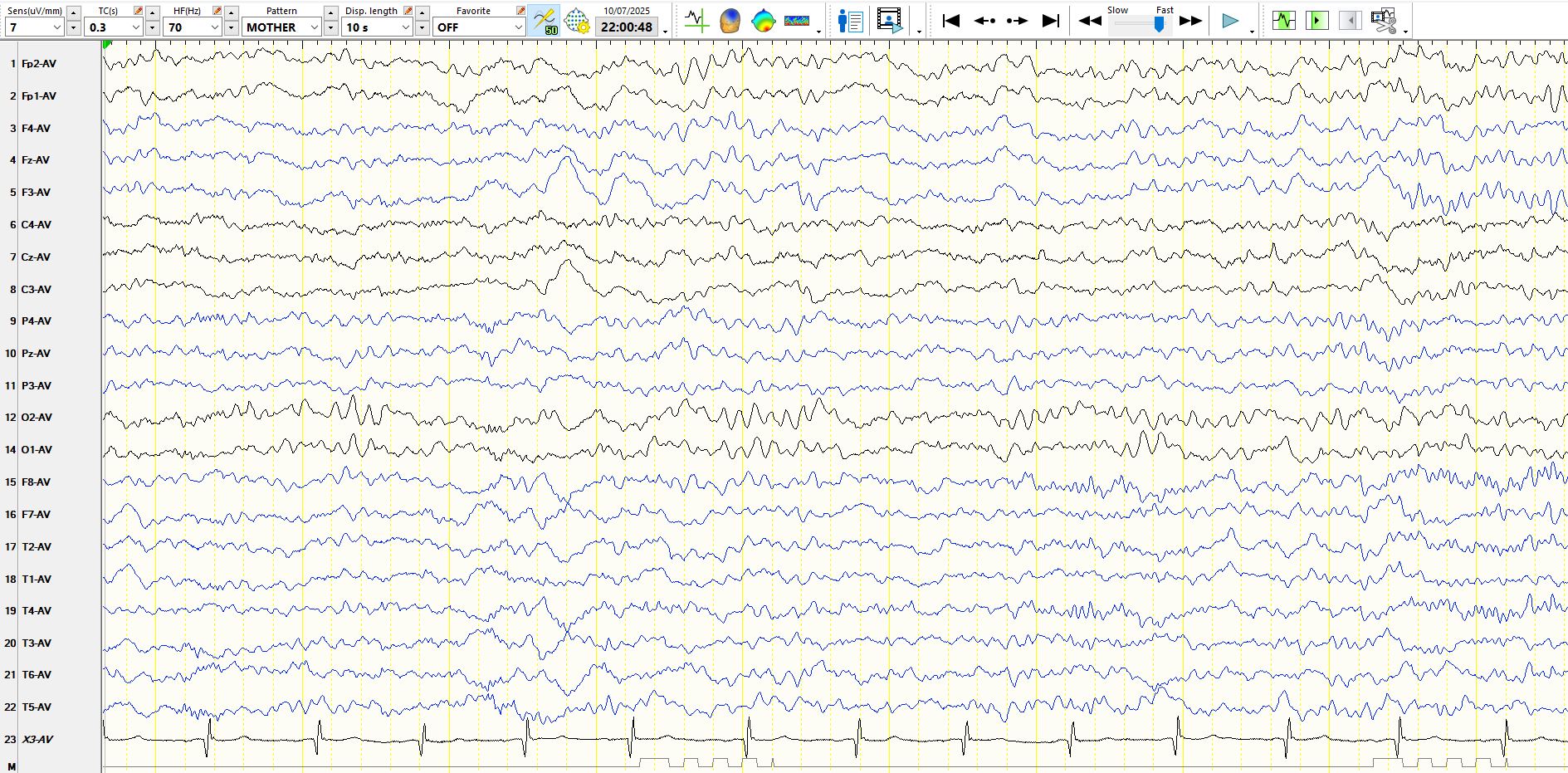
Figure 16:
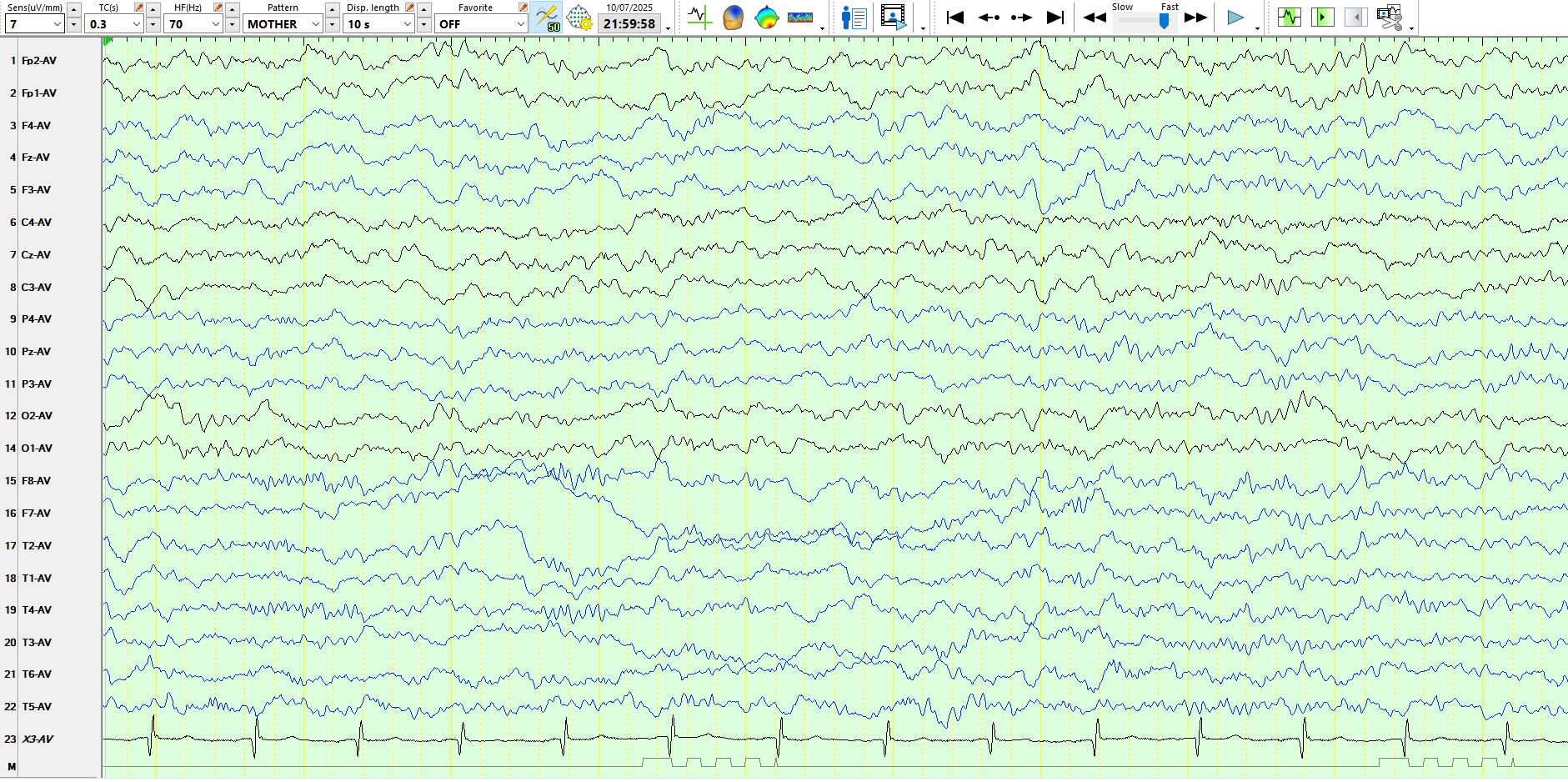
Figure 17:

Figure 18:
Figure 19:
Figure 20:
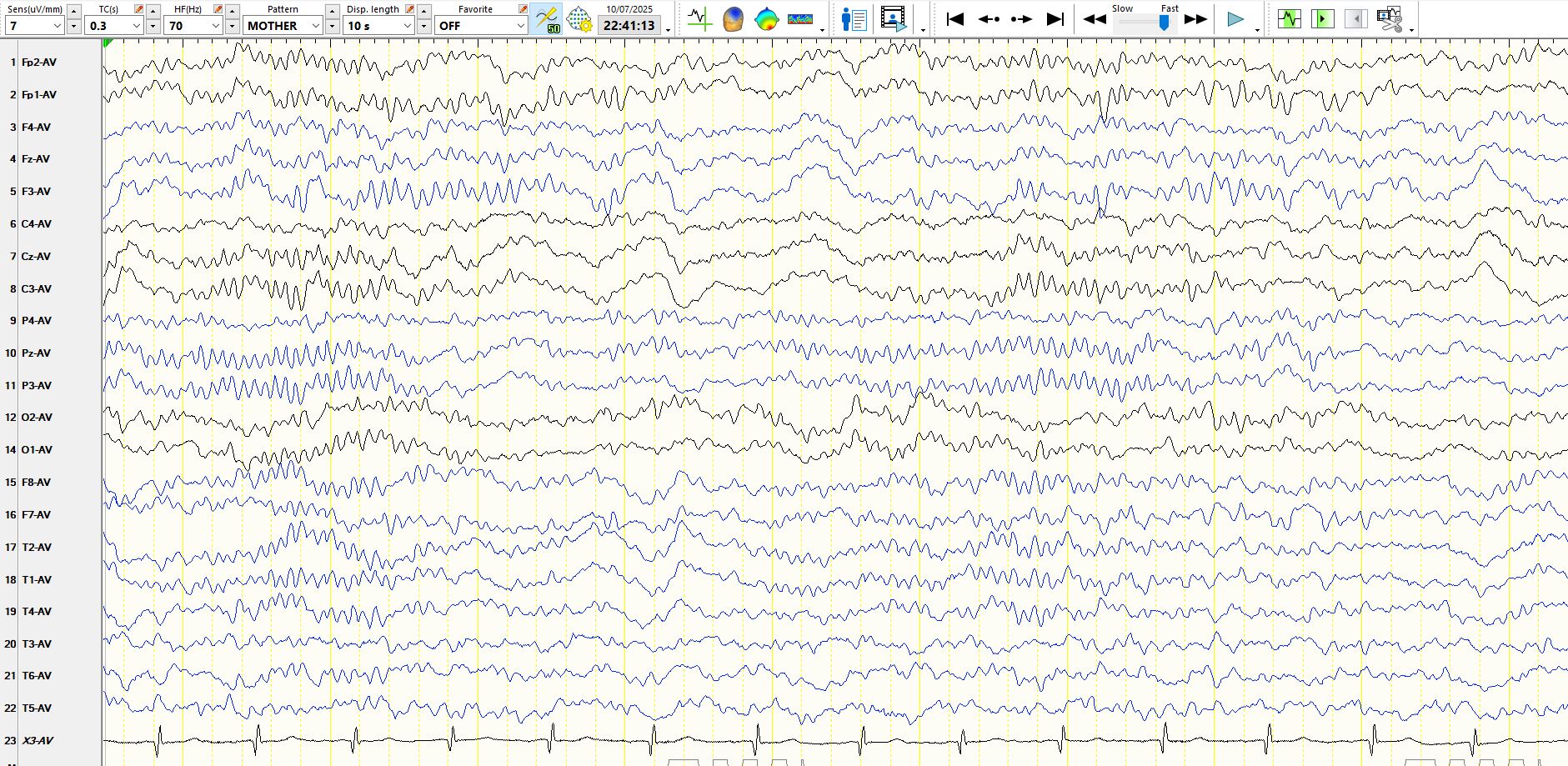
Figure 21:
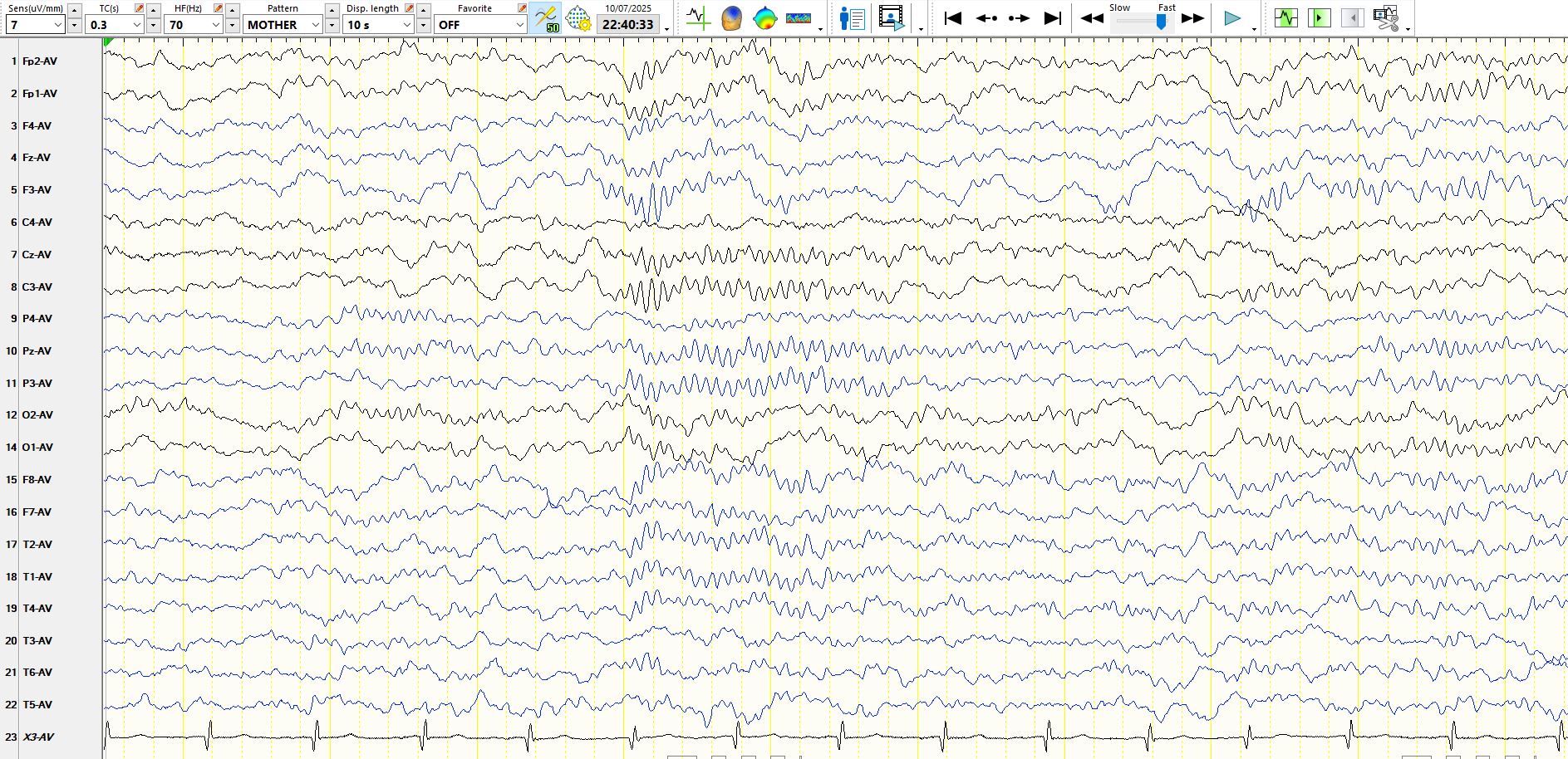
Figure 22:
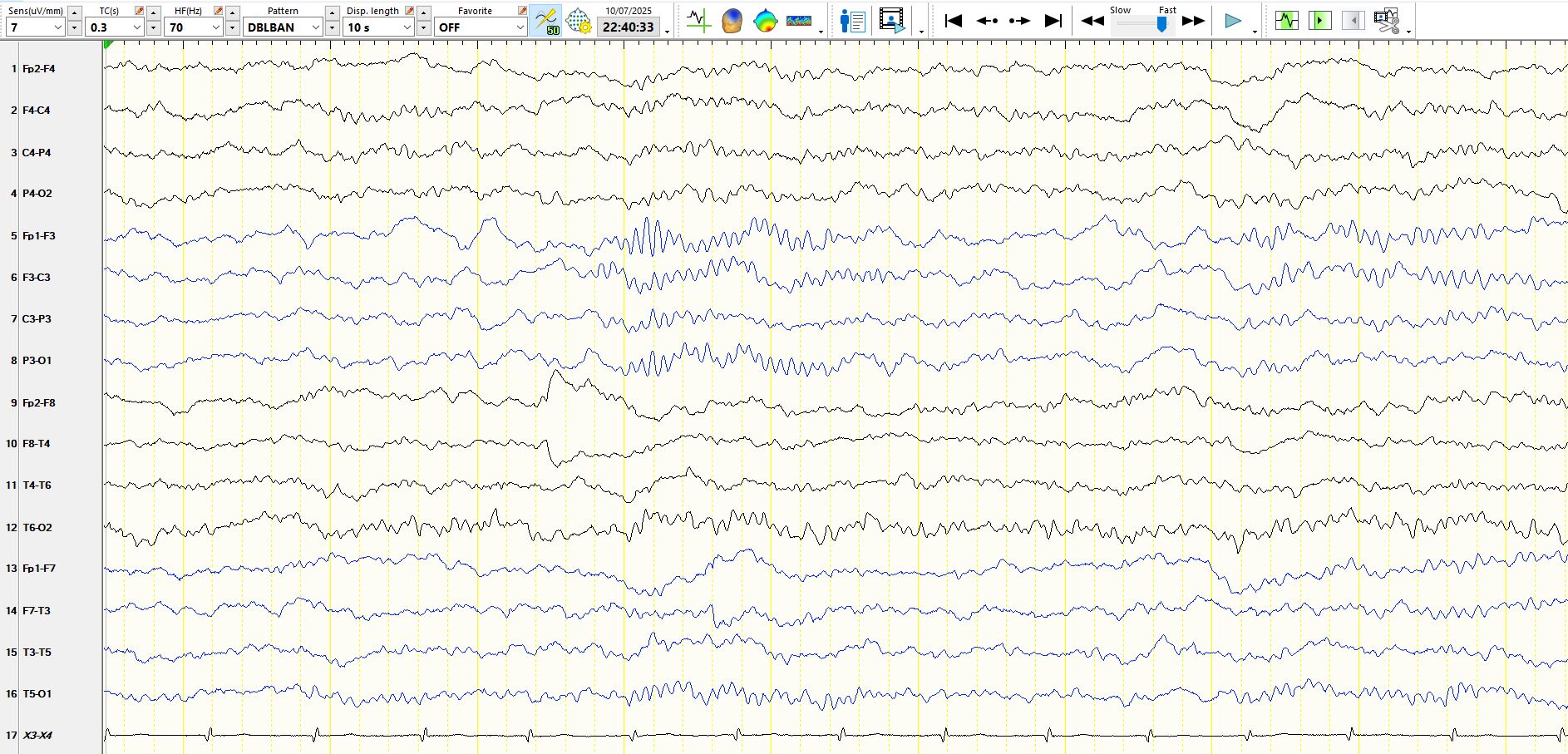
Figure 23:
The recordings performed while awake are normal. In figure 1 there are theta waves at C4-CZ, not seen at C3, but this is not necessarily an abnormality. Figures 4 and 5 reveal normal alpha rhythms, indicating that thalamo-occipital pathways are substantially intact.
In figure 6 there is a relatively inconspicuous vertex wave approximately one second from the end of the page; it is modestly higher in amplitude at C3 than at C4. Spindles appear in the middle of the page, and while these are symmetrical over the temporal and prefrontal regions, there is a marked asymmetry between F4 and F3, C4 and C3 and P4 and P3, lower in amplitude on the right. This is not easily explained by electrode artifacts or placement and, while requiring validation on further scrutiny, this is an important observation. In figure 6 there is a theta wave at FP1-F3-F7 in the middle of the page: given the asymmetry of spindles, it is possible that this is an F wave, normally generated on the left, but not generated on the right. This probability is substantially augmented by the temporal association between this wave and the spindle discharge.
Figure 7 demonstrates that the asymmetry of sleep spindles is sustained. Vertex waves can also be seen, some of which are blunt, such as the waves in the first two seconds and two seconds from the end of the page. These are clearly markedly asymmetric, again appearing at C3-F3 but barely at C4-F4. The sharply contoured waves at F3-C3, delineated by the vertical red lines, have a morphology that is compatible with vertex waves and, given the asymmetry of the spindles, other vertex and frontal waves (F-waves) and the particular stage of sleep, it would be prudent to call these asymmetric vertex waves. It is sensible to be conservative with any judgements like these. Recall Red alert or to paraphrase "Thou shalt not over-call".
Figures 11, 13-21 demonstrate a variety of theta waves and delta waves over the left frontal-central region, some of which are sharply contoured. Yet all of these waves, if accompanied by similar waveforms on the right, would be regarded as normal. Hence, given the near absence of spindles in the right central-frontal region, the absence of these waves, which would otherwise be regarded as physiologically normal, is the abnormality. There is severe dysfunction over the right frontal-central region, extending into the right parietal region. The high amplitude sharply contoured theta waves at F4-FP2-C4 in figure 12 and the delta waves in the same distribution in figures 9-13 provide further evidence for dysfunction in this region.
The patient has epilepsy with seizures commencing as focal clonic movements in the left hand. These have been well controlled for a number of years. However, in 2023 the patient had electrical status epilepticus in sleep over the right frontal-central region.
MRI scan:
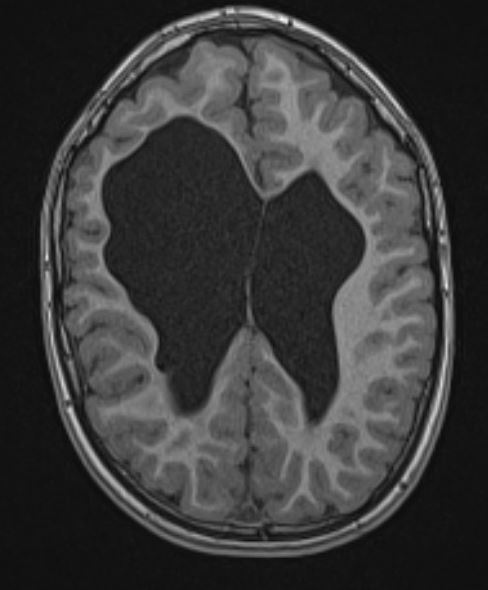
While there is ventricular enlargement bilaterally, the white matter on the right is disproportionately thin and there is disproportionate right ventricular enlargement. The patient has a congenital left hemiplegia related to periventricular haemorrhage in the perinatal period. EEGs performed in another country demonstrated right frontal inter-ictal epileptiform discharges. Magnetoencephalography demonstrated similar findings.